Transcription
World J Gastroenterol 2017 January 14; 23(2): 328-335ISSN 1007-9327 (print) ISSN 2219-2840 (online)Submit a Manuscript: http://www.wjgnet.com/esps/Help Desk: http://www.wjgnet.com/esps/helpdesk.aspxDOI: 10.3748/wjg.v23.i2.328 2017 Baishideng Publishing Group Inc. All rights reserved.ORIGINAL ARTICLERandomized Clinical TrialRemoval of diminutive colorectal polyps: A prospectiverandomized clinical trial between cold snare polypectomyand hot forceps biopsyYoriaki Komeda, Hiroshi Kashida, Toshiharu Sakurai, George Tribonias, Kazuki Okamoto, Masashi Kono,Mitsunari Yamada, Teppei Adachi, Hiromasa Mine, Tomoyuki Nagai, Yutaka Asakuma, Satoru Hagiwara,Shigenaga Matsui, Tomohiro Watanabe, Masayuki Kitano, Takaaki Chikugo, Yasutaka Chiba, Masatoshi KudoData sharing statement: The technical appendix, statisticalcode, and data set are available from the corresponding author.Yoriaki Komeda, Hiroshi Kashida, Toshiharu Sakurai, GeorgeTribonias, Kazuki Okamoto, Masashi Kono, MitsunariYamada, Teppei Adachi, Hiromasa Mine, TomoyukiNagai, Yutaka Asakuma, Satoru Hagiwara, ShigenagaMatsui, Tomohiro Watanabe, Masayuki Kitano, TakaakiChikugo, Yasutaka Chiba, Masatoshi Kudo, Department ofGastroenterology and Hepatology, Kindai University Faculty ofMedicine, Osaka-Sayama, Osaka 589-8511, JapanOpen-Access: This article is an open-access article which wasselected by an in-house editor and fully peer-reviewed by externalreviewers. It is distributed in accordance with the CreativeCommons Attribution Non Commercial (CC BY-NC 4.0) license,which permits others to distribute, remix, adapt, build upon thiswork non-commercially, and license their derivative works ondifferent terms, provided the original work is properly cited andthe use is non-commercial. See: aki Chikugo, Department of Pathology, Kindai UniversityFaculty of Medicine, Osaka-Sayama, Osaka 589-8511, JapanYasutaka Chiba, Clinical Research Center, Kindai UniversityHospital, Osaka-Sayama, Osaka 589-8511, JapanManuscript source: Unsolicited manuscriptCorrespondence to: Yoriaki Komeda, MD, Department ofGastroenterology and Hepatology, Kindai University Faculty ofMedicine, 377-2 Ohno-Higashi, Osaka-Sayama, Osaka 589-8511,Japan. y-komme@mvb.biglobe.ne.jpTelephone: 81-72-3660221-3525Fax: 81-72-3672880Author contributions: Komeda Y and Kitano M were involvedin the study conception and design; Komeda Y drafted the articleand analyzed and interpreted the data; Kashida H and Kudo Mperformed critical revision of the article for important intellectualcontent; Tribonias G, Okamoto K, Kono M, Yamada M, AdachiT, Hagiwara S, Matsui S, and Watanabe T collected data; KashidaH, Komeda Y, Sakurai T, Mine H, Nagai T, and Asakuma Yperformed endoscopic procedure; Chiba Y performed statisticalanalysis; Chikugo T conducted pathologic evaluation; all authorsperformed the final approval of the article.Institutional review board statement: The study was reviewedand approved by the Ethics Committee of the Kindai UniversityFaculty of Medicine.Received: August 8, 2016Peer-review started: August 9, 2016First decision: September 20, 2016Revised: October 19, 2016Accepted: November 13, 2016Article in press: November 13, 2016Published online: January 14, 2017Clinical trial registration statement: This study is registered athttp://www.umin.ac.jp/ctr/index.htm. The registration identificationnumber is UMIN000015016.AbstractAIMTo compare the efficacy and safety of cold snare polype ctomy (CSP) and hot forceps biopsy (HFB) for diminutivecolorectal polyps.Informed consent statement: All study participants providedinformed written consent prior to study enrollment.Conflict-of-interest statement: None to declare.WJG www.wjgnet.com328January 14, 2017 Volume 23 Issue 2
Komeda Y et al . Diminutive colorectal polyp removalMETHODSThis prospective, randomized single-center clinical trialincluded consecutive patients 20 years of age withdiminutive colorectal polyps 3-5 mm from December2014 to October 2015. The primary outcome measureswere en-bloc resection (endoscopic evaluation) andcomplete resection rates (pathological evaluation).The secondary outcome measures were the immediatebleeding or immediate perforation rate after poly pectomy, delayed bleeding or delayed perforationrate after polypectomy, use of clipping for bleedingor perforation, and polyp retrieval rate. Prophylacticclipping after polyp removal wasn’t routinely performed.INTRODUCTIONThe United States National Polyp Study demonstratedthat a clean colon (i.e., a colon in which all adeno matous polyps have been eliminated) significantly[1]decreases the mortality rate for colorectal cancer .Accordingly, there is a need to consider the resectionof neoplastic polyps, including diminutive polyps, whenperforming colonoscopy. Cold snare polypectomy (CSP)is becoming a common method for resecting small ordiminutive polyps without using submucosal injectionsor electrocautery, and it is regarded as a safe treatment[2]in Western countries . Recently, it has also gradually[3-5]gained popularity in Japan. The advantages ofCSP are that electrocautery-related damages to thesubmucosal vascular tissue are prevented and there arefewer restrictions on patients’ postoperative activity ordiet. Low rates of postoperative bleeding and perforationcan also be expected, because electrocautery is notused during CSP.Hot forceps biopsy (HFB) is another method usedto remove diminutive polyps; it has been widely usedin Japan, because it is comparatively easy to use.Although the HFB approach is advantageous in thatpossible adenomatous remnants are fulgurated and theblood vessels are coagulated, it also has disadvantagesassociated with electrocautery, such as perforation and[6,7]delayed bleeding . To our knowledge, CSP and HFBhave not been directly compared. We hypothesized thatCSP would be more effective than HFB for resectingdiminutive polyps 3-5 mm. Therefore, the present studyaimed to compare the efficacy and safety of CSP andHFB for removing colorectal polyps measuring 3-5 mm.RESULTSTwo hundred eight patients were randomized into theCSP (102), HFB (106) and 283 polyps were evaluated(CSP: 148, HFB: 135). The en-bloc resection rate wassignificantly higher with CSP than with HFB [99.3%(147/148) vs 80.0% (108/135), P 0.0001]. Thecomplete resection rate was significantly higher with CSPthan with HFB [80.4% (119/148) vs 47.4% (64/135),P 0.0001]. The immediate bleeding rate was similarbetween the groups [8.6% (13/148) vs 8.1% (11/135),P 1.000], and endoscopic hemostasis with hemoclipswas successful in all cases. No cases of perforation ordelayed bleeding occurred. The rate of severe tissueinjury to the pathological specimen was higher HFBthan CSP [52.6% (71/135) vs 1.3% (2/148), P 0.0001]. Polyp retrieval failure was encountered CSP(7), HFB (2).CONCLUSIONCSP is more effective than HFB for resecting diminutivepolyps. Further long-term follow-up study is required.MATERIALS AND METHODSKey words: Cold snare polypectomy; Colonoscopy;Polypectomy; Colorectal diminutive polyps; Hot forcepsbiopsyStudy design, subjects, and methodsThis prospective, randomized, single-center comparisonstudy was conducted from December 2014 to October2015. The inclusion criteria were consecutive patientsover 20 years old and those who were scheduled toundergo the removal of colorectal polyps measuring3-5 mm. The preoperative exclusion criteria werepatients with inflammatory bowel disease, polyposis,polyps suggestive of cancer, and hyperplastic polypsmeasuring less than 5 mm in the distal colon. Similar tohyperplastic polyps less than 5 mm, typical hyperplasticpolyps featuring white, flat protrusions with a diameterof 5 mm or less, which are frequently observed in thedistal colon (rectum and sigmoid colon), reportedlyexhibit no relationship with adenoma onset in thefuture, and guidelines state that no proactive action isrequired. The intra-operative exclusion criteria werepatients converted to endoscopic mucosal resection(EMR), those with polyp retrieval failure, and patientswith non-neoplastic polyps. Patients presenting withdiminutive polyps were assigned to either the CSPor HFB group using computer-generated randomsequencing. The polyp size was estimated on the basis The Author(s) 2017. Published by Baishideng PublishingGroup Inc. All rights reserved.Core tip: Cold snare polypectomy (CSP) is moreeffective in terms of both endoscopic en-bloc resectionrate and pathological complete resection rate thanhot forceps biopsy (HFB) for resecting diminutivepolyps. Moreover, CSP and HFB did not result in anyserious adverse events such as delayed bleeding andperforation.Komeda Y, Kashida H, Sakurai T, Tribonias G, Okamoto K,Kono M, Yamada M, Adachi T, Mine H, Nagai T, AsakumaY, Hagiwara S, Matsui S, Watanabe T, Kitano M, Chikugo T,Chiba Y, Kudo M. Removal of diminutive colorectal polyps:A prospective randomized clinical trial between cold snarepolypectomy and hot forceps biopsy. World J Gastroenterol2017; 23(2): 328-335 Available from: URL: m DOI: http://dx.doi.org/10.3748/wjg.v23.i2.328WJG www.wjgnet.com329January 14, 2017 Volume 23 Issue 2
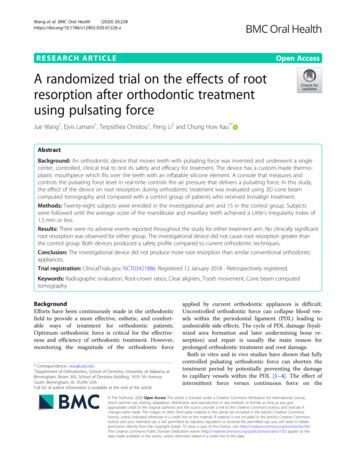
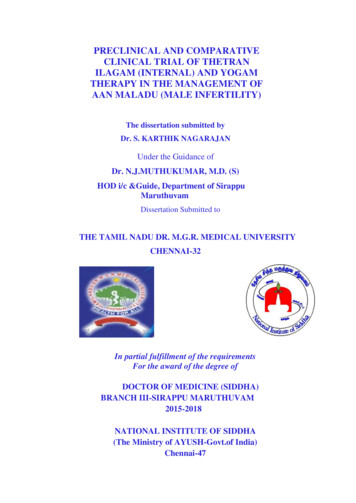
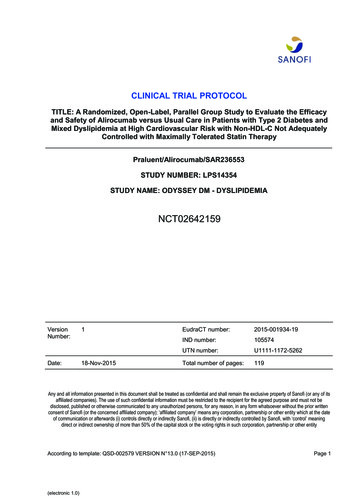
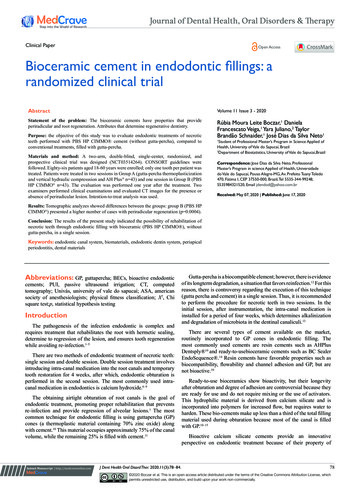
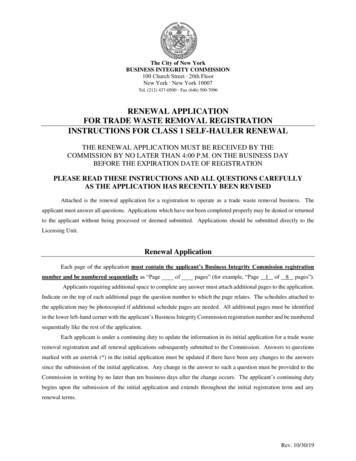
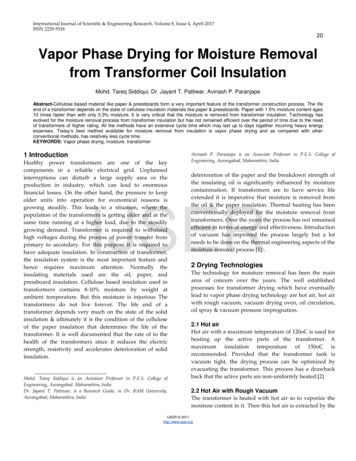
Komeda Y et al . Diminutive colorectal polyp removalhematochezia after the patient was removed from theendoscopic room; this was confirmed by a question naire at the time of the patient’s next hospital visit(7-10 d after treatment). Prophylactic clipping afterpolyp removal was not routinely performed, exceptin patients with immediate bleeding or in those witha high risk for perforation, patients with a bleedingtendency, those taking antithrombotic agents, etc.229 patients were recruitedExcluded: 3 patients (rejected)226 patients were enrolled in this studyExcluded: 18 patients(no diminutive polyps)Endoscopic proceduresScreened, 208 patients in whom at least one polyps was detectedAll colonoscopic procedures were performed by sixexperienced endoscopists (H.K., T.S., Y.A., Y.K., T.N.,and H.M.) who had each performed more than 1000polypectomies before. No colonoscopist had performedCSP before this trial. High-definition endoscopes(PCF-Q260AZI, CF-H260AZI, CF-HQ290I; OlympusMedical Systems, Tokyo, Japan) were used in thisstudy. Patients drank a polyethylene glycol-electrolytesolution (Ajinomoto Pharmaceutical Co., Tokyo, Japan)for bowel preparation. Two types of snares were usedfor CSP: the Profile snare and Captivator-II Snare(Boston Scientific, Natick, MA, United States), bothof which are approved for cold polypectomy in Japan.Each endoscopist chose which snare they preferred.In addition, the FD-1U-1 forceps (Olympus) was usedto perform HFB. The respective maximum widths ofthe FD-1U-1 forceps, Profile snare, and Captivator-IISnare were 7, 10, and 11 mm.During CSP, the polyps were resected withoutinjection or electrocautery, and some of the surroundingnormal mucosa was removed (Figure 1). The transectedpolyps in the CSP group were vacuumed into a trap andwere collected (Figure 2). During HFB, an electrocauterywith coagulating current at 25-30 W in the setting ofthe electrosurgical unit VIO300D (Erbe Elektromedizin,Tuebingen, Germany) was applied to the polyp until the[8]white coagulum was seen at the polyp base (Figure 3) ,and then the polyp was removed by gently pulling itfrom the mucosa. The resected polyps in the HFB groupwere collected in the cup of the forceps.All tissue specimens were examined by an ex perienced pathologist (T.T.) who was blinded to theclinical information concerning the patient and polyp,and to how the polyp was resected. The vertical andlateral cut margins and tissue damage were evaluatedwith a hematoxylin and eosin stain.RandomizationCSP group102 patients183 polypsHFP group106 patients156 polypsExcluded, 35 polypsConverted to EMR (2)Polyp retrival failure (7)Non-neoplastic (26)Included, 148 polypsExcluded, 21 polypsConverted to EMR (1)Polyp retrival failure (2)Non-neoplastic (18)Included, 135 polypsFigure 1 Enrollment flowchart. CSP: Cold snare polypectomy; HFB: Hotforceps biopsy; EMR: Endoscopic mucosal resection.of the maximum width of the opened snare or HFB.Endoscopic and pathological images obtained duringthe tests were de-identified, and they were used tomake diagnoses on the basis of the findings. No limitwas set for the number of polyps removed per patient.Each polypectomy was considered independent of theothers.The study was approved by the institutional ethicscommittee (registration number 26-180; date: Dec 22014), and it was registered with the University HospitalMedical Information Network (UMIN ID: 000015016;date of registration: Sep 1, 2014). Written informedconsent was obtained from all patients.Outcome measuresThe primary outcome measures were as follows:the en-bloc resection rate (endoscopic evaluationwas used to confirm the tumor-free cut margin withmagnified endoscopic view) and complete resectionrate (pathological evaluation was used to confirmthe tumor-free cut margin in microscopic view). Thesecondary outcome measures were as follows: theimmediate bleeding or immediate perforation rate afterpolypectomy, delayed bleeding or delayed perforationrate after polypectomy, use of clipping for bleeding orperforation, and polyp retrieval rate.Immediate bleeding was defined as spurting oroozing blood that continued for more than 1 minfollowing resection that was stopped with hemoclips.Delayed bleeding was clinically defined as evidentWJG www.wjgnet.comSample size calculation and statistical analysisThe sample size was calculated on the basis of theoverall estimated complete resection rate. We assumedthat it would be 95% in the CSP group and 80% inthe HFB group according to the results of previous[9,10]reports (93% and 83%, respectively). Thus, theneeded sample size was 150 polyps per group witha significance level of 5% (two-tailed) and power of80% when the Fisher exact test was used to confirmsuperiority of CSP to HFB. We assumed a dropout rate330January 14, 2017 Volume 23 Issue 2
Komeda Y et al . Diminutive colorectal polyp removalABC500.00 μmFigure 2 Technique for cold snare polypectomy. A: Chromoendoscopy was used to detect the polyp and surrounding normal mucosa, which were captured witha snare, and resection was performed without electrocautery; B: The mucosal defect was assessed to ensure complete resection and no persistent bleeding; C: Thefree cut-margin was negative for neoplastic tissue (area between the arrows).ABCD500.00 μmFigure 3 Technique for hot forceps biopsy. A: A slightly protruded polyp was detected with magnified chromoendoscopy; B: The polyp was captured in the cup ofthe forceps and gently pulled from the mucosa; C: The electrocautery current was applied to the polyp until the color changed to white at the polyp base. Then thepolyp was completely removed from the mucosa; D: Pathologic evaluation of the free cut-margin was difficult to perform because of a thermal tissue injury (arrow).from ITT analysis because endoscopic/pathologicalevaluation of these polyps could not originally be per formed. The target of modified ITT analysis was 157polyps in CSP and 138 polyps in HFB.All statistical analyses were performed using SASsoftware, version 9.4 (SAS Institute, Cary, NC, UnitedStates). Statistical review of the study was performedby a biomedical statistician.of 10%; thus, we determined that the sample sizeshould be 165 polyps per group.Categorical variables were compared with the Fisherexact test, and continuous variables were comparedwith the t-test. To determine predictive factors ofcomplete resection, we conducted multivariable logisticregression analysis with the resection method (CSP orHFB) and polyp characteristics (location, shape, andhistology) as explanatory variables.We performed a modified intention-to-treat (ITT)analysis. In our modified ITT analysis, we consideredpolyps converted to EMR and polyp retrieval failureas incomplete en-bloc resection and pathologicalresection. We excluded the non-neoplastic polypsWJG www.wjgnet.comRESULTSPatients’ and polyps’ characteristicsTwo hundred eight patients were enrolled in the study[mean SD: age 69.0 8.0 years (range 35-87331January 14, 2017 Volume 23 Issue 2
Komeda Y et al . Diminutive colorectal polyp removalwas significantly higher with CSP than with HFB [80.4%(119/148) vs 47.4% (64/135), P 0.0001]; however,there were 6 polyps in the CSP group that broke intopieces during retrieval by aspiration (Table 3). Theimmediate bleeding rate was similar between the twogroups [CSP group: 8.8% (13/148) vs HFB group:8.1% (11/135), P 1.000]. Endoscopic hemostasiswith hemoclips was successful in cases of immediatebleeding. Serious adverse events such as perforationor delayed bleeding did not occur in any case, althoughprophylactic clipping after polyp removal was notroutinely performed, except in cases of immediatebleeding or in those with a high risk of bleeding.The rate of tissue injury according to the pathologicspecimen was higher in the HFB group than in theCSP group [52.6% (71/135) vs 1.3% (2/148), P 0.0001]. The frequency of polyp retrieval failure washigher in the CSP group than in the HFB group (7/148vs 2/135). There was no significant difference betweenthe Profile snare and Captivator II Snare for CSP interms of all the factors (Table 4).The results of this modified ITT analysis were thatthe en-bloc resection rate was significantly higherwith CSP than with HFB [87.9% (138/157) vs 76.0%(105/138), P 0.0001]. The complete resection ratewas significantly higher with CSP than with HFB [70.1%(110/157) vs 44.2% (61/138), P 0.0001]. Therewas no significant difference between the original dataand modified ITT analysis.Multivariable logistic regression analysis showedthat the resection method (CSP vs HFB) was the stron gest predictive factor for complete resection (Table 5).Table 1 Patients’ baseline characteristics n (%)Age (yr), mean (SD)Female sexUse of antithrombotic agentsCSP group(n 102)HFB group(n 106)P value69.4 (8.0)32 (31.3)4 (3.9)68.9 (7.9)31 (29.2)3 (2.8)0.600.760.72CSP: Cold snare polypectomy; HFB: Hot forceps biopsy.Table 2 Polyps’ characteristicsTotal No. of polypsPolyp size (mm)mean SDNo. of polyps perpatient, yHigh-grade adenomaLow-grade adenomaSSA/PHyperplastic polypOtherCSP groupHFB group1484.2 (1.0)1353.8 (1.0)1.51.344/10453/821074111025121246333126420P value0.100.090.161Located from the cecum to the splenic flexure; 2Located from the splenicflexure to the rectum. SSA/P: Sessile serrated adenoma/polyp; CSP: Coldsnare polypectomy; HFB: Hot forceps biopsy.years), 31% women], and we excluded 3 patients whowere rejected (the rejection rate for inclusion in thetrial was 1.3%: 3/229) and 18 patients who had nodiminutive polyps (7.9%: 18/229). After randomizationwas performed, 102 patients were allocated to theCSP group, and 106 were allocated to the HFB group.A flowchart of the study enrollment is shown in Figure1. The mean ages were 69.4 9.4 in the CSP groupand 68.9 7.9 in the HFB group. The mean numberof resected polyps per patient was 1.5 in the CSPgroup and 1.3 in the HFB group. Finally, 283 polyps(CSP group: 148 polyps, HFB group: 135 polyps)were evaluated after excluding some polyps (polypsremoved with EMR, polyps that could not be retrieved,and non-neoplastic polyps). There was no significantdifference between the two groups with regard to thecharacteristics of the patients and polyps (Tables 1 and2). According to the pathological diagnosis, tubularadenoma with low-grade dysplasia accounted for83.4% of polyps in the CSP group and 93.3% in theHFB group.DISCUSSIONWe demonstrated that CSP is more effective than HFBfor resecting diminutive polyps 3-5 mm. Recently,in a randomized controlled trial at a single center,[9]Lee et al reported that CSP was superior to CFP forremoving small polyps 5 mm (93% vs 76%, P [11]0.009). Kim et al also demonstrated that the overallcomplete resection rate wa
Each endoscopist chose which snare they preferred. In addition, the FD 1U 1 forceps (Olympus) was used to perform HFB. The respective maximum widths of the FD 1U 1 forceps, Profile snare, and Captivator II Snare were 7, 10, and 11 mm. During CSP, the polyps were resected without