Transcription
Root Cause Analysis(RCA)PROF.DR.SEVAL AKGUN MD, PhDProfessor of Public Health and MedicineChief Quality OfficerDirector, Employee and Environmental Health DepartmentsBaskent University Hospitals Network, TURKEYAdjunct Professor, St. John International UniversityITALY, UNITED STATESPresidentHealth Care Academician Society- Ankara/ TURKEY
WHAT IS ROOT CAUSE ANALYSIS? Root cause analysis (RCA), is a structuralstep by step technique that focuses on findingthe real cause of a problem and deals with it. Root Cause Analysis is a procedure forascertaining and analyzing the cause ofproblems, to determine how these problems canbe solved or be prevented from occurring.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-2
RCA Root Cause Analysis is a tool foridentifying prevention strategies. It is aprocess that is part of the effort to build aculture of safety and move beyond the cultureof blame. In Root Cause Analysis, basic andcontributing causes are discovered in aprocess similar to diagnosis of disease - withthe goal always in mind of preventingrecurrence.8.6.2014Prof. Seval Akgün MD, PhD Workshop onPatient Safety and Quality Management forResidents, June 14-153
RCASince the situation (condition) is usuallyaffected by many factors (physicalconditions, human behavior, behavior ofsystems or processes), several root causeswill usually be found.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-4
RCA1. Inter-disciplinary, involves experts from thefrontline services2. Involves those who are the most familiar withthe situation3. Continually digging deeper by asking why, why,why at each level of cause and effect.4. A process that identifies changes that need to bemade to systems.5. A process that is as impartial as possible8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-5
RCAThe goal is to find out; What happened? Why happened? What can be done to prevent the problem fromhappening again?8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-6
Guiding principles The 5 WHY’s.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-7
Causal factors Are those contributors (human, equipment,processes/measures, system, environment)that if were removed the effect would eitherbe eliminated/prevented or its severity/risk isreduced.Quality Progress, 20048.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-8
RCAmust include:1. Determination of human & other factors2. Determination of related processes and systems3. Analysis of underlying cause and effect systemsthrough a series of why questions4. Identification of risks & their potentialcontributions5. Determination of potential improvement inprocesses or systems8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-9
RCA It is not a single, sharply-definedmethodology; there are many differenttools, processes, and philosophies of RCAin existence. However, most of these can beclassified into five, very-broadly defined"schools" that are named here by theirbasic fields of origin: safety-based,production-based, process-based,failure-based, and systems-based.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-10
Avoid attributing causes to .“sever weather”, “operation error”, “externalfactors”, “equipment malfunction”, “act ofGod”, “nursing error”, “low salaries”, “newmanagement”, “staff dissatisfied”, “nonimplementable solutions”, “generalcauses/solutions”, .etc.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-11
Remember.RC and Problem Roots and WeedsIgnoring the weedsCutting the weedsRemoving the rootsImproving the soil8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-12
ROOT CAUSE ANALYSIS STEPSThree main steps:1. Investigation Data Collection Causal Factor Charting2. Analysis Root Cause Identification Root Cause Prioritization3. Recommendations and Implementation Display of Results Plan of Action8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-13
STEPS IN ROOT CAUSE ANALYSIS PROCESS-1-Step one; The most common element of RCA method variantsincludes asking why today’s situation (condition)occurred. While the answers are recorded. Then ask why foreach answer, again and again. RCA attempts to identifycontributing factors and all causes possible. This allows you to proceed further, by asking why ,until the desired goal of finding the “root” causes isreached.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-14
STEPS IN ROOT CAUSE ANALYSIS PROCESS-2-Next Step; To evaluate best method to change the root cause, so wecan improve our current condition. That is another process, commonly known as: correctiveand preventive action. While we are searching for root cause, we mustremember to review each found cause and factor forcorrection as well, since this can also provide for greatimprovements.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-15
GENERAL PROCESS FORPERFORMING RCA1. Define the problem.2. Gather data/evidence.3. Identify issues that contributed to the problem.4. Find root causes.5. Develop solution recommendations.6. Implement the solutions.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-16
DISADVANTAGES OF RCAThis method, presupposes a single sourceof the problem. In reality, the situationmay be more complex8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-17
ROOT CAUSE ANALYSIS TOOLS1.2.3.4.5.6.5 WhysBarrier AnalysisChange AnalysisCausal Factor Tree AnalysisFailure mode and effects analysisFish-Bone Diagram or Ishikawadiagram7. Pareto Analysis8. Fault Tree Analysis8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-18
TOOLS USED IN RCA9. Surveys10. Histograms (Frequency Charts)11. Flowcharts12. RC Map13. Prioritization Grid14. RC Summary Table15. Trend Charts8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-19
RC Investigation Do NOT answer:– What should have happened?– What didn’t happen? Answer:– What did happen?– How did it happen? Be OBJECTIVE! Avoid: should, not, error, must, inapprop., etc.8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-20
RC Analysis Answer “WHY it happened?” Compare with “what should havehappened?” Answer “why it did Not happen?” Do NOT answer “how Can I fix it?” Think of the environment as well! Subjectivity is OK! Apply different tools8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-21
SUMMARY OF ROOT CAUSE METHODSOccurrenceYesUse all applicable analyticalmodelsFORObscure causeOrganizational Behavior BreakdownComplex barriers and controls(Procedure or AdministrativeProblems)Multi-faced Problems with longcausal factor chainsPeople ProblemsThorough analysis of both8.6.2014causes and corrective actionSerious or complexNoUse scaled down methods prinformal analysisUSEChange Analysis(Use concept for all cases)Barrier AnalysisEvents and causal factorcharting and/or MORTHuman Performance Evaluationand/or MORTKepner-Tregoe ProblemProf. Seval Akgün MD, PhD Workshopon Patient Safety and QualitySolving and DecisionManagement for Residents, JuneMaking14-22
RC Recommendations 8.6.2014Tie action to learningObjective is to remove or correct RCMust be practical, operational and realisticChoose best recommendations!Subjectivity is OK!Be careful of consequences!Check with IO/RC occurrenceProf. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-23
JCAHO’s RCA Worksheet 1/3 Identifying information Team members What happened?– What?– When?– Where?– Who?– How?– Who else?8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-24
JCAHO’s RCA Worksheet 2/3 Why did it happen?– What human factors contributed?– What process issues contributed?– Were there Info Mgt issues?– Were there environmental issues?– Were there leadership issues?– Were there any uncontrollable factors?8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-25
JCAHO’s RCA Worksheet 3/3 Risk Reduction Strategies/Recom.– What strategies to prevent recurrence?– How will these strategies be measured?– When will all strategies be fullyimplemented?– Who will carry out the implementation?– How will the effectiveness of thesestrategies be monitored?8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-26
Remember .to close the loop!Measure—ID Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-27
CASE STUDY-PATIENT FALLProf. Seval Akgun, MD, PhDProfessor of Public Health and MedicineChief Quality Officer, Baskent University HospitalsNetworkAdunt Professor, Oklahoma University School of PublicHealth17.07.2017Prof. Dr. Seval Akgun, MD, PhD28
Steps in making an RCA(ROOT CAUSE ANALYSIS)1. Flow chart of the process2. Formulate a team3. Brainstorming for causes4. Do affinity diagram5. Draw cause and effect diagram6. Find Root Cause by exclusion7. Do PARETTO Chart8. Find solutions9. Put Action Plan10. Prevent Failure (Control Spread Sheet)
ROOT CAUSEANALYSISTITLE OF INCIDENT:TYPE OF INCIDENT:TEAM LEADER:TEAM MEMBERS:Patient Fall
SOLUTIONS must:1. Solve the causes2.Practical3.Satisfy all4.Prevent Reoccurrence
BRAINSTORMING1. Lack of Staff2. Poor Communication3. Lack of training4. Bed/chair broken5. Side rails broken6. No enough strategies7. Side rail not applied8. Failure to monitor9. No regular checking10. No closed Monitoring11. No restraint fixed12. Bad quality13. No Budget
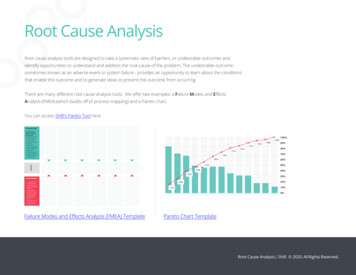
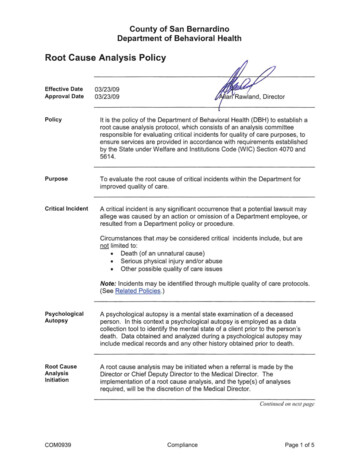
AFFINITY DIAGRAMManpowerMachine Lack of Staff Bed/ChairBroken Side rails notapplied PoorCommunication Side RailsBroken Failure tomonitor Lack of Training Low Quality No regularchecking No enoughstretcherMethodMeasurementMaterials No closed Monitoring No Restraintfixed Bad QualityMiscellaneous No Budget
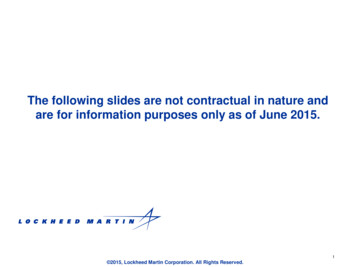
FLOW CHARTPatient AdmittedYesManageNoClose MonitoringNeedRestraintNoYesRestraintYesNoPatient Fall
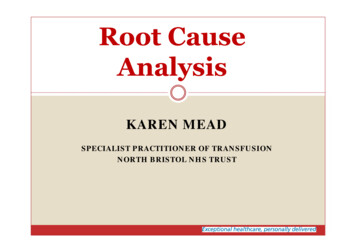
CAUSE AND EFFECT DIAGRAMManpowerMethodMachineSide rail not appliedLack ofStaffPoorCommunicationNo enoughStretcherBed/ChairBrokenFailure to monitorNo regular checkingLow QualityLack ofTrainingSide railsbrokenPatient FallNo Restraint FixedNo closedMonitoringNo budgetBad QualityMeasurementMaterialsMiscellaneous
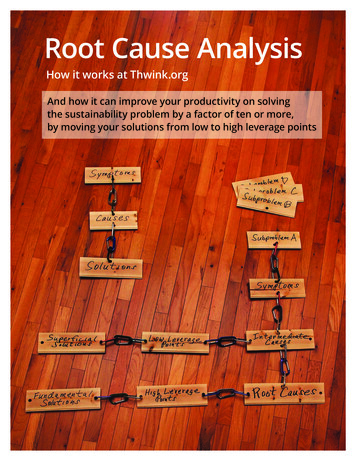
Weighted SelectionTeam MembersItemsAysha Jolly SynRoseTot%alJennRank1. Lack of Staff21243122412. Lack of communication2122181623. Lack of training forrestraint002013644. No frequency assessment bystaff0402061235. No close monitoring2221281626. Bed was little up000000067. Bed was not locked200002458. Restraint was not applied222281629. Bed was broken000000610. Lack of knowledge for0
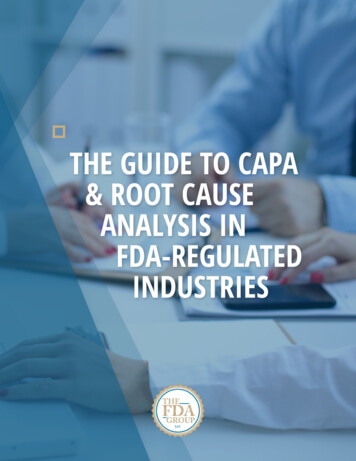
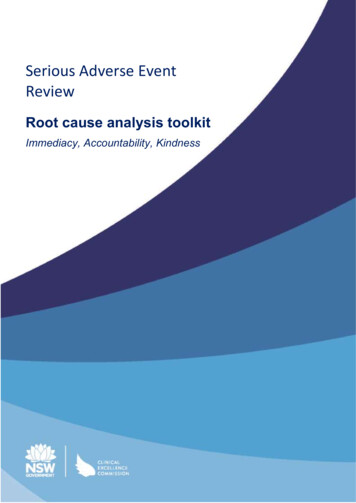
Paretto chart100%3012%2575%2016% 16% 16%other1512%series 2series 1106%6%4%50%0Lack of staffLack ofcom m unicationNo closem onitoringRestraint notappliedNo frequentassessm entLack of trainingLack ofknow ledgeBed w as notlocked
ACTION PLANITEMHire Enough StaffRESOURCES Budget Staffing planWHOACTIONSTIMEFRAME Finance department DON Approving the staff byDON & Administration6 monthsDON & AdministrationApproving the staffing plan6 monthsMEASURE OFRESOURCES 80% of staff areavailableClose Monitoringduring patientmobilizationManpowerTo have restraintmaterials Restraint material Budget for purchasingPurchasingDepartmentApproving the restrain byAdministration1 monthRestraining materialsare available The present policy ComputerHead nurseHDU directorTo add how to discover thatpatient is liable for fallPatent criteria for restrain1monthAvailability andapplication of the policyTo review therestrain policy 80% of staff areavailable
CONTROL SPREAD SHEETVARIABLESSTANDARDWHODISCOVERSHOW TODISCOVERACTIONS TO BE DONERESPONSIBLEPERSONPatient liable tofall from dialysisbedPatient should notfallAssigned NurseDuring close monitoring Informed attending physicianto write restrain order Restrain the patientHead Nurse, and nursein chargeRestrainmaterials are notavailableRestrainmaterials to beavailableHead nurseDuring checking thestore inventory To write DR to ware house To barrow from ICUHead nurse
NURSİNG DEPARTMENT: ROOT CAUSE ANALYSİSUnits involved:Hemodialysis UnitOVR date: 20 August 2009Date of Meeting: 31 August 2009 atCommittee members:1. Attending HdU Staff2. Staff Nurse3. Head Nurse4. Doctor5. Biomed6. Quality Member7. Quality Director Prepared by:Submitted to:
Questions? Comments?17.07.201741Prof. Dr. Seval Akgun, MD,PhD
17.07.2017Prof. Dr. Seval Akgun, MD, PhD42
8.6.2014Prof. Seval Akgün MD, PhD Workshopon Patient Safety and QualityManagement for Residents, June 14-43
WHAT IS ROOT CAUSE ANALYSIS? 2 Root cause analysis (RCA), is a structural step by step technique that focuses on finding the real cause of a problem and deals with it. Root Cause Analysis is a procedure for ascertaining and analyzing the cause of problems, to determine how these proble