Transcription
TATRC TIMESSeptember 2016 Volume 2, Qtr. 4Dr. Jaques Reifman Wins the 2016Samuel J. Heyman Service to America MedalThe nonprofit, nonpartisanPartnership for Public Service presented eightSamuel J. Heyman ‘Serviceto America Medals‘ (Sammies) on Tuesday, September20, at the Andrew W. MellonAuditorium in Washington,D.C., to remarkable publicservants who are making adifference in their communities and improving the lives ofAmericans and others aroundthe world. One of those recipients was our very own Dr.Dr. Jaques Reifman,Jaques Reifman, a U.S. ArmyBHSAI DirectorMedical Research and Matephoto by Aaron Clamageriel Command Senior Research Scientist and TATRC’sLab Director for the Biotechnology High PerformanceComputing Software Applications Institute (BHSAI).Reifman, who was named as a Samuel J. Heyman ‘Service to America’ finalist, was honored on May 3rd on CapitolHill in Washington, D.C., as part of Public Service Recognition Week. Dr. Reifman was among those distinguishedfinalists being recognized and has officially been presentedthe SAMMIE Medal in the category of Science and theEnvironment for his work on the APPRAISE project.Reifman and his team developed an artificial intelligencesystem, called the Automated Processing of the PhysiologicRegistry for Assessment of Injury Severity known as APPRAISE, for medics to quickly detect if severely injuredpatients in transit are hemorrhaging, improving survival ratesby preparing trauma centers to act immediately upon thepatient’s arrival.Key contributors to Reifman’s APPRAISE team included Maxim Khitrov and Jianbo Liu as well as AndrewReisner, an investigator with the Army’s BHSAI lab, and anemergency room doctor at Massachusetts General Hospital.The Army has received two U.S. patents for the APPRAISE system and is now pursuing Food and DrugAdministration clearance and a licensing agreement with acommercial partner.Gary Gilbert, TATRC’s Operational Lab Director, saidReifman “argued for years that we measure many vital signs,but that we don’t know if the data we are collecting is actually information we need to be sure someone is in criticalcondition.”“He had a vision,” Gilbert said. “He addressed the needfor expediency to help medical personnel in combat.”Reifman said the APPRAISE system offers “an opportunity to save lives on the battlefield” and eventuallycould be of great assistance to emergency medical personnelthroughout the country.“Not too often do scientists have an idea or a dream,and then over time advance the science to take the conceptto deployment and show that it works,” Reifman said. “I’mthankful that I’m here at the Army, which provides longevity in funding and support over time.” Congratulations Dr.Reifman, on this well deserved, high honor!IN THIS ISSUE:REIFMAN RECOGNIZED WITH “SAMMIE” AWARDPage 1OPTMED FIELD EXERCISE AT CGAPage 2OPTMED ATTENDS RIMPAC EXERCISEPage 3TATRC INVOLVED IN SUICIDE PREVENTION MONTHPage 4TATRC TAKES PART IN AIS3 SUMMITPage 5FAREWELL TO MG BRIAN LEINPage 6STEMS & GEMSPage 6MRMC COMMANDER, MG BARBARA HOLCOMB VISITS TATRCPage 7LINKED PROBLEM LIST: ENHANCING ACCESS FOR DOD AND VAPage 8EMPLOYEE SPOTLIGHTS:TATRC WELCOMES JEFF LEVYPage 10EMPLOYEE OF THE QUARTER: KATI WEAVERPage 10NEW TATRC IPASPage 11MMSIC LAB EXPANDS CAPABILITIESPage 12TATRC LEADERS PARTICIPATE IN MHSRSPage 14GOT AN IDEA? AAMTI RAPID INNOVATION FUNDPage 15MMSIC SERVES ON CAPABILITY DEVELOPER TEAMPage 16mHIC TELEHEALTH 2.0 PROJECT AWARDEDPage 17AAMTI PROJECT UPDATE FROM MADIGANPage 18ON THE HORIZONPage 18HTIC COLLABORATES WITH NISTPage 19AAMTI AWARDS ANNOUNCED FOR FY17Page 20TEAM TATRC PRESENTS AT 2016 DHITSPage 21TATRC PAVES THE WAY TOWARDS OPTIMIZING ITS SIMULATED FIELDENVIRONMENTPage 22TATRC SUPPORTS ATARC FEDERAL CLOUD COMPUTING SUMMIT Page 23MHCE-R SYSTEM NOW INCLUDES T2 MOOD TRACKERPage 24A QUARTERLY NEWSLETTER OF THE TELEMEDICINE & ADVANCED TECHNOLOGY RESEARCH CENTER
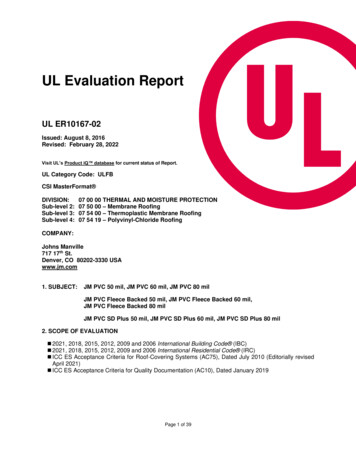
TATRC TIMESSeptember 2016 Volume 2, Qtr. 4OpTMed Lab Conducts 4th Annual FieldEvaluations at CERDEC Ground ActivityDuring the month of August, TATRC’s OperationalMedicine Team spent their weeks setting up and preparing for their annual telemedicine evaluation and exercise. Bymid-month, the entire team had relocated to the CERDECGround Activity (CGA) Range #1 at Joint Base McGuireDix-Lakehurst ( JBMDL), New Jersey, to conduct advancedconcept demonstrations and operational user evaluations ofprototype technologies emerging from TATRC’s executedresearch projects. The Operational Medicine Lab managesapplied research and pre-advanced development projects forPoint of Care (POC) telemedicine and unmanned casualtyextraction and, each year, takes them to the field for evaluationwith soldiers at the CGA facility. CGA provides an excellentenvironment to test and evaluate medical devices, sensors,medical information exchange, and tele-health research anddevelopment prototypes using the latest U.S. Army TacticalCommunications Capability Sets. While this year’s evaluations focused on three major efforts: 1) POC wireless medical sensors, encounter documentation, and tele-health; 2)Enroute-care patient monitoring integrated with commandand control of unmanned casualty evacuation vehicles; and 3)a cloud-based Theater Electronic Health Record (EHR): theprimary focus was on the latter, the feasibility of implementinga cloud-based Theater EHR using service (Army) providedcommon user command and control tactical communications networks. Measured in terms of that objective alone, theentire CGA Telemedicine event was a success.To validate the cloud-based Theater EHR concept,TATRC invited a number of university and industry researchers and other MRMC laboratories previously awardedTATRC managed Phase II SBIRs or other research contracts,to work with TATRC and CGA to integrate and test theirprototype medical information exchange capabilities on theCGA tactical radionetworks. Thesenetworks wereconfigured byCGA engineers toprovide connectivity from battlefieldpoints of care,through enroutecare, to Roles I & IImedical treatmentfacilities (MTFs).Connections weremade from thosepoints of care overMedic provides electronic,tactical radios,medical point of caresatellites, and theencounter documentation.Defense Research& Engineering Network to remote Armed Forces HealthLongitudinal Technology Application - Theater (AHLTA-T)Remote Data Services (RDS) servers developed by PM MC4and located at Fort Detrick and Aberdeen Proving Ground(APG). Patient monitoring data generated by POC vitalsigns sensors and telemetry was transmitted wirelessly viaultra-wideband, tunable narrow band, or Bluetooth technologies to an Army Nett Warrior type Android End User Device(EUD) to be posted to an electronic Tactical Combat Casualty Care (TC3)/DD1380 card. The EUD was connectedto a riflemen radio, which was used to transmit the data overCGA’s implementation of the Army’s Joint Tactical RadioSystem ( JTRS) network and a prototype Cross DomainSolution (CDS) at the Brigade Tactical Operations Center(TOC) to the “cloud-based” RDS AHLTA-T servers at FortDetrick and APG. The prototype CDS enabled unclassifieddata transmitted over the tactical SIPRNET to cross over tothe unclassified military internet where the AHLTA-T serversreside. At the Roles I-III MTFs, a light version of AHLTA-Tcalled Health Assessment Light Operations (HALO), alsodeveloped by PM MC4, was used to input new encountersfor immediate upload to the remote RDS AHLTA-T servers at Fort Detrick and APG. Once all the components wereassembled and network pieces became operational at Range1, the mobile tactical network and the prototype medicalinformation capabilities were moved to more remote rangesfor further testing and evaluation. Not only were points ofcare EHRs able to be posted to the remote RDS AHLTA-Tservers from all points on the exercise battlefield, they couldalso be readily accessed in short order at the Roles I and IIMTFs at JBMDL, and the Role III Combat Support Hospital at Fort Gordon, GA, as soon as they were posted to theMC4 RDS AHLTA-T servers. This was accomplished byusing a thin client (web server) access capability developed byPM MC4 and implemented on both wireless notepads andthe same MC4 laptops at Roles I, II and III as the HALOcapability.Another field evaluation focus area was aimed at assessingthe concept of integrating Command and Control of Unmanned CASEVAC vehicles with patient telementoring during transport on either ground or air CASEVAC platforms. Acombined ground and air unmanned CASEVAC mission wasconducted using a rugged AMBOT Unmanned Ground System (UGS), and the Lockheed Martin’s K-MAX UnmannedAerial System (UAS) Platform for patient transport. Integration of an on-board TEMPUS-Pro telementoring system andNeya’s Unmanned Systems Control Segment (UCS) VerticalTakeoff and Landing Evacuation and Resupply Tactical Interface (VERTI) notepad were performed on both the UGV and2
September 2016 Volume 2, Qtr. 4CERDEC,TATRC TIMESContinued from page 2UAV in order to provideHuman-Computer Interface (HCI) and Command and Control (C2)of simulated casualtyevacuation missions using unmanned systems,Soldiers utilizing UAS & UGV to support expedited CASEVACand to provide a transa simulated CASEVAC mission, as well medical information exchange researchport telemedicine patientprojects in the field with soldiers ismonitoring capability while enroute us- as several radio network architecturessupporting ground to ground, ground to probably the most important activity weing a UCS implemented Telemedicineair, and air to ground medical informado as a lab. We go to CGA to identifyReference Architecture. Arranging fortion exchange using a variety of medical major technical or operational weaka full sized man rated UAS, like the Knesses early during the research phase,MAX, to execute this field evaluation at and mobile devices. Participants at theVisitor Day came from across the enter- before advanced development begins,JBMDL was a major accomplishmentso that development strategies can bemade possible by the material support of prise and included representatives fromJPC-6, USAMMA, USAMMDA, US- adjusted before significant investmentsthe USAMMA PM MEDEVAC.ARIEM, USAARL, USAISR, Marineare made. Over the years, I have seenAt the end of the evaluation,Corps Warfighting Lab, ONR, AFRL,so many new capabilities, already at orTATRC hosted a Visitor’s day demAFMSA, DHA, PEO DHMHS, PEO near full development, fail miserablyonstration to give the broader militarySoldier, PM JOMIS, PM MC4, PMwhen they are first put in the handsmedical community a glimpse of theMEDEVAC, AMEDD C&S MEPDof Soldiers. Only from Soldier-userprevious 3-weeks of operational andand JTAPIC, as well as five US SOfeedback in the field and direct obsertechnical field assessments supportingCOM organizations. A thorough “hotvation of performance on real, tacticalDefense Health Program research innetworks, can you effectively assess thevestments in Operational Telemedicine. wash” discussion was conducted at theend of the day. While comments frompotential of new medical informationVisitors were exposed to a variety oftechnologies for operational use. If, as Ifield scenarios including prototype tech- the participants varied, all agreed theevent was worthwhile and beneficial.suspect, those attending our visitor’s daynologies for telementoring and casualtyOperational Telemedicine Labwent home with an appreciation for thatcare documentation, integrated patientDirector, Dr. Gary Gilbert stated, “Ouraspect of our research, the day was moretelemonitoring & command & controlCGA evaluations of telehealth andthan successful.”of ground and air unmanned systems inRIMPAC Exercise Highlights Value of MultiService, Joint Research CollaborationsPersonnel from TATRC’s Operational Telemedicine (Op T-med) Lab were invitedto attend and observe the “Rim of the Pacific”(RIMPAC) exercise by the Marine CorpsWarfighting Laboratory’s (MCWL) Officer inCharge of Medical Experimentation, LCDRDavid Gribben. TATRC and MCWL areresearch partners investigating Maritime useof telemedicine capabilities. Mr. James Beach,Project Manager for Op-T-med, representedTATRC during the exercise conducted 29-30July 2016 at Camp Pendleton, California.The MCWL objective was to conducta baseline experiment focused on employ-3ment of standard Enroute Care Teams, ShockTrauma Section (STS) Capability, and enhanced Forward Resuscitative Surgical Systemwithin a Marine Expeditionary Force thatis conducting forcible entry operations in adenied environment. Casualty evacuations andresupply were conducted using MH-53E Helicopters and MV-22B Osprey Vertical TakeOff Landing (VTOL) Aircraft, as vehicles ofopportunity. The experiment was designed toidentify the minimum organizational, clinical,and logistical requirements by deployment ofthe lightest possible footprint, for providinginitial care during a forcible entry operation.Contributions from TATRC, such asContinued to page 4Members of a STSreceive instructionon the TempusPro PhysiologicalStatus Monitor.
TATRC TIMESRIMPAC, Continued from page 3loaning of Tempus Pro Physiological Status Monitors,allowed the MCWL to validate operational concepts inproviding real-time patient status information in a MedicalCommon Operating Picture. James Beach stated, “Thereare many common problem sets facing both Services. Ourcollaboration between the MCWL and TATRC, enabledthe Marines to prove the concept for using medical data toinform a [Medical] Common Operating Picture and provide insight into Marine Warfighting Concepts that may beemployed in the Army.”September 2016 Volume 2, Qtr. 4The medical evaluations of RIMPAC were focusedon validation of concepts and not on technical testing offinal solutions. The concept evaluations were not limited tospecific solutions; rather, they supported the overall conceptof a light weight, easily transportable, expeditionary medical capability to support forcible entry operations untillater phases of an operation brings more medical capabilityto bear. The concepts could easily be translated into earlyentry warfighting concepts for Light Divisions in the Army.Some of the research could potentially be further expandedto result in reduced footprints of deployed Army militarytreatment facilities.TATRC Gets Involved in September’s SuicidePrevention & Awareness MonthSeptember has been designated Suicide Prevention andAwareness Month. In 2012, the VA released a SuicideData Report that an average of 22 Veterans are lost tosuicide every day. Suicide prevention is a very difficult taskto undertake, especially when the general public is unawareof the issue in the first place. In order to prevent or “fix” aproblem, one must firstlearn and understandthe problem itself andits causes. By educatingourselves, we are ableto identify the triggersthat can lead someoneto thoughts of suicide,and confront thoseissues as they come,Mr. Tim McCarthy, TATRC’srather than lettingDeputy Director “gives athem accumulate intoset.”something much worse.This problem notonly plagues the military population, but the civilian population as well. A recent Social Media campaign, initiated bythe organization 22KILL, has taken off and includes celebri-Geoff Miller, Nate Fisher, and Jeff Levy participatein Suicide Awareness Month.ties, civilians, Veterans andmore, all working togetherand showing support to raiseawareness for the 22 Veterans a day statistic. The name“22KILL” is meant to grabpeople’s attention and notjust raise awareness aboutVeteran suicide, but alsoTATRC Director, COLto highlight mental healthDan Kral, does dailyissues that can lead to suicide. pushups in his office.These issues stem primarily from conditions such as PTS and TBI, and struggles oftransitioning out of the military.Hashtags can be found with the #22pushupchallenge or#22pushups all over various Social Media Platforms. TeamTATRC worked this September to also raise awareness onSuicide Prevention and TATRC’s Director, COL Dan Kralled the way and encouraged everyone to participate. Teammembers have been “caught in the act” of doing their 22pushups all over our Lab. COL Kral has been known to tellhis staff to “drop and give him a set” before a meeting starts.TATRC has been proud to push the envelope with theirpushups and help in this small way to try to raise awarenesson this very important topic.Don’t ever be afraid to reach out and check in with yourfriends, family and co-workers! It can make all the differencein the world. Please be aware of the countless programs outthere to assist people who are in these dire situations.For the military, if you are experiencing a crisis, or havea friend or family member in crisis, call: 1-800-273-talk(8255) press ‘1’ for the military crisis line or text to 838255.For more information go to: www.militarycrisisline.net.Civilians can contact the National Suicide PreventionLifeline at 1-800-273-8255 or visit the National SuicidePrevention Lifeline at www.suicidepreventionlifeline.org.4
September 2016 Volume 2, Qtr. 4TATRC TIMESTATRC Plays a Part in AIS3 Summit WhereInnovation Takes CollaborationInnovation takes collaboration. That was the message fromthe U.S. Army Materiel Command’s (AMC) top leaderas AMC co-hosted the U.S. Army Innovation Summit 3(AIS3) with the Army Training and Doctrine Command,at the College of William and Mary, School of Education,August 16 – 17 in Williamsburg, Virginia.TATRC’s Deputy Director, Mr. Tim McCarthy andProgram Manager, Mr. Dave Williams, attended the AIS3where TATRC was one of 30 DoD Exhibitors selected toparticipate. This gave Mr. McCarthy and Mr. Williams theopportunity to engage in various discussions with current andformer DoD partners from both military and civilian sectors.These dialogues focused on how TATRC has been an integralpartner spurring development and innovation in various areasof Military Medicine.The event brought together more than 250 leaders fromindustry, academia, DoD and the Army to explore processesto achieve innovation, expand collaboration efforts, and refineinnovation initiatives developed at the first two Army Innovation Summits. The three summits are part of the largerInnovation Campaign, initiated by AMC on behalf of theArmy in 2015.The first summit (AIS1) took place in November of 2015at Redstone Arsenal with representatives from across theArmy with a focus on concepts and requirements. AIS1 identified barriers to innovation and ideas on how to overcomeBG John Cho, Deputy Chief of Staff for Support,MEDCOM, visits TATRC’s Mr. Dave Williams and Mr.Tim McCarthy at TATRC’s Exhibit Booth during theAIS3.them. The second meeting, (AIS2) was held April 4-6, 2016at Aberdeen Proving Ground and focused on reviewing andrefining innovation solutions, assigning ownership/ collaborative partners, and implementing “ActionPlans.”In this third gathering, leaders from acrossthe Army, along with members of industry andacademia, met to examine the Army’s innovationefforts within its mission to equip and provide forthe Soldier. AIS3 provided a cost-effective platform for the Army and other senior governmentleaders to engage key audiences, articulate Armystrategic priorities and serve as a mechanism toestablish critical relationships with academia andindustry leaders for innovation. The event exploredand highlighted different aspects of innovation foran unpredictable global security environment out tothe year 2025 and beyond.General Dennis L. Via, of the United States Army MaterielIn his opening comments, AMC CommanderCommand (AMC) stopped by the TATRC Booth to talkGen. Dennis L. Via said, “It is critical to take a mo“technology and innovation” with TATRC’s Mr. Timment to pause, slow down and ask ourselves are weMcCarthy & Mr. Dave Williams. General Via assumeddoing things right, and more importantly, are weresponsibilities as the 18th commanding general of AMCdoing the right thing. You can’t achieve innovationon August 7, 2012, headquartered at Redstone Arsenal, AL.all at once, it takes time and collaboration.”5
TATRC TIMESSeptember 2016 Volume 2, Qtr. 4USAMRMC & Ft. Detrick Bid Farewell toMG Brian LeinOn Thursday, 28 July, the U.S. Army Medical Researchand Materiel Command (USAMRMC) and FortDetrick Community said “Farewell” to outgoing Commander,Maj. Gen. Brian C. Lein, as he handed over the reins toMaj. Gen. Barbara R. Holcomb, former Deputy Commanding General for Operations, U.S. Army Medical Command(MEDCOM) and Chief, U.S. Army Nurse Corps, during anoutdoor ceremonial Change of Command which took placeon the Blue & Gray Parade Field at Fort Detrick.At the Change of Command ceremony, MG Lein beganby saying: “It’s a great day to be a Soldier,” and went on to say“I’m sad to leave such a great Command, but I am very confident that MG Holcomb will continue to lead this Commandforward.” He concluded with “One Team One Purpose!Conserve the Fighting Strength!”Lein’s tenure at Fort Detrick has undoubtedly been ademanding assignment. A job, Lein notes, that he could nothave successfully accomplished “without the support, dedica-STEMS & GEMS Students Return to TATRC for a Science& Technology Tour!This summer, TATRC was proud to be invitedby USAMRMC’s Strategic Partnership Officeto host once again, two groups of students fromthe Gains in the Education of Mathematics andScience (GEMS) and Science, Technology, Engineering, and Mathematics (STEM) Programs. TheGEMS is an Army-sponsored, summer STEMenrichment program for middle and high schoolstudents with an interest in science & technology.STEMS & GEMS Students visited TATRC for a first-hand lookThe students visited the TATRC team for theirat OpTMed’s drone.annual tour which included an interactive, hands-onexperience in telemedicine. The visiting students werewe hope continues to grow.”able to get up close and personal with our interactive maniAdditionally, the GEMS students were given a tour ofkins that simulate real, life-like gunshot wounds, which wereTATRC’s PITLab facility and met with Mr. Nate Fisher,demonstrated by Mr. Geoff Miller, TATRC’s MMSIC LabTATRC’s Operational Telemedicine Program Manager, whoManager. “Getting a chance to share what we do with thesespoke to the students on Robotics, Unmanned Aerial Systemsyoung scientists is an absolute pleasure,” says Mr. Miller. “They & Unmanned Ground Systems, which included a first-handhave a true and honest curiosity that is infectious, and one thatlook at OpTmed’s Drones. Mr. Fisher explained howMr. Geoff Miller, TATRC MMSIC Lab Manager (Left),explains the use of a tissue task trainer to a group ofvisiting students.the use of Commercial off the Shelf Technology,combined with custom components, can enhance theresearch model and spur innovation. Ms. RebeccaLee, a Biomedical Engineer & Project Officer, alsowith the Operational Telemedicine Lab, explainedthe capabilities of the 3-D Maker-Bot Printer andshowed a prototype that she printed just an hourbefore the tour. She talked about how the benefits ofrapid prototyping in the research and developmentprocess, enables TATRC to transition ideas fromconcept to reality.The TATRC Team enjoyed spending time withthe GEMS students and thanked them for visitingour lab. We hope that this visit inspires the students tocontinue exploring the world of science & technologyand motivates them to pursue their dreams!6
September 2016 Volume 2, Qtr. 4Lein, Continued from page 6tion and passion” of the people workingnot just here at Fort Detrick, but worldwide within the command. Under MGLein’s leadership, USAMRMC played acritical role in the Ebola outbreak training and deployment efforts, and pavedthe way for the development of a Zikavaccine.MG Lein now serves as the newCommanding General at the U.S. ArmyMedical Department Center and School(AMEDD C & S) at Fort Sam Houstonin San Antonio, Texas where he overseesthe formulation of medical organization,tactics, doctrine, equipment and the education and training of medical personnel.TATRC TIMESTaking over for MG Lein is Maj.Gen. Barbara R. Holcomb. MG Holcomb was the Deputy CommandingGeneral for Operations for MEDCOM.She is the first female Commander ofUSAMRMC and also its first Commander to come from the Nurse Corps.MG Holcomb will continue to serve asthe Chief of the Nurse Corps, a positionthat she held before assuming commandat USAMRMC.The TATRC team would like tothank MG Lein for his leadership thesepast two years and wishes MG Leinmuch success in his new role as theCommanding General at the AMEDDC & S, Fort Sam Houston, TX!Former MRMC CG MG BrianC. Lein bids farewell duringthe change of commandceremonyPhoto courtesy of USAMRMCNew MRMC Commander, MG BarbaraHolcomb, visits Team TATRCOn Wednesday, 10 August, new Commanding General of fication in emergency and disaster management from Amerithe U.S. Army Medical Research and Materiel Comcan Military University, and a Master’s in Military Strategicmand (USAMRMC), MG Barbara Holcomb, visited theStudies from the U.S. Army War College in Carlisle, PennTATRC team for a TATRC orientation briefing & overview.sylvania. She is the first female to lead USAMRMC and theMG Holcomb met with TATRC’s senior leadership and keyfirst Commander to be drawn from the Army Nurse Corps.personnel to gain a better understanding about TATRC’sTATRC Warmly Welcomes MG Barbara Holcomb tomany initiatives and core capabilities, as well as how it supUSAMRMC!ports the Command. TATRC Director, COLDan Kral outlined the history and current statusof the organization, as well as where he seesthe direction TATRC is heading in the future,and how it fits into the U.S. Army MedicalCommand mission. After the formal briefingconcluded, MG Holcomb toured the TATRCfacility and had a chance to meet and chat withnumerous TATRC staff.“I am excited to be here, and I am really looking forward to working with all ofyou, learning from you and understanding thecomplexities of all you do,” said Holcomb in hercomments.MG Holcomb assumed command ofUSAMRMC on 28 July. She is a 1987 Distinguished Military Graduate of Seattle University’s Army ROTC where she earned a Bachelorof Science degree in nursing. She earned aNew MRMC CG MG Barbara Holcomb (Left) visits with TATRCMaster’s degree in nursing administration fromDirector COL Dan Kral (Right)the University of Kansas, a Master’s level Certi-7
TATRC TIMESSeptember 2016 Volume 2, Qtr. 4Linked Problem List: Enhancing Access tothe Clinical Record for DoD and VA UsersMany active duty service members transition to theDepartment of Veteran Affairs (VA) for ongoingcare, especially those with disabilities when they separatefrom active duty. Many people, including reservists, continue to receive care in both the DoD and VA systems.Clinicians from the DoD and VA need a total pictureof the care rendered in both facilities for these cases.In response to the mandates of the National DefenseAuthorization Act (NDAA) of 2014, the Joint LegacyViewer ( JLV) was selected as a secured, standard-based,integrated read-only view of electronic health recorddata from the DoD’s Composite Health Care System(CHCS) and Armed Forces Health Longitudinal Technology Application (AHLTA), and the VA’s VeteransHealth Information Systems & Technology Architecture(VistA) Electronic Health Record (EHR) systems, thuseliminating the need for VA or DoD clinicians to accessseparate viewers to obtain patient information from theother facility.The Problem List is one of many widgets in the JLVapplication. It provides a listing of all the active diagnoses, or problems associated with a given patient. Whenhovering with a mouse over a problem in the list, a usercan view the Systematized Nomenclature of Medicine(SNOMED) and International Classification of Diseasesand Related Health Problems - 10th edition (ICD-10)codes associated with each problem. If a JLV user clickson the problem, a more detailed description of thatproblem is shown including a listing of notes, encounters,orders, procedures, or consults related to that problem.However, links to those artifacts are not readily availablefrom within the Problem List widget. In other words,JLV displays all the problems in its Problem List widget,but its users cannot simply click on a problem and easilysee all associated notes, encounters, orders, procedures, orconsults.In AHLTA, linking the associated artifacts with theproblems in the Problem List is a standard feature. In apresentation to the Health Information Exchange WorkGroup earlier this year, COL John Scott, Director forInformatics Policy, Office of the Assistant Secretary ofDefense for Health Affairs OASD(HA), clarified thefeature this way, “[The] AHLTA Problem List Modulecreates a powerful navigation aid for record review. Associated encounters, medications, orders, and artifacts aredisplayed. One click navigation makes it easy to navigateto associated notes and artifacts.” To view the associated artifacts in JLV, a user must switch to each respective domain widget and must remember the identifyinginformation about that artifact in order to retrieve theoriginal note, encounter, order, procedure, or consult.This requires several mouse clicks and when a clinician isbusy, this often does not get done. As Dr. Reese Omizoof the Defense Health Agency (DHA) Innovation andAdvanced Technology DevelopmentDivision (IATDD) and the VA Officeof Informatics & Analytics explains,“users need to be able to make associations between some of the AHLTAassociations that are automaticallybrought in to the Linked ProblemList and keep those associations forfuture use and for shared use.” Healso believes that, “the Linked Problem List feature in the JLV couldchange the way users interact with theEHR in a way that allows cliniciansto be clinicians again.” This prototypeis a positive step toward focusing onclinical workflow while addressingCOL John Scott (standing) gives a presentation on the AHLTAProblems list to the Health Information Exchange Work Group inthe needs of other users that requirewhich TATRC participates.8
Septem
the unclassified military internet where the AHLTA-T servers reside. At the Roles I-III MTFs, a light version of AHLTA-T called Health Assessment Light Operations (HALO), also developed by PM MC4, was used to input new encounters for immediate upload to the remote RDS AHLTA-T serv-ers at Fort Detrick and APG. Once all the components were