Transcription
Training InterprofessionalTeams for Patient-CenteredPrimary careWilliam Warning, Crozer-Keystone Family Medicine ResidencyTerry Keene, UCSF, San Francisco VA Medical CenterRebecca Shunk, San Francisco VA Medical CenterMichele Stanek, University of South Carolina School of Medicine
Patient-Centered Primary Care Training Database:Features 130 searchable programs4 Source: www.pcpcc.org/training
Forthcoming Publication: 7 Exemplary ProgramsMulti-professional reviewers analyzed self-reported data and identified innovativeprograms focused on interprofessional education (IPE) training with PCMH learningcompetencies. Sponsoring organizations selected programs & set overall direction forthe publication: AAFP, APA, CSWE, FASHP, NASW, National Center for IPE. To bereleased on December 11, 2014. Harbor-UCLA Family Medicine: Transforming Primary Care & FacultyDevelopment Fellowship New Mexico State University, Counseling Psychology PhD Program Northwestern McGaw Family Medicine Residency: Teaching Health Center San Francisco VA Medical Center: Center of Excellence in Primary CareEducation University of Oklahoma, College of Pharmacy University of South Carolina School of Medicine: I3 Population HealthCollaborative (NC, SC, VA) University of Texas at Austin, School of Social Work5
Training InterprofessionalTeams for Patient-CenteredPrimary careWilliam Warning, Crozer-Keystone Family Medicine ResidencyTerry Keene, UCSF, San Francisco VA Medical CenterRebecca Shunk, San Francisco VA Medical CenterMichele Stanek, University of South Carolina School of Medicine
Center of Excellence inPrimary Care EducationCo-Directed by:Rebecca Shunk, MDTerry Keene, DNP, ARNP
PACT Team-based patient-centered model of care 1200 patients per team Teamlet- Primary Care Provider, Registered Nurse, LicensedVocational Nurse and Clerical Associate Practice Changes Population Management Panel Management Pre-visit planning Huddles Shared Medical Appointments/Group Clinics Walk-in appointments Telephone appointments Secure Messaging Health Coaching
Centers of Excellence (COE) Criteria: Transformative, generalizable, sustainable, andinterprofessional primary care training Must include MD & NP trainees COE awards: Up to 1 M/yr x 5 years, exclusive of any newtrainee positions 5 COEs Cleveland, San Francisco, West Haven, Boise,and Seattle
Mission of EdPACTTo develop and implement an inspirationalmodel of patient-centered, interprofessionaleducation that will advance primary carewithin and beyond the VAJoint effort with: UCSF School of Nursing UCSF School of Medicine Office of Medical Education
Educational Domains of EdPACTKey Components of PACT1. Interprofessional Collaboration2. Patient-Centered Communication & SharedDecision-Making3. Sustained Relationships4. Performance Improvement
Health Professions Primary care training ina team-based, PCMHmodel Practice partnershipmodel Each trainee hashis/her own panel andcross-covers partners’patients Interprofessionaltrainees supportmultiple traineeteamlets
Educational Domains of EdPACT1. Interprofessional Collaboration: care is teambased, efficient and coordinated; trainees practicecollaboratively2. Patient-Centered Communication & SharedDecision-Making3. Sustained Relationships4. Performance Improvement
Curricular FrameworkWorkplaceReinforcement( Experiential)3 ½ days clinic/ wkDidactic6 conferences/wkCulture ofTeam-basedCareReflection
Curricular Content:Interprofessional CollaborationDidacticsInteractive small group seminars:HuddlingTeam Members RolesHandoff communicationFeedbackConflict ResolutionDebriefingWorkplace reinforcement:HuddlingHuddle CoachesPreceptors reinforce skills andprovide feedback during huddlesTeams engage in formativeassessment processesReflectionHalf-day retreat:Team buildingOpportunities to reflectIdentifying similarities anddifferences
Huddle
Collaborative Conferences PACT ICU Diabetes Board Collaborative Case Conference Mental Health and Primary Care Conference
Outcomes: Trainee Reflections The huddle is such an awesome opportunity to really connect withdifferent team members and figure out what’s important to them andmake a game plan for handling the tougher patients and distributingwork in a way that gets stuff done and everyone feels like they havehelp. (R2, 2012-13) Watching how we built the team and seeing how it actually improvedpatient care - that was inspiring for our future in primary care It wasreally cool to see. (R2, 2011-12) On a personal level, to get to know people a little bit and feel like youhave a relationship. It makes you feel better about coming to clinic andbeing part of a community that’s taking care of people. (NP student, 201213)
Faculty and Staff Participants Longitudinal MD & NP preceptors UCSF NP Faculty- 2 SFVA NP Faculty- 9 MD Faculty -15 plus Chief Residents in Ambulatory Care and QI Clinical psychology faculty & fellows Experts in communication, teamwork, performanceimprovement Additional health professionals– podiatry, social work,pharmacy, nutrition
Curricular ContentSustained Relationships: FacultyDidacticsBasic TrainingNational TeamSTEPPS ProgramPACT trainingTEACH and Motivational InterviewingUCSF SOM OME and SONFaculty Development CoursesSmall Group FacilitationWorkplace reinforcement:Interprofessional PreceptorsReinforce skills/ give feedbackduring preceptingFeedback on teaching sessionsAcademy of Medical EducatorsTIPTOPReflective Practice:American Academy forCommunication in HealthcareTeam RetreatsMonthly Curricular Meetings
Thank You
Questions?
Team Development Results:Years 1 & 2STAGESCORECOMPONENTSPre-team0-36None to Role Clarity58-63Goals-means Role Clarity881-86Goals-means ClarityFully pt)Spring(Mar/Apr)In PlaceYr 1 - Trainee4 Teams: 59.4Yr 2 - Trainee Teams: 62.2Yr 1 - Trainee Teams: 64.6Yr2 - Trainee Teams: -measure/Pages/Default.aspx Last Accessed 1/12/2012.Firmly In Place
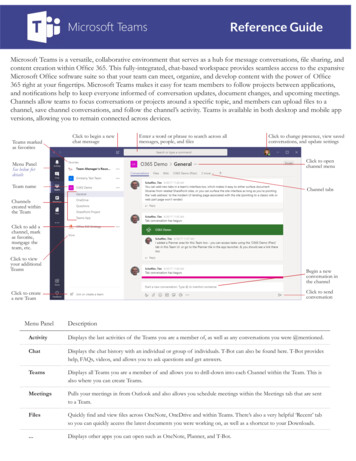
Team Development Scores by TeamFall 2012 to Spring 2013100889082TDM Scores (0 - 100)8081766360607369706664 6459565578746055564850403020100Team 1Team 2Team 3Team 4Team 5Team 6Team 7R2-NP student Teams (Fall and Spring)Aug/Sept 2012Mar/Apr 2013Team 8Team 9Team 10
Highlights from the National PACT EvaluationKari Nelson, MD MSHSAssociate Director, PACT Coordinating CenterInvestigator, Northwest Center of Excellence, HSR&D Modest overall effect of PACT on health care utilization & costs Decrease ACSC hospitalizations & specialty mental health visits; increasedprimary care visits Potential costs avoided from April 2010- FY2012 600M; modest negativeshort term ROI Provider and staff burnout rates are high Volume of clinical reminders reported as greatest barrier to deliveringoptimal patient-centered care Teamlet huddles reported as greatest facilitator to PACT implementation Implementation can be measured using administrative, provider andpatient level data at the national level Higher levels of implementation associated with higher patient satisfaction,lower provider burnout, and decrease in ACSC hospitalizations
26Results: Hospitalizations for Ambulatory Care SensitiveConditions (ACSC), Veterans age 65Predicted ACSChospitalizations ifPACT 0Predictedhospitalizationsfor ACSCsObservedhospitalizationsfor ACSCsHospitalizationsavoided-4.2%
Changes in process of care pre- and post-PACTPatient Access and Utilization QuarterlyTrendsLarge increases in phone care visitsPACTstartsRosland, Nelson in press AJMC
Changes in process of care pre- and post-PACTSteady increase in access and continuityLarge increase in post-hospital follow upSmaller increase in secure message enrollment and utilizationPACTRosland, Nelson in press AJMC
Training InterprofessionalTeams for Patient-CenteredPrimary careWilliam Warning, Crozer-Keystone Family Medicine ResidencyTerry Keene, UCSF, San Francisco VA Medical CenterRebecca Shunk, San Francisco VA Medical CenterMichele Stanek, University of South Carolina School of Medicine
I3 PopulationHealth CollaborativeImproving the health of populations in SC, NC and VAI3 Population Health CollaborativeTraining Interdisciplinary TeamsMichele Stanek, MHSI3 Population Health CollaborativeUniversity of South Carolina Department of Family &Preventive Medicine
I3 Population Health CollaborativeI331Population Health Collaborative 29 Family Medicine, InternalMedicine and Pediatricresidencies across SC, NC, VAand FL Almost all PCMH Level 3designated teaching practices Over 325,000 patients,providing over 850,000 visits Majority served are minoritypatients 680 Residents 339 Faculty 140 staff
I3 Population Health Collaborative3IImprovements in teaching practicesbenefit: Patients of the practice directly Graduating residents’ patients Community practices’ patients
I3 Population Health CollaborativeAcademic3 ‘Population HealthvCollaborativeIHII Regional focus Ongoing learning community Practice improvement & relatedcurriculum innovations Additional meetings & more time Team participation Academic arm (scholarship & curriculum)
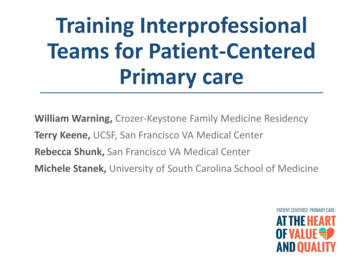
I3 Population Health CollaborativeI3 Chronic Illness CollaborativeChronic Illness (Diabetes, CHF)May 2006 – September 2008AshevilleHendersonvilleAndersonChapel Hill umbia (USC)CHFDiabetesCharleston (MUSC)DiabetesProcess measures HbA1c testing Foot exam Self-management documentedOutcome measures HbA1c 7 BP 130/80; 140/90All met/exceeded NCQA goalsCHFProcess measures LVEF ACEI/ARB β-blocker “Best practice” careOutcome measure Hospitalization38% reduction in hospitalizationNewton W, Baxley E, Reid A, et al. Improving chronic illness care in teaching practices: learnings fromthe I3 collaborative. Fam Med. 2011;43(7):495-502.
I3 Population Health CollaborativeI3 PCMHCollaborativePCMH – NCQA RecognitionMay 2009 –Nov folk/Portsmouth(EVMS)GreensboroChapel Hill (UNC)Winston SalemGreenville (ECU)Asheville (WFU)ConcordHendersonville FlorenceWilmingtonColumbia (USC)Internal MedicinePediatricsFamily MedicineExecutive CommitteeCharleston (MUSC)GoalsSpread Topic: chronic illness practice Geography: more residencies (25) Discipline: Peds, GIMPCMH NCQA recognition Practice improvement EducationKey OutcomesNCQA Recognition 22/25 programs committed toNCQA application All 22 achieved recognitionReid A, Baxley E, Stanek M, Newton WP. Practice transformation in teaching settings: Lessons from theI3 PCMH Collaborative. Family Medicine. 2011;43(7):487-94.
I3 Population Health CollaborativeI3 Population Health CollaborativePopulation HealthMay 2012 –Dec 2015GoalsSpread Topic: practice population Geography: additional residencies Discipline: Peds, GIMIHI ‘Triple Aim’ Improve patient experience Reduce cost of care Improve quality of careAll at the same timeKey Outcomes Core Measures Across the Triple Aim Threads/Workgroups focusing onspecific improvements in each aim
I3 Population Health CollaborativeMethodsLearning Sessions 2x per year Face-to-face contact Share clinicalinnovations & bestpractices Share new curriculumand training approaches Develop capacity fortransformation Dedicated team time Plan next action periodAction Periods Monthly thread datacollection & PDSAs Monthly threadwebinars Expert didactics Data reporting Experience sharing I3 SharePoint site Academic Arm:Curriculum & scholarlyproducts Annual Core Measures
I3 Population Health CollaborativePractice is the curriculum
I3 Population Health CollaborativeApproach Preparing future healthcare professionals as wellas supporting current healthcare professionals ingaining new knowledge and skills Broad approach to “learners” – All Learn/AllTeach Tactical approaches to practice change includingteam based care Experiential learning experiences Focus on system/curricular changes but also needcultural changes Learning organization – meet needs of practiceteams
I3 Population Health singWisely ssCare
I3 Population Health CollaborativeInterdisciplinary Team Training Form/Structure– Interdisciplinary team participation Incentives for team involvement Active mentorship of practices– Shared leadership at collaborative & practicelevel– Teams required to develop and implementcurricular changes– Redirection in course every 6-months; newstrategic direction every 2-3 years– Learning opportunities open to all members ofteam
I3 Population Health CollaborativeInterdisciplinary Team Training Function/Dynamics– 3 monthly webinars led by interdisciplinary practiceteam members– Learning Sessions Role-based Affinity GroupsTeam-based Care concurrent session trackLearner SessionsLearning from Each Other Sessions– Practice Improvement– Educational/Curriculum– Participating practice innovations & best practices– IHI Open School chapters
I3 Population Health CollaborativePromise & Challenges of Team-BasedCare Development Support development of new/expanded roles– Acquisition of new skills & experiences– Acceptance of new roles– Adaption of new capabilities/job performance metrics Education & training is not always enough -- Contentto Culture Teamwork & team-based care in acute environments Multiple masters Tension between continuity with personal provider &care team Resources needed for team-based care Impact of team-based care on patient experience
Chapel Hill (UNC) Greenville (ECU) Anderson Concord Columbia (USC) Spartanburg CHF Diabetes Chronic Illness (Diabetes, CHF) May 2006 - September 2008 Newton W, Baxley E, Reid A, et al. Improving chronic illness care in teaching practices: learnings from the I3 collaborative. Fam Med. 2011;43(7):495-502.