Transcription
Patient-Centered Referral Workflow AutomationSession 260, February 14, 2019Heather Trafton, PA-C, MBA, SVP of National MSO Operations, Steward Health Care NetworkKristin Ottariano, MSHI, Director of Medicaid Operations, Steward Health Care Network1
Conflict of InterestHeather Trafton, PA-C, MBAKristin Ottariano, MSHIHave no real or apparent conflicts of interest to report.2
Agenda HIMSS Learning Objectives Steward Health Care Network The Challenge Steward’s Approach1Process Improvement2System Development3Enhance & Scale Lessons and Recommendations Questions3
Learning Objectives1. Adapt a patient-focused, user-driven approach to referral portaldesign2. Construct a set of business rules to govern an automatedreferral workflow3. Design a referral process that improves patient, PCP, specialist,and administrator experiences4. Select the data required to support referral workflow automationbased on business requirements5. Plan to roll out a new referral workflow to a large providernetwork4
Steward Health Care Network5
STEWARD HEALTH CARE NETWORKA Clinically Integrated, Community Based ACOWith the Vision:To be the top performing ACO and health planFor:Commercial, Medicare, Medicaid PopulationsMissionAchieve the quadruple aim: Better care of individuals Better health for populations Lower cost Drive value to physicians outside ofthe traditional fee for service constructHow we create value Quality ManagementCare and Utilization ManagementAccurate Risk AdjustmentCare CoordinationNetwork Governance andPerformance Management6
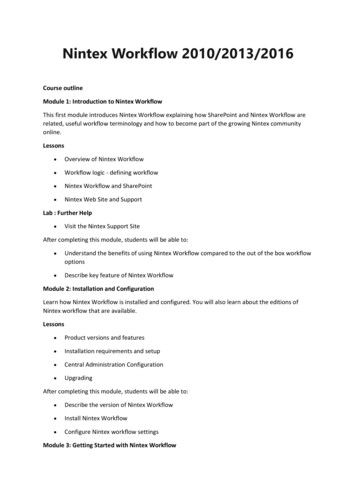
Steward Health Care Network FootprintMA, 13 LocalChaptersOne of the largest ACOs in the country, SHCN has 6regions. Each region has local chapters.Holy FamilyHospitalOH/PA, 4 Local ChaptersUT, 4 Local ChaptersDavis Hospitaland MedicalCenterJordan ValleyMedical Center West JordanHillsideHospitalSalt LakeRegional MedicalCenterTrumbull RegionalMedical CenterEastonHospitalNashobaValleyMedicalCenterSt. Elizabeth’sMedical HospitalMortonHospitalJordan ValleyMedical CenterSharon RegionalMedical CenterSt. Anne’sHospitalGoodSamaritanMedicalCenterMountain PointMedical CenterTX/AR/LA, 6 Local ChaptersAZ, 3 Local ChaptersSt. Luke’sMedical CenterSt. Luke’sBehavioral HealthCenterWadleyRegionalMedical CenterWadley RegionalMedical Center at HopeOdessa RegionalMedical CenterMountain VistaMedical CenterTempe St. Luke’sHospitalThe Medical Centerof Southeast Texas– Victory CampusSouthwestGeneralHospitalGlenwood RegionalMedical CenterThe Medical Centerof Southeast TexasSt. JosephMedical CenterFL, 3 Local ChaptersRockledgeRegional MedicalCenterMelbourneRegional MedicalCenterSebastian RiverMedical Center7
Steward Health Care System LLCSteward HospitalManagement CompanySteward Medical Group(SMG)Steward Health CareNetwork (SHCN) 33 US hospitals across 9states, focusing on drivingvalue to patients through highquality / low cost access pointsof care 1,800 providers inemployed multi-specialtygroup across 11 states Equal partnership betweenhospitals, employed andaffiliated physicians 3000 total employees 7,300 beds undermanagement 385 practice locations Highly-integrated deliverysystem, health plan andmanaged care contractingentityPhysician-Affiliated Businesses 6 ASCs, 25 affiliated orowned urgent care providers;and 42 preferred SNFs 34,000 employees Approximately 500 PCPs eICU, Mobile Oncology (PET)Imaging, Tailored RiskAssurance Company(“TRACO”)Steward International Hospitals in Malta Letter of Intent withCroatian Ministry ofHealth 1,300,000 covered livesunder value-based contracts 5,500 contracted physicians Nationally-recognizedpopulation health & analyticsinfrastructureSteward is a nationally recognized, fully integrated, healthcare system centered aroundcommunity care as a means to meet the increasing market demand for value.8
The ChallengeHow do we quickly and efficiently refer patients to highquality providers in their community?9
Frustration for Patients, ProvidersSpreadsheetsFaxPortalsEmails1/3 of patients in theUnited States receive areferral each year (2 onaverage for elderlypatients)1– but many do notresult in appointmentsFragmented and time consumingworkflow for practice staffFrustrating experience and poorcare coordination for patientsHow could SHCN improve the experience for 2 million patients?(1) MC3160594/10
Steward’s ChallengePoor visibility into local specialistsInefficient staffing of referral coordinators across the systemFragmented processes across the Steward systemLack of comprehensive and real-time data to understandreferral patterns and service line gapsInability to track referral status11
Vision: Patient-Centered Care CoordinationStewardHealth CareNetworkPROVIDERPATIENT Provide high-quality,coordinated care Efficient process thatdoesn’t burden practicestaff Access to a high-qualityspecialist close to home Appointment available in areasonable amount of time Covered by insuranceSHCN Improve patient experience Reduce administrativeburden on our practices Staffing efficiency Monitor data and addressareas of opportunity12
Steward’s Approach13
3-Phase ImplementationPHASE 1PHASE 2PHASE 3ProcessImprovementSystemDevelopmentEnhancements andNational Use CaseExtension14
Phase 1 : Process ImprovementSHCN’s initial approach focused on:Improving provider and practice manager awareness of high-qualityspecialists through an improved DoctorFinder website, local meet andgreets, marketing, and a trained and knowledgeable referral team.Establishing centralized referral coordinators to reduce theadministrative burden on practices by identifying appropriate specialistsand processing referrals.“Simplification” Reducing paperwork for referrals to high-qualityproviders through managed care agreements.Medical Director Oversight: Establishing a process for SHCN to reviewreferrals for select specialties.Performance Monitoring: Developing reports to monitor referralpatterns, staff productivity, and service line gaps.15
Results and Room for ImprovementSHCN improved the referral process, but there were persisting challenges.ResultsPersisting Challenges 60% of PCPs utilizing centralizedreferral processing (131%increase from previous year)Increase in referrals to highquality Steward providersImprovement in patientexperience Inefficient paper processProviders lacked insight intocase statusIncomplete and lagged dataInconsistent usage acrosspractices (only 20% of referralssubmitted through process)16
Phase 2: System DevelopmentPlatformrequirements Accessible to affiliated and employed providers Automated eligibility check to replace timeconsuming manual process Rules engine to allow SHCN to configure businessrules by payor, specialty, and geography Nudge to suggest high quality providers located nearthe patient Allows for centralized processing Includes process for case review and status tracking Comprehensive tracking and reporting available inreal-time Scalable to new markets Improves the patient experience17
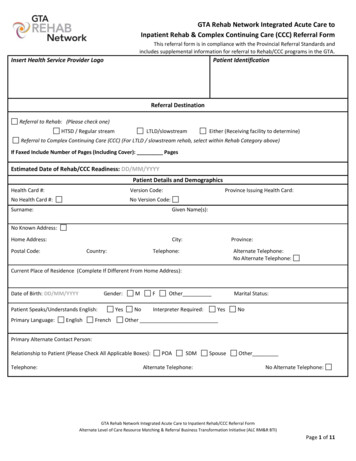
Underlying ArchitectureSHCN’s Referral Platform is powered by a central data warehouse. Key datacomponents are: patient demographics and managed care attribution, providerdemographics, and specialist insurance credentials.PatientReferral PlatformProviderPop Health VendorsPayorCare ManagementClaimsEMRQuality/RiskADTLabs/RxProvider DirectorySHCN CENTRALDATA WAREHOUSEDashboard Reports MembershipQualityPatient ExperienceAd Hoc Analytics18
Key Data SourcesThree data sources are critical to legitimacy, ease of use, and dataintegrity/reporting:PATIENTPAYOR1. Patient data: Patient demographic data is used to identify specialistscovered by the patient’s insurance and located within an appropriategeography. Provides the option to tie back to patient utilization data orlimit submissions to patients within the data warehouse.2. Provider data: Pre-populates information to support ease of use ofend user. Accuracy is critical to identifying appropriate specialists PROVIDERespecially data on specialty and sub-specialty. Provider data alsopowers the user attribution model, linking users to providers andpractices.3. Payor data: Payor rosters identify providers in the referral circle foreach insurance plan. Accuracy is critical to classifying cases assimplification, needs processing, or requires review.19
Referral EntryPractice staff log in to a secure URLto submit referrals. Users enter member and PCPinformation on a submission page. A type-ahead function autopopulates fields from Steward’sdata warehouse. An automated eligibility check isexecuted.20
Specialist Selection Selection: Users select a specialist by enteringspecialist information or searching based on specialty. Results: Providers return based on distance from thepatient. Workflow: A rules engine classifies the referral into oneof three categories, triggering associated workflows.“Simplification” Workflow“Needs Processing” WorkflowRules Engine“Requires Review” Workflow21
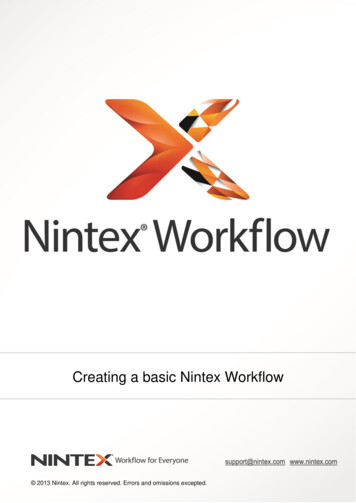
Nudge ScreenIf the referral requires Medical Director review, the tool will surface specialists that meetsimplification criteria and do not require review, sorted by distance from the patient. The referral you submitted requires review.User getsnotificationthat referralrequires reviewList ral is sentto MedicalDirector tReferral isprocessed withsimplificationworkflow22
Case Queue Submitted cases enter aqueue where users canview all related detailsand activity. Referral coordinators canmanage cases from endto end within the queuepage. Cases can be edited,redirected, escalated,and shared.23
Referral SummaryThe user can view, print, or fax a summary of the referral with keyinformation (referral number, case ID, patient information).24
NotificationsUsers receive emailnotifications whenthere is activity ontheir cases (new caseassignments, casedecisions, questions/comments).25
Administrative – Rules EngineSHCN controls key administrative functions, including a rules engineand user access. A rules engine ensures referrals are handledconsistently as the network grows.Flexibility: Rules can be configured by Geography Specialty Payor Network affiliationDeceptive simplicity: A significant amount of work went intodistilling the business requirements into a workflow that wasas simple, clean, and scalable as possible.26
Administrative – User AccessThe user management design attributes end-users to PCPs and practicesbased on structured data stored in the data warehouse. This approach allowsusers to view cases based on their relationship to the PCP and practice andallows staff to cross-cover cases.27
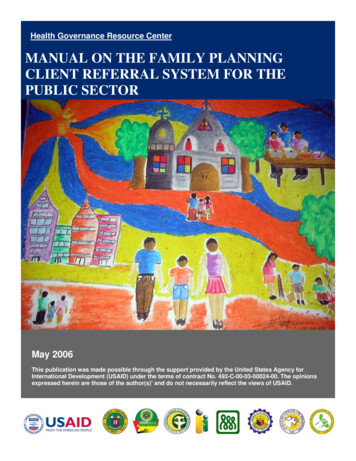
Implementation Process 6 month implementation period after initialproduct developmentMonth1 2 3 4 5 6Referral Coordinator Roll-OutMedical Director Roll-OutProduct enhancements Phased approach to implementation allowing forproduct enhancements as each user type wasadded to tool Swift roll-out to PCP sites (6 weeks)–General education through Provider & PracticeManager meetingsFull Roll-Out–Face-to-face meetings with high volume practicesProvider Education–Education to end users of previous referralsubmission processTest Sites Roll-OutProduct enhancements28
Reporting & Results 90% of practices using the referral management toolto submit referrals for review and processing (up from60%) Average time to process referrals is 1 day if it doesnot require Medical Director review and 5 days if itdoes require Medical Director review Practice staff report ease-of-use and improved abilityto track referral results Improved visibility into Medical Director reviewdecisions, service line gaps, referral patterns, andreferral staff performance29
Phase 3: Scale & EnhanceNational Roll-Out SHCN is expanding nationally and building our network innew markets Standard, centralized processes, and administrativesupport allow providers to focus on patient care Critical factors:– Cloud-based platform– Provider data accuracy– Local strategy– Increasing visibility intohigh-quality providers30
Scale & EnhanceOngoing enhancements to benefit referring practicesSurfacing utilizationhistory and claimsdata to close loop onreferralDirect SchedulingEMR integration31
Scale & EnhanceNew use cases: Behavioral Health, High-Tech RadiologyUse Case #1Use Case #2Bringing BehavioralHealth carecoordination in-houseCentralizing High-TechRadiology care coordinationduring expansion32
Lessons Learned & RecommendationsProcess First,Then TechnologyProviderAdoption FocusVendorResponsiveness& CustomizationPatient-CenteredProcess DesignCoordinatedStrategy33
Questions Please complete online session evaluation Contact us:Heather Trafton, m/in/heather-trafton-43961914Kristin Ottariano, tinottariano34
1. Patient data: Patient demographic data is used to identify specialists covered by the patient's insurance and located within an appropriate geography. Provides the option to tie back to patient utilization data or limit submissions to patients within the data warehouse. 2. Provider data: Pre-populates information to support ease of use of .