Transcription
Emergency Manual, Processes andGuidelines for Obstetric AnesthesiaObstetric AnesthesiologyDepartment of Anesthesia, Critical Care and Pain MedicineBeth Israel Deaconess Medical CenterVersion 1.01
PrefacePrefaceDivision of Obstetric Anesthesia in the Department of Anesthesia, CriticalCare and Pain Medicine at Beth Israel Deaconess Medical Center wascredentialed as a CENTER OF EXCELLENCE by Society for Obstetric Anesthesiaand Perinatology in 2019.The division had been led by our extraordinary founders Dr. Nancy Orioland Dr. Phil Hess for 40 years.The cognitive aids contained within this emergency manual concentrateour institutional tradition and achievements along with significant contributionsfrom our young star physicians. It contains recommendations as well asdescriptions of safety and standards. The recommendations are advisory innature, informational in content and are intended to assist anesthesiologists inproviding safe and standardized care in Obstetric Anesthesia.Material contained in this publication is open to the public and may bereproduced, fully or partially, without permission.All content subject to change, updates and addition.Yunping Li, MD2
ContentsPart I. General IntroductionPART V. Anesthesia For Cesarean DeliveryImportant Phone Numbers 5Medications in Obstetric Anesthesia 6OB Anesthesia Dosage Cookbook 8Tranexamic Acid Protocol 9Conversion of Labor Analgesia for CD 52Spinal Anesthesia for Cesarean Delivery 53General Anesthesia for Cesarean Delivery 54ERAS After Cesarean Delivery 56Anesthesia for External Cephalic Version 58Anesthesia For EXIT Procedure 59Uterotonics 60PART II. Obstetric EmergenciesACLS in Pregnant Women 13Amniotic Fluid Embolism 15Caring parturients with Preeclampsia andEclampsia 17Anesthesia Set Up for Placenta Accreta 19Monitoring During Obstetric Hemorrhage 21Transfusion Guidelines 22Fetal Distress and Intrauterine Resuscitation 23Shoulder Dystocia, Cord Prolapse andUterine Inversion 24Maternal Early Warning System 26PART III. Evaluation and AssessmentEvaluation of Hemorrhage Risks (H Scores) 28Blood Bank Type Screen and Crossmatch 29NPO Guidelines 30Anesthesia Consult 31Transition of Care 33PART IV. Labor AnalgesiaTest Dose 35Labor Epidural Analgesia 37Labor CSE Analgesia 39PCA for Labor Analgesia 41Epidural Morphine following Vaginal Delivery 43Recipes for Labor Analgesia 44Breakthrough Pain Algorithm 45Management of Failed Epidural 46Management of Pruritus fromLabor Analgesia 48Vacuum Delivery and Forceps Delivery 49Delivery of Twin 50PART VI. Postpartum CareCaring Patients after Neuraxial Morphine 62Treatment of Pain after Cesarean Delivery 65Treatment of Pruritis after Cesarean Delivery 66Treatment of Nausea and Vomiting after CD 66Treatment of Hypothermia after CD 67PACU Flowchart 68PART VII. High Risk ObstetricsCardiac Patients in Obstetrics 70Cardiac Parturients – Labor Analgesia 72Cardiac Parturients – Vaginal DeliveryEpidural Titration 73Cardiac Parturients – Anesthesia for CD 74Caring Parturients with Opioids Use Disorder 75Caring Parturients Who are on Anticoagulants 77Anesthesia Consideration for Pregnant WomenUndergoing Non-Obstetric Surgery 78PART VIII. Anesthetic ComplicationsManagement of Intrathecal Catheter 82High Spinal or Total Spinal 83Local Anesthetic Systemic Toxicity 84Postdural Puncture Headache 85What the Patient Needs to Knowafter a Dural Puncture 86Post Epidural Blood Patch Instructions 87Acknowledgment 883
PART IGeneral InformationqqqqImportant Phone Numbers 5Medications in Obstetric Anesthesia 6OB Anesthesia Dosage Cookbook 8Tranexamic Acid Protocol 94
Important Phone NumbersBlood Bank EastBlood Bank WestBlood Bank Resident667-4480754-4330p 30003Anesthesia Office (W)Anesthesia Office (E)754-2675667-3112Holding area -ShapiroHolding area – FeldbergHolding area – West667-0200667-5663754-3100ICUFICU FinardSICU A CC6SICU B CC6T/SICU CC5MICU AMICU &D Anesthesia TechL&D nursing stationL&D OR AL&D OR BL&D OR C (Anesthesia)L&D OR C (Nurse)p 31047667-2295667-2354667-2455667-2273667-2525OB Anesthesia OfficeOB Anesthesia Consult667-3077667-3353OR front desk – EastOR front desk -West667-2411754-3000PACU FeldbergPACU Shapiro phase IPACU Shapiro phase IIPACU West667-3905667-0300667-4790754-2800PharmacyEast main667-4247West main754-3808Pharmacy administrator on callP 92428RadiologyCT – West754-2568CT – East667-5711MRI – West754-2099INR West754-2663IR West754-2552IR East667-2103RemoteCath Lab holdingCath Lab rm 6Cath Lab rm 7ECT632-7447632-7476632-7477632-8355Stat LabEastWestABG, East667-5227754-3230667-3131Workroom – FeldWorkroom – ShapiroWorkroom – West667-4481667-3432754-3098CombosBlue BellEpidural PumpEpidural CartsL&D utility roomL&D restroomOB Call room (Attending)OB Anesthesia OfficeWorkroom3123112331231397512345234123453125
COMMONLY USED MEDICATIONSIN OBSTETRIC ANESTHESIAAzithromycin 500mg, diluted in 20ml of NS/LR, infuse slowly over 1 hour. 4mg of ondansetron IV before infusion due to significant nausea and vomiting Indications: intrapartum cesarean section, spontaneous rupture of membranesReference: NEJM 2016; 375:1231-1241Bicitrate 30ml per container PO, before epidural placement and before cesarean section3% Chloroprocaine Alkalization of chloroprocaine: in a 30-ml syringe, add 2ml of 8.4% bicarbonateto 20ml of preservative free (PF) 3% chloroprocaine Use for emergent cesarean section or for forceps delivery STAT Cesarean Kit: prepackage in OB Anesthesia Office:(1) 3% chloroprocaine (1) 8.4% bicarbonate (1) 30ml syringe (1) blunt needle.Replace it after use.Dexmedetomidine Dilute 200 mcg in 20 ml of NS, final concentration 10 mcg/ml. Indications:- Severe shivering after delivery: 10 mcg IV, may repeat up to 30 mcg- Severe pruritus associated with epidural fentanyl, see separate chapterReference: SOAP annual meeting abstract 2019Ephedrine Premixed by pharmacy, 5mg/ml Historically, ephedrine was used as the “Gold standard” for spinal hypotension. Higher placental transfer than phenylephrine; it can cause clinicallyinsignificant fetal acidosis. Since late 1990s, used as a second line medicine for maternal hypotension.Reference: Am J Obstet Gynecol 1968;102:911 Anesthesiology 2009; 111:506-12Epinephrine Add 250 mcg to 150 ml premixed bupivacaine/fentanyl epidural solution; finalconcentration of epinephrine will be 1.67 mcg/ml Add 5mcg/ml of epinephrine into 2% lidocaine for cesarean section Mechanism: alpha -2 synergic effect, alpha-1 vasoconstriction to prolong theduration of anesthesia and decrease systemic absorption.Reference: J Anesth Perioper Med 2019; 6:1-72% Lidocaine Alkalization of lidocaine: in a 30-ml syringe, add 2ml of 8.4% bicarbonate to20ml of preservative free (PF) 2% lidocaine For cesarean section, add 5mcg/ml of epinephrineMagnesium 2g/hr as maintenance dose For preeclampsia, continue magnesium for entire cesarean delivery For fetal neuroprotection, discontinue magnesium after deliveryReference: The Magpie Trial. Lancet 2002;359:1877-906
COMMONLY USED MEDICATIONSIN OBSTETRIC ANESTHESIAMorphine PFNitroglycerine 0.5mg/ml for spinal use; 1mg/ml for epidural use Pre-made by pharmacy, store at 4 Indications: Cesarean delivery- spinal 250mcg, epidural 3mgLabor CSE for dysfunctional labor – spinal 100 mcgS/p 3rd degree vaginal laceration repair – epidural 2mg Refer to separate chapters for details 400mcg/ml, light sensitive. Kept in Omnicell the same drawer with oxytocin.Dilute to 40 mcg/ml or 100 mcg/ml. Dose: 80-100 mcg IV, may repeat, titrate to effect Indications: cervico-uterine relaxation, uterine inversion, difficult extraction atcesarean deliveryReference: Am J Obstet Gynecol 1998; 179:813Phenylephrine Pre-made by Pharmacy, 100 mcg/ml Indications: first line medication for maternal hypotension Phenylephrine use is associated with a decrease in maternal cardiacoutput, but the clinical significance is not clear Infusion 0.5-0.7 mcg/kg/min or bolus 100mcg, titrate to effectReference: Anesth Analg 2012; 114:377Terbutaline 1mg/ml, use 0.25mg SC, administrated by L&D nurse Indication: Tachysystole contraction with associated FHR changesBefore external cephalic version (ECV) at Obstetrician's discretionACOG Practice Bulletin No. 106Tranexamic acid 1 gram (10ml), infuse over 10 min Treatment of postpartum hemorrhage (PPH) after vaginal or Cesarean delivery Prophylaxis in patients at high risk for PPH, or women with hypertensivedisorder or asthma Discourage use of TXA for prophylaxis in low risk women Exclusion: Hx of DVT/PE/MI/CVA, metastatic neoplasm, or acquired colorblindness. Decreased dose (5mg/kg) for renal failureReference: NEJM 2018; 379:731-42.UterotonicsLancet 2017;389:2095-16 Including oxytocin, methylergonovine (Methergine), carboprost (Hemabate),misoprostol (Cytotec) and calcium chloride Refer to separate chapter for detailsYunping Li, MD7
OB Anesthesiadosage aine 2mgFentanyl25mcgBupivacaine 11.25mgContents:Contents:Premixed in OmnicellMix 0.25cc of Fent (50mcg/cc) with0.8cc of Bupivacaine (0.25%)Mix0.5cc of Fent (50mcg/cc) with1.5cc of Bupiv 0.75% (hyperbaric)May also be mixed withpreservative free (PF) morphine0.25mg (0.5cc)EpiduralEpiduralBupivacaine 0.04% Fentanyl1.67mcg/cc.May add 0.25cc of epinephrine to150 cc bag (1.67 mcg/cc).Lido 2% x 15-20 cc Fent 100 mcg (2cc)Top up: 10-15 cc of BEF or 5-10 cc of0.0625% or 0.125% bupivacaineAdd 50-100 mcg of fentanyl forsynergyAfter delivery: may give Morphine(PF) 3mg (6cc). Lido may be replacedwith: 0.5% bupivacaine orChloroprocaine (CPC3%)BicarbonationUterotonic agentsContents:Contents:LidocaineCPC 3%Bupivacaine(will precipitate)Drug10cc10cc10ccInject divided doses (3-5cc at a time)Oxytocin: 20 IU in 1L of LRBeware hypotensionHCO3 Methergine 0.2mg IM not IV1ccBeware hypertension1ccHemabate 250µg IM or0.1ccIntrauterine not IVBeware bronchospasmCytotec (misoprostol) 1 mg PR8
Tranexamic AcidBackground: Obstetric hemorrhage is the leading cause of maternal mortality worldwide.Despite active management during the third stage of labor, postpartum hemorrhage remains aproblem and is increasing in the United States, primarily due to the increasing incidence ofatony.1 Tranexamic Acid (TXA) is a lysine analogue and works by binding to plasminogen,thereby inhibiting fibrinolysis. TXA has been used for years in the management and preventionof hemorrhage in the surgical setting including cardiac, orthopedic and trauma surgery.2,3Prior studies have established the safety and efficacy of using TXA in the treatment of PPH.More recently, a large multi-center international RCT (The WOMAN trial) demonstrated asignificant reduction in postpartum hemorrhage and death due to bleeding when TXA was usedearly in the treatment of PPH.4 Although there is significantly less data, a few of other smallstudies have demonstrated its efficacy in preventing postpartum hemorrhage in patients atboth average or increased risk when given either prior to or immediately after delivery incesarean deliveries.5,6 Although less well studied, TXA has also been used to prevent PPH invaginal delivery.7 Despite concerns for potentially increasing thromboembolic events, no studyto date has indicated any increased risk in gravid patients receiving TXA. Given this data, ourgoals are outlined below.Goals:1. To reduce the incidence of postpartum hemorrhage in patients at high risk forhemorrhage due to known risk factors2. To reduce the severity of postpartum hemorrhage once a patient has been identified ashaving a hemorrhage (EBL 500 ml in vaginal delivery or 1000 ml in Cesarean delivery)Clinical Practice:1. Prophylactic use: Consider prophylactic use in cesarean or vaginal delivery with patientsat increased risk for hemorrhage (see criteria below), especially in circumstances whereuterotonics may be contraindicated. Discuss possible use at briefing or at teammeeting.2. Therapeutic use: Consider use when patient has been identified as having ahemorrhage. Team agreement prior to administration.9
Method of administration:Dosage: 1 gram given intravenously over 10 minutes. Possible methods of administrationinclude 1g diluted into 10 ml of normal saline or 1g diluted into 100 ml of normal saline.Timing: Administer immediately after delivery of baby in either vaginal or cesarean delivery,or when hemorrhage has been identified. Consider redosing 1g after 30 minutes incontinuing hemorrhage. Consider infusion (5mg/kg/hr) if prolonged bleeding period isexpected.Side effects:Minor: nausea, vomiting, GI upset, headaches, dizziness, hypotension, color blindnessMajor: thromboembolic complications (PE, DVT, MI), seizure, anaphylaxisAt increased risk for hemorrhage: Abnormal placentation (previa, accreta)PolyhydramniosHistory of prior postpartum hemorrhageMultiple gestationGrand multiparityChorioamnionitisFetal macrosomia (fetal weight 5000 g)Morbid obesity (BMI 40)Known coagulopathyRetained placentaSuspected placental abruptionProlonged inductionContraindications: History of thromboembolic disease (DVT, PE or CVA)History of ischemic heart diseaseKnown disorder of hypercoagulability (ex. Factor V Leiden)Prior reaction to TXA10
Relative contraindications:OliguriaReferences1. Incidence, risk factors and temporal trends in severe postpartum hemorrhage. Kramer S, Berg C,Abehmaim H, Dahhou M, Rouleau J, Mehrabadi A, Joseph KS. American Journal of Obstetrics andGynecology 2013. Nov 1; 209(5):449.e1-449e.72. Efficacy of tranexamic acid on surgical bleeding in spine surgery: a meta-analysis.Cheriyan T, Maier SP 2nd, Bianco K, Slobodyanyuk K, Rattenni RN, Lafage V, Schwab FJ, Lonner BS,Errico TJ Spine J. 2015 Apr 1; 15(4):752-61.3. CRASH-2 trial collaborators, Shakur H, Roberts I, Bautista R, Caballero J, Coats T, et al. Effects oftranexamic acid on death, vascular occlusive events, and blood transfusion in trauma patients withsignificant hemorrhage (CRASH 2): a randomized placebo-controlled trial. Lancet 2010; 376:23–32.4. WOMAN Trial Collaborators. Effect of early tranexamic acid administration on mortality,hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): aninternational, randomized, double-blind, placebo-controlled trial. Lancet 2017; 389:2105–165. Randomized controlled trial of tranexamic acid among parturients at increased risk for postpartumhemorrhage undergoing cesarean delivery. Sujata N, Tobin R, Kaur R, Aneja A, Khanna M, Hanjoora V.International Journal of Gynecology and Obstetrics. 2016; 133:312-315.6. Novikova N, Hofmeyr GJ, Cluver C. Tranexamic acid for preventing postpartum haemorrhage.Cochrane Database of Systematic Reviews 2015, Issue 6. Art. No.: CD007872. DOI:10.1002/14651858.CD007872.pub3.7. Gungorduk K, Asicioglu O, Yildirim G, Ark C, Tekirdag AI, Besimoglu B. Can intravenous injection oftranexamic acid be used in routine practice with active management of the third stage of labor invaginal delivery? A randomized controlled study. American Journal of Perinatology 2013;30 (5):407–13.Phil Hess, MD11
PART IIObstetric EmergenciesqqqqqqqqACLS in Pregnant Women 13Amniotic Fluid Embolism 15Caring parturients with Preeclampsia and Eclampsia 17Anesthesia Set Up for Placenta Accreta 19Monitoring During Obstetric Hemorrhage 21Transfusion Guidelines 22Fetal Distress and Intrauterine Resuscitation 23Shoulder Dystocia, Cord Prolapse andUterine Inversion 24q Maternal Early Warning System 2612
ACLS IN PREGNANCYCardiac arrest in pregnancy follows the SAME algorithms and principles in AHA Guidelines,but has a few IMPORTANT DIFFERENCES, which will be highlighted hereCHEST COMPRESSIONS ARE IDENTICAL (no longer recommended to go higher), CODEMEDICATIONS ARE SAME DOSAGE, DEFIBRILLATION VOLTAGE IS IDENTICAL AS NONPARTURIENTS.REMEMBER TO CALL FOR HELP, CALL FOR A CODE BLUE AND OB EMERGENCY, which will alertOB staff and NICU, as a STAT Cesarean delivery is a likely outcome.Location of Code Cart: Alcove between room 7 and 8CONTINUOUS LEFT UTERINE DISPLACEMENT (LUD) IS ESSENTIAL TO MINIMIZE AORTOCAVALCOMPRESSION—WHICH RENDERS CPR INEFFICIENT. Continuous MANUAL LUD is likely the bestform of LUDPrefer IV’s ABOVE the diaphragm since venous return is hinderedPlace lateral defibrillation pad below breast tissueBefore administering a shock consider removing fetal monitors if it can be done quickly, do notdelay shock for that concernIf patient is on Magnesium, d/c the Magnesium and strongly consider administrating calciumPrepare to face a DIFFICULT AIRWAY IN PREGNANCY. First attempt by senior provider with asmaller ETT (6.5)If no ROSC after 4 minutes, call for a STAT Cesarean delivery ON SITE.Baby’s delivery will improve mother’s hemodynamics and chances for ROSCDelivery within 5 minutesAssess possible etiology of arrest. Hypoxemia should be considered as a cause, O2 reserveslower (LOW FRC) and the metabolic demands are higher in the pregnant patient.13
Etiology ABCDEFG:Anesthesia complications: high/total block, hypotension, airway loss, aspiration, respiratory depression, LASTAccident: trauma, suicideBleeding: massive hemorrhage, coagulopathy, uterine atony, placenta accreta, placental abruption, placentaprevia, retained POC, uterine rupture, surgical (retroperitoneal), transfusion reactionCardiovascular: MI, peripartum cardiomyopathy, aortic dissection, arrhythmias, valve disease, CHDDrugs: oxytocin, Magnesium, drug error, illicit drugs, opioids, insulin, anaphylaxisEmbolic: amniotic fluid, air, PE, strokeFever: sepsisGeneral H’s & T’sHypertension: preeclampsia, eclampsia, HELLPCardiac Arrest in Pregnancy A Scientific Statement from the American Heart Association Farida M.Jeejeebhoy et.al. 6 Oct rculation. 2015; 132:1747–1773Advanced Cardiac Life Support of the Pregnant Patient Chapter 17 Robert A. RaschkeLior Levy, MD14
Amniotic Fluid EmbolismIntroductionA syndrome of 3H’s – Hypoxia, Hemodynamic collapse, HemorrhageLow frequency 1:8,000 deliveries, but High clinical acuity, High mortality condition.Very high mortality (50% will die in the first hour, another 10-20% in the next 5 hours).Overall 40-80% mortality with at least 50% permanent neurological damage in survivors.High vigilance, prompt resuscitation and modern ICU have significantly improved outcomes.EtiologyDisruption of the fetal/maternal interface w/ fetal debris in the maternal circulation causingan abnormal activation of anaphylactoid inflammatory response. AFE during labor (70%),during 3rd stage (10%), during c-section (20%), or even during postpartum. Occasionallyoccurring in 1st or 2nd trimester or during termination of pregnancy.Risk factorsOperative (forceps) vaginal or cesarean delivery, placenta previa, accreta, abruption,meconium, and induction of labor. Other: cervical lacerations, uterine rupture, eclampsia,polyhydramnios, multiple gestation.PathophysiologyPassage of amniotic fluid into maternal blood releases pulmonary vasoconstrictors, causingacute RV and late LV failure, cardiopulmonary collapse, severe hypoxemia; Activation of FVIIand platelet causes DIC, hemorrhage and organ failure.Diagnosis§ AFE remains a clinical diagnosis. AFE causes a SUDDEN change in clinicalpresentation. NOT initially via diagnostic modality such as TEE/TTE.§ Must quickly exclude other possible primary causes such as anaphylaxis, eclampsia,seizure disorder, venous air embolism, PE, total spinal.§ Many patients will initially exhibit sense of doom, anxiety, altered mentation, possiblebronchospasm in 15% only.§Progression to cardiac arrest, PEA, VF, or VT is rapid in severe cases. Gravid patientmay have fetus with terminal bradycardia secondary to poor uterine perfusion.15
Clinical Responses to AFE From an Anesthesiologist PerspectiveCall for Help§ call for code cart, high quality CPR, consider massive transfusion protocol activation.§ Place patient in left uterine displacement (LUD) to reduce aortocaval compression§ Consider early intubation§ Place additional Central Line and arterial access§ Cesarean delivery indicated if no maternal ROSC after 4minutes§ Overall Goals: Oxygenation, cardiovascular support, treatment of coagulopathyEarly Phase: characterized by RV failure.§ Consider TTE/TEE for fluid resuscitation§ Consider norepinephrine, dobutamine, milrinone.Second Phase: characterized by LV failure.§ Avoid fluid overload which exacerbates RV function and thus LV function.§ Pressors: norepinephrine, epinephrine, dobutamine, milrinone or vasopressin.DIC Phase (later): Severe coagulopathy can occur early and late. DIC is present in 83%.§ Aggressive treatment of uterine atony and repair other bleeding sites.§ Blood products in 1:1:1§ TEG guidance for replacement§ TXA and rVIIa are controversialDrugs for cardiovascular support in AFE (RV support)Sildenafil (20mg via NG)Dobutamine (2.5-5.0 mcg/kg/min)Milrinone (0.25-0.75mcg/kg/min)Inhaled NO (5-40ppm)Inhaled prostacyclin (10-50ng/kg/min)IV prostacyclin 1-2ng/kg/minNorepinephrine (0.025-0.5mcg/kg/min)Epinephrine (0.03-0.5 mcg/kg/min)Additional Thoughts§ Post-ROSC mild hypothermia (32-36C for 12-24 hour) treatment is indicated§ Treatment with PVR reduction is indicated- prostacyclin, inhaled NO, sildenafilSociety for Maternal Fetal Medicine (SMFM). Amniotic Fluid embolism; diagnosis and management. Am J ObstetGynecol 2016;215: B16-24Joan Spiegel, MD16
Caring for patients withPreeclampsia (PEC) and EclampsiaReview: Pathophysiology and Clinical Diagnosis of PEC Multisystem disease attributable to endothelial dysfunction Clinically defined by new onset, after 20 weeks gestational age, of hypertension (SBP 140 mm Hg orDBP 90 mm Hg) plus one or more systemic manifestations Early onset ( 34 weeks GA) typically carries greater risk of severe disease and maternal/fetalcomplications Occurrence of seizures not attributable to any other cause Eclampsia (may be a presenting sign)Systemic manifestationsFeatureClinical criteriaProteinuria 300 mg over 24h, or Protein: creatinine ratio 0.3Thrombocytopenia 100,000 / uLRenal insufficiencySerum Cr 1.1 mg/dL, or doubling from baselineLiver dysfunctionTransaminases 2x baselinePulmonary edemaLow pulse OX readingCerebral symptomsUnexplained HA not responsive to medical treatment, orvisual disturbancePotential ComplicationsCardiomyopathyPulmonary edemaSeizureThrombocytopeniaDICIntracranial hemorrhageStrokeRenal failureHepatic injury/ruptureLiver subcapsular bleedingFetal growth restrictionPlacental abruption17
Clinical ManagementObstetric decision-making guidelinesPEC without severe features à expectant management until 37 weeks GA, then IOL (or CD )PEC with severe features, 34 weeks GA OR 34 weeks GA with any clinical instabilityà delivery soon after maternal stabilizationIntrapartum management cornerstones:1. BP monitoring and treatment At least once per hour pre-delivery Target SBP 160, DBP 110 mm Hg. Be aware that excessive lowering BP can cause a rapiddecrease in uteroplacental perfusion. 1st –line therapy: labetalol. 2nd-line: hydralazine, nifedipine2. Seizure prophylaxis – MgSO4 4-6g bolus followed by 1-2g/h infusion (renally cleared; reduce dose if renal insufficiency) Target range: 4.8-8.4 mg/dL Signs of toxicity: loss of DTR (9.6-12 mg/dL), hypotension, respiratory depression (12-18 mg/dL),hypoxia, EKG changes and cardiac arrest (24-30 mg/dL) Treatment of Magnesium toxicity: CaCl2 intravenously3. Mild fluid restriction ( 1 mL/kg/h maintenance during L&D)1. Eclamptic seizure treatment 1st-line: MgSO4 (4g bolus over 5min, then 1g/h infusion) Adjuncts: benzodiazepines, phenytoin Consider alternative causes (LA toxicity, electrolyte derangement) Fetal bradycardia is common due to temporary hypoxemia and hypercarbia, not a necessarilyindication for STAT cesarean deliveryAnesthesia Considerations1. Check platelets prior to neuraxial in any patient with hypertension2. General anesthesia is less desirable due to the risk of severe hypertension/cerebral hemorrhagewith intubation/extubation and possible difficult intubation3. Spinal anesthesia for cesarean delivery is not contraindicated4. Consider early epidural or epidural with dural puncture for labor analgesia if platelet is trendingdown.5. Fluid restriction (preload/co-load not necessary in PEC; judicious crystalloid use in CD)6. Beware Magnesium toxicity, especially if renal impairment7. Beware high risk of postpartum hemorrhage8. Uterotonic agents: Avoid Methergine. Consider Tranexamic acid and calcium chloride in addition toregular uterotonic agents.9. Avoid ketorolac if renal insufficiencyErin Ciampa, MD, PhD18
Acc e a Pe c e a P e a a i nOR PREPARATIONRight side of bedArterial line transducerInfusion pump with large neo stick primedInfusion pump with large norepi stick, not primedInfusion pump with large epi stick, not primedPlasmalyte with blood tubing through Ranger warmerLR with microdrip tubing through gang of 5 (to 20g IV)Left side of bedBelmont rapid infuserPlasmalyte through BelmontSecond Ranger with Plasmalyte with blood tubingExtra equipmentRed hemorrhage folder contains all necessary paperwork.Pre-fill ABG and lab paperworkPatient labels prepped (name, phone extension, date)SuperSTAT stickersBair Hugger X 2 (underbody and upper)Activate PPV on aline waveform on monitorTake head segment off top and put on foot endEnsure RIC kit and CVL kit (MAC line) available in emergency cartPHARMACYWorkroom OmnicellCalcium chloride (5) (may need to call pharmacy 7-4247)50ml phenylephrine & norepinephrineOR OmnicellConfirm Hemabate and methergine available in OR fridge (2 of each)RemindersRe-dose cefazolin with 1.5L blood loss1gm TXA load after deliveryRe-dose TXA if excessive bleeding, consider infusion191
Acc e a Pe c e a P e a a i nFROM BLOODBANKCooler with 4 RBC, 2 FFP to startMassive transfusion protocol, as needed. Change ratio to 1:1 if fibrinogen 300 mg/dlDURING CASEMove regional cart and other equipment out of room after use (create space)Move nursing computer workstation out of roomMove cysto tower out of room when doneOR C has metal cart used for papers / blood coolerMake sure nursing is prepared to weigh lap padsPATIENT PREP16G or 14G peripheral IV (X2)Radial arterial line (better on right but not important)20G IV for infusions (good vein so can be changed for RIC in OR)CSE or CSE - GA, as per plan for individual patientEMERGENCY PHONE #SBlood bank 7-4480 All communication is through the blood runner ONLYMain Pharmacy 7-4247STAT Lab 7-1493STAT lab ABG- 73131Perfusion pager on-call schedule (should put # on board if they step out)20
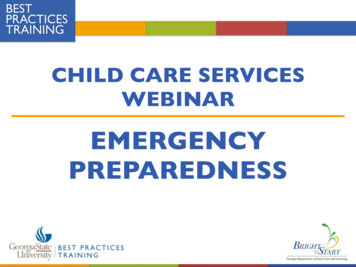
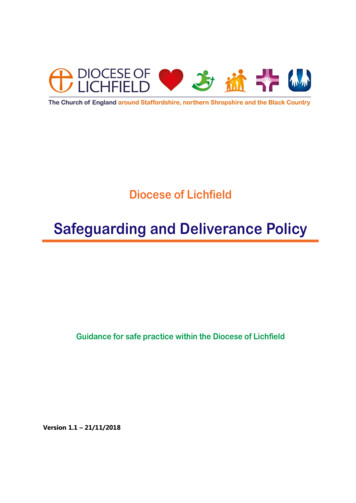
21Phil Hess, MDintubated patients (AA2015;120:76-84) Base excess – withprognostic value (M Colellaet al. SOAP annual meeting,2018) Lactic acid Quantitative Blood Loss(QBL): ask the circulatingnurse Temperature Urine output Ultrasound: volume andcontractility assessment Arterial line PPV – validated in non-Additional Monitoring Tranexamic acid 1g Cefazolin2g q4h, repeat whenEBL 1500ml CaCl2, IVwhen ionized Calcium islow, or with 3rd set ofRBC/FFP UterotonicsMedicationsTransfusion Notify resource nurse Activate Massive Blood PT/PTT/INRTransfusion Protocol Fibrinogen Start 1:1:2, switch to 1:1:1 ABG/VBG with pH, BE, K, iCa,when coags affectedHct, Lactic acid Designate a Blood BankrunnerLabs sent q60 min for massive Designate a person to runPPHBelmont CBC Cell saver – call perfusion Transfusion GuidelinesNote: Consider TEG if coags(PTO)delayed or not matchingclinical pictureLabs sent q30 min for massivePPHLaboratory TestWorkflows for PPH
22
FETAL DISTRESS AND INTRAUTERINE RESUSCITATIONAbnormalities in fetal heart tracing (FHT) pattern can be concerning for progressive fetal hypoxia andacidosis. When a “pattern check” is called, resuscitative measures are taken to increase O2 deliveryto the placenta and umbilical blood flowANESTHESIA TEAM SHOULD GO TO THE LABOR ROOM WITH THE “STAT CESAREAN KIT”(CHLOROPROCAINE 3 % 20 cc, AN EMPTY 30 CC SYRINGE, A BOTTLE OF 8.4% BICARBONATE) IN CASEA STAT CESAREAN SECTION IS CALLEDMaternal positioning Left Uterine Displacement (LUD) to decrease aortocaval compression and improve maternalhemodynamics and utero-placental blood flow “Hands and knees” also used as alternative positionMaternal hemodynamics and oxygenation Correct maternal hypotension: IV Fluids Vasopressors as needed (phenylephrine preferred) Supplemental O2 to be used ONLY to correct maternal hypoxemia. Empirical use of O2 toimprove FHT is not evidence-based, no longer in practice particularly with concerns of COVID-19transmissionTocolysisIn the presence of uterine hyperstimulation (uterine tachysystole leading to non-reassuring FHT) Administer IV fluids Stop oxytocin administration Administer terbutaline 250 mcg subcutaneously No evidence to use tocolytics unless tachysystole ( 5 contractions in 10 min averaged over 30 minperiod) or uterine hypertonus (single contraction lasting 2 min) are presentProgression of labor Cervical exam to check for rapid cervical dilation, descent of fetal head or umbilical cord prolapse In trial of labor after cesarean (TOLAC) patients, CONSIDER uterine rupture (abdominal pain) In the presence of variable decelerations, uterine AMNIO-INFUSION with saline can be considered(bolus or continuous)Obstetrics & Gynecology: November 2010 - Volume 116 - Issue 5 - p 1232-1240 doi:10.1097/AOG.0b013e3182004fa9Intrauterine Resuscitation During Labor GARITE, THOMAS J. MD*; SIMPSON, KATHLEEN RICE PhD, RNC†Clinical Obstetrics and Gynecology: March 2011 - Volume 54 - Issue 1 - p 28-39 doi:10.1097/GRF.0b013e31820a062bLior Levy, MD23
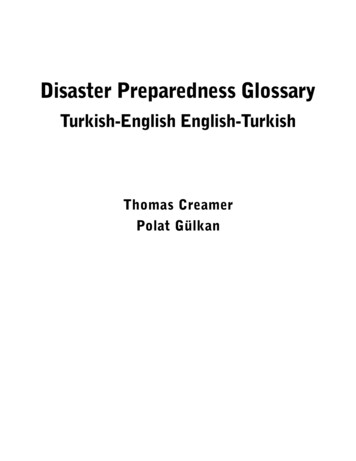
Obstetric EmergenciesShoulder Dystocia5-9% 4000-4500g14-21% 4500-5000gACOG Recommends c/s for 5000g without diabetes, 4500g with diabetes*Diagnosis of macrosomia is impreciseTurtle Sign- Retractionof head against maternal perineumResistance of delivery of anterior shoulder with usual tracti
ACLS in Pregnant Women 13 Amniotic Fluid Embolism 15 Caring parturients with Preeclampsia and Eclampsia 17 Anesthesia Set Up for Placenta Accreta 19 Monitoring During Obstetric Hemorrhage 21 Transfusion Guidelines 22 Fetal Distress and Intrauterine Resuscitation 23 Shoulder Dystocia, Cord Prolapse and Uterine Inversion 24 Maternal Early Warning .