Transcription
Craniomaxillofacial Surgery3Universal Screw Removal System (USR)Craniomaxillofacial rigid fixation systems are available from a variety of manufacturers. TheOrthoAnchorSystemThe USR system is a complete screwdriver array thatallowsthe easy removal of virtuallyany craniomaxillofacial screw.The passion to find a better way.At KLS Martin , we are driven to make thebest possible devices so that patients andpractitioners have a reason to smile.The OrthoAnchor System does just that. Absolute anchorage with immediateloading Better, faster results without headgearVisit www.orthoanchor.com to learn more.
2Skeletal Anchorage in OrthodonticsAnchorage control has always been a difficult and unpredictable challenge fororthodontists. Unlike tooth-borne appliances, which rely on patient compliance to achievetooth movement, (bone-borne) implants provide true stationary anchorage, allowingtreatment to proceed more rapidly with highly predictable results. Immediate loading Easy fixation with Drill-Free or self-tapping screws Reduced risk of tooth damage (root resorption, toothloosening, tooth tilting) Maximum retention force Precise control of desired tooth movement Microplates are easy to adapt Normal dental hygiene can be maintained Minimum irritation to the oral tissues Minimized side affectsPre-operative X-rayPlacement X-rayPlacementLoading
3OrthoAnchor ScrewsThe OrthoAnchor screws can be used in cases where maximum anchorage forceis required. The screws are simple to place and designed for immediate loading.The OrthAnchor screws work best in patients over the age of 13 years and whereretention can be attained in good cortical bone.IndicationsContraindications When the present posterior occlusal relationshipshould be maintained stable When cortical bone is not thick enough When there is no dental anchorage When posterior teeth cannot be used as a dentalanchorage due to excessive alveolar bone loss The use of skeletal anchorage will shorten treatment time When maximum anchorage preparation is required When skeletal anchorage is required but the width ofattached gingiva is not adequateDeveloped in cooperation withDr. Paul ThomasSenior Research FellowEastman Dental Institute, London, England Patients with deciduous or mixed dentition Patients with active infection Patient conditions including: blood supply limitations,insufficient quantity or quality of bone, or latent infections Patients with mental or neurological conditions whoare unwilling or incapable of following post-operative careinstructions
455-969-70Teflon container, OrthoAnchor System: Small and compact For OrthoAnchor only55-961-28Office Fixation Kit Module: Level One Style Slots for screw cartridge An all-in-one kit for OrthoAnchor and other in-office procedures1.5mm “soft tissue 1.5x10mm50-345-112.0x6mm50-345-132.0x8mm2.0mm “soft tissue 42.0x8mm50-340-121.5x8mm1.5mm2.0mm6mmThreadLength meterOrthodontic appliances can be attached using the 0.9mm (0.035”) gap on the head of the screw, or through the0.9mm(0.035”) diameter hole in the head of the screw.1.5mm
5C-tube PlatesIn comparison to a single-point anchorage with cylindrical implants, the micro-plate fixationwith our OrthoAnchor system offers additional benefits: Lack of space between tooth roots (plates can be placed away from tooth roots and ‘reach’ down with the orthodontic attachment) Monocortical depth fixation (4-5mm screws can be used) Where OrthoAnchor screws do not provide adequate fixation or force vector, plates provide multiple points of anchorage(micro screws) in the bone that results in an independent stable structure.The use of implant-quality titanium micro plates and screws provides perfectbio-compatibility and ideal adaptation properties.The tube has an inner diameter of 0.9mm (.035”),accepting an archwire, ligature wire, or otherorthodontic hardware.IndicationsContraindications When the present posterior occlusal relationship shouldbe maintained stably When cortical bone is less than 5mm in depth When there is no dental anchorage When posterior teeth cannot be used as a dentalanchorage due to excessive alveolar bone loss The use of skeletal anchorage will shorten treamentperiod When maximum anchorage preparation is required When skeletal anchorage is required but the width ofattached gingiva is not adequateDeveloped in cooperation withProf. Dr. Kyu Rhim ChungKyung-Hee University Hospital Patients with deciduous or mixed dentition Patients with active infection Patient conditions including: blood supply limitations,insufficient quantity less than 5mm in depth, or latentinfections Patients with mental or neurological conditions whoare unwilling or incapable of following post-operativecare instructions General contra-indication is the severely diseased system:Immunodeficiency - irradiated patients - severe diabetes severe osteoporosis
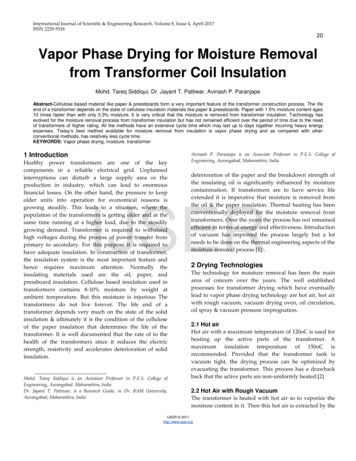
6Advantages of the C-tube PlatesThe principle of C-tube fixation in the lateral maxilla: The eyelet remains in thevestibulum and serves to hold the dental arch wire.Case 115-year old boy is presenting Class II Division 1 malocclusion with permanent dentition. Severe teeth crowding in both upper and lower jaw and protrusion of the upper lip is chief complaint. Maxillary first bicuspids extracted.Pre-treatment intraoral view and lateral cephalogramDental situation of the maxilla.The side view shows clear protrusionof the maxilla.Patient’s lateral cephalogram.
7Intra-operative approachSmall lateral incision with buccal mucosalflap and periosteal elevation in order toplace the C-tube plate.The C-tube plate has been adapted andis fixed with two Drill-Free screws 1.5 x7mm between the 2nd premolar and the1st molar.After suturing, the eyelet remainsin the vestibulum.Occlusal view of the maxilla.The C-tube plate fixed between the rootswith two microscrews.The dental arch is completely formed.Frontal viewInitial stage of treatmentThe eyelet serves as the anchorage pointsfor dental arch wire.12 months post operationFinal results after 1 year.Post-treatment intraoral view and lateral cephalogram
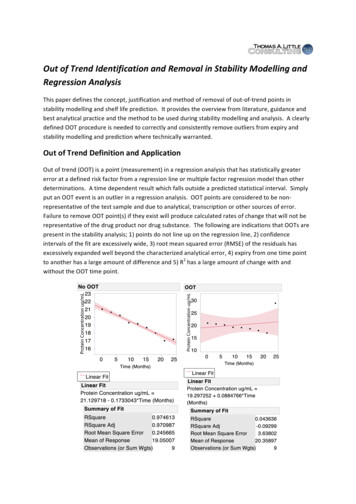
8C-palate PlateThe C-palate plate is recommended in more severe cases, where the orthognathic situation hasto be corrected and palatal traction is needed. The implant is designed to compensate for morecomplex and multidirectional traction forces.Indications When the present posterior occlusal relationship should bemaintained stably When there is not dental anchorage When posterior teeth cannot be used as a dental anchoragedue to excessive alveolar bone loss The use of skeletal anchorage will shorten treatment period When maximum anchorage preparation is required When skeletal anchorage is required but the width ofattached gingiva is not adequateContraindications When cortical bone is less than 5mm in depth Patients with deciduous or mixed dentition Patient conditions including: blood supply limitations,bone quantity less than 5mm in depth, or latent infections Patients with mental or neurological conditions who areunwilling or incapable of following post-operative care instructions General contra-indication is the severely diseased system:Immunodeficiency - irradiated patients - severe diabetes severe osteoporosis
9Advantages of the C-palate Plate The surgery is quick and simple Immediate loading after surgery is possible Application of various force vectors sumultaneously Good resistance against shear forcesThe basic principle of C-palate plate fixation:The plate is fixed to the palatum with threeDrill-Free screws.The dotted lines indicate the submucosalposition of the C-palate plate. Springs areattached to the exposed (red) part of theplate.Post-operative situationPost-anterior retraction situation
10C-tube Plates1/11/125-301-02Micro plate straight2 hole, 6mm bridge/11/1125-301-01Micro plate straight4 hole, 6mm bridge125-301-04Cross-shaped,9mm bridge25-301-03Cross-shaped,6mm bridge/125-301-06Cross-shaped,12mm bridgeC-tube Plates/11/1101-301-31Left hook, 4 hole6mm bridge01-301-32Right hook, 4 hole6mm bridgeC-palate PlatesBracket Plates/1125-301-051/11/1100-301-125mm flat,12mm00-301-145mm flat,14mm/100-301-175mm flat,17mmOrthoAnchor ScrewsCross-DriveScrewCartridges1.5 x 6mm50-340-0899-340-081.5 x 8mm50-340-1099-340-101.5 x 10mm50-340-1199-340-112.0 x 6mm50-345-1199-345-112.0 x 8mm50-345-1399-345-132.0 x 10mm50-345-1599-345-151.5mm “soft tissue collar“/122/1Drill-Free Screws12.0mm “soft tissue collar“/12/11.5 x 4mm-single25-668-04-125-678-04-11.5 x 5mm-single25-668-05-125-678-05-11.5 x 7mm-single25-668-07-125-678-07-11.5 x 8mm01-350-081.5 x 8mm50-340-1299-340-121.5 x 4mm-5 pk25-668-0425-678-042.0 x 8mm50-345-1499-345-141.5 x 5mm-5 pk25-668-0525-678-051.5 x 7mm-5 pk25-668-0725-678-0712Drill-Free Drill-Free Centre-Drive Cross-Drive/2/2
11OptionalOrthoAnchor Teflon Container55-969-70Office Fixation Kit55-961-28Trephine, 5mm diameter38-032-05Bending Pliers25-412-12Lindorf Plate Holding Instrument25-435-15Rosebud Burr51-535-66Right Angle Screwdriver50-900-00Soft Tissue Punch, 2mm28-240-021/2/111/21/2BladesDrillsCentre-Drive 7mm5mm1/11/1Cylindrical attachment1.1mm DIA x 50mm25-451-05Stop 5mm1.1mm DIA x 50mm25-451-07Stop 7mm1.5mm, 80mm25-430-982.0/2.3mm, 80mm25-434-98Cross-DriveStryker attachmentNo Stop7mmStop1.1mm DIA x 50mm25-452-05Stop 5mm1.1mm DIA x 50mm25-452-07Stop 7mm/125-483-972.0/2.3mm, 94mm25-484-97Right Angle BladeDental Latch11.5mm, 80mm/111.1mm DIA x 50mm50-920-07Stop 7mm1.1mm DIA x 50mm50-920-00No Stop1/1/211/21.5mm Cross-Drive50-915-152.0/2.3mm Cross-Drive50-915-201.5mm Centre-Drive 50-910-15/21
TA tradition of innovation and serviceKLS Martin has been manufacturing high quality surgical instruments and medical devices since1896 in Mühlheim, Germany. Our commitment to the creation of innovative products has broughtabout many advancements in the discipline of plastic reconstructive surgery.Surgical innovation and service to our customers are the core principles that drive ourmanufacturing process. Our North American headquarters and extensive network of localrepresentatives brings this relationship directly to you.Please contact us for further information on any of the products you see in this literature.P.O. Box 16369 Jacksonville, FL 32245 Tel. 904.641.7746 800.625.1557 Fax 904.641.7378www.klsmartin.coma member ofThe OrthoAnchor Systemv7 10.02.09
02.10.2009 · Skeletal Anchorage in Orthodontics Anchorage control has always been a difficult and unpredictable challenge for orthodontists. Unlike tooth-borne appliances, which rely on patient compliance to achieve tooth movement, (bone-borne) implants provide true stationary anchorage, allowing treatment to proceed more rapidly with highly predictable results. Immediate loading