Transcription
Health Governance Resource CenterMANUAL ON THE FAMILY PLANNINGCLIENT REFERRAL SYSTEM FOR THEPUBLIC SECTORMay 2006This publication was made possible through the support provided by the United States Agency forInternational Development (USAID) under the terms of contract No. 492-C-00-03-00024-00. The opinionsexpressed herein are those of the author(s)' and do not necessarily reflect the views of USAID.
TABLE OF CONTENTSPageAcknowledgements1List of Abbreviations2INTRODUCTION3I. Purpose of the FP Client Referral System4II. Scope of the FP Client Referral System5III. Elements of a Functional FP Client Referral System6IV. Organizing the Public Sector FP Client Referral System7V. Referral ProceduresA. Referrals for FP Contraceptives & PillsB. Referrals for BTL and NSVC. Referrals for Consultation and Technical EvaluationVI. Recording and Reporting9131722A. ReferrrorB. Receiving ProviderVII.Monitoring and EvaluationAnnexesA.B.C.D.E.F.G.H.I.J.2425Levels of Public Health Care and Service Capability for Family PlanningCriteria for Selection of Private ProvidersSynopsis of Department of Health Administrative Order 158Memorandum of UnderstandingAddendum Contract of servicesReferral slip for dispensing commoditiesInformed consent form for surgical sterilizationReferral form for consultation/technical interventionReporting tables for referrorReporting tables for receiving providers
ACKNOWLEDGEMENTSThe development and production of this manual was made possible through the supportand invaluable inputs of the following resource persons for which deep gratitude isextended by the authors: The Provincial Population Office of Pangasinan under the stewardship of Ms. LuzMuego and her staff, Ms. Loida Episcope, Ms. Vicky Banez for their help inimproving the systems content of this manual so that they may be as relevant andas useful for the users of this manual in the province of Pangasinan. The same isalso acknowledged for the selection of the municipalities/cities for the pilotimplementation of this referral system The Municipalities/Cities of Mangaldan, Binalonan and Urdaneta under thestewardship of Dr. Ophelia Rivera, Dr. Larry Patawaran and Dr. BernardMacaraeg implementation of this referral system even if it meant adding to thealready voluminous tasks and activities in their respective offices. Dr. Babes Perez, Ms. Lynn Almario, Ms. Risa Yapchiongco, Mr. Fidel Bautista,Mr. Delbert Marquez of the PRISM Project and their consultants Dr. MelchorLucas, Jr. and Ariel Canaveral, likewise under the funding assistance of USAIDfor the collaboration in the design and development of this referral system andmanual especially in the clinical procedures presented herein. Ms. RoseAnn Gaffud (Field Coordinator, LEAD for Health Pangasinan) and Mr.Ed Joel Carlos , Ms. Ailene Nitor and Mr. Daniel Culili (PLCPD - LEAD forHealth Pangasinan Partner) for providing the logistical arrangements in theconduct of coordination meetings with the pilot areas. Mr. Verne Quiazon and Ms. Ida Cayetano for the relentless faith and support tothe authors of this manual that it may come to fruition and final completion forthe benefit of use in the various LGUs who may adopt the referral system forfamily planning services from the public to the private sector towards achievingthe market development goals ultimately leading to the attainment ofContraceptive Self-Reliance in the country.Once again, our heartfelt gratitude and acknowledgement for all the assistance.1
LIST OF ESSTDUSAIDDevelopmentUSDAdministrative OrderBarangay Health StationBarangay Health WorkerBilateral Tubal LigationCommunity-Based Drug OutletCommunity-Based Monitoring and InformationContraceptive Independence InitiativeContraceptive Self-RelianceDepartment of HealthFamily PlanningHealth CenterIntra-Uterine DeviceLocal Government UnitLocal Health System (Sector)Municipal Health OfficeMarried Women of Reproductive AgeNon-Government OrganizationNon-Scalpel VasectomyPhilippine Health Insurance CorporationPhilippine PesoProvincial Health OfficePopulation CommissionRural Health UnitSocio Economic StatusSexually Transmitted DiseaseUnited States Agency for InternationalUS Dollar2
INTRODUCTIONFor the last 30 years, the country’s Family Planning Program has relied primarily onforeign donations for the supply of contraceptives. Specifically, the United StatesAgency for International Development (USAID) has been providing 80% of thecountry’s contraceptive supply – pills, condoms, IUDs and injectables, amounting toaround USD 3 million yearly.In 1999, the national government of the Philippines produced a draft of the ContraceptiveIndependence Initiative (CII) to launch the country’s bid to be more self-reliant insecuring its own contraceptive supply. This was spearheaded by the Department ofHealth followed through by a multi-sectoral task force convened by the POPCOM thatled to the issuance by the DOH of a National Family Planning Program Policy inSeptember 2001. Overall, this policy states that the Philippine Government will nowassume greater responsibility for the Family Planning (FP) program of the Philippines.In response to this development, USAID initiated the program for the phase-down of itscontraceptive assistance to the Philippine government. The continuing support of USAIDshall now be focused on the country’s poorest and the neediest coming from the socioeconomic brackets D1 (earning roughly PhP 5,209 to PhP 7,291 per month) and E (PhP5,208 and below per month). After several meetings with key stakeholders in thisindustry, USAID officially announced its phase-down plan to the public in September2002. Phasedown of pills began in 2004, and will be completely phased out by 2007.Injectables shall begin in 2005 and will be completely phased-out by 2008. IUD’s isplanned for a later date because of the lack of availability of other brands and sources inthe country.Since then, preparations have been underway to ensure that family planning services willcontinue to be given to both current and future potential users. Many initiatives havebeen undertaken in the national government level towards the direction of contraceptiveself reliance. However, in the local government level, the LGU’s capacity to completelycover the current as well as future demands may be constrained by its limited funds.While this might be the case, several studies already show that many contraceptive usersare actually willing to pay for their supplies, that is, of 4.6 million women who usecontraceptives, 1/3 or 3.22 million come from middle and high income classes who canafford and are willing to pay for their supplies. As such, one of the approaches beingexplored is the setting up of a client referral network whose aim is to direct public sectorclients to the appropriate provider in the private sector and also higher level public sectorproviders. Once the referral networks is in place, the public and private FP providers shallhave covered both the non-paying and paying clients respectively and contribute to theelimination of “unmet needs” for family planning.3
PURPOSE OF THE FP CLIENT REFERRAL SYSTEMThe health care delivery system typically involves different geographic units,departments, and levels—including central, regional, and community. Thinking about theway work is organized helps managers and providers throughout the system to see theirorganization as a collection of interdependent resources (including infrastructure,supplies, and referral sites) and processes (such as client scheduling and informationmanagement) that change and evolve in response to both clients’ and staff needs.In the public health sector, there are different levels of health care providers. The mostbasic unit is the barangay health station followed by the rural health unit, municipalhealth hospital, district hospital and provincial health hospital. Each of these has adifferent service capability for family planning services (Attachment A). For casesbeyond its capability level, the health care provider sends its patient to another provideras a referral. The health provider from whom the patient/client is being transferred iscalled the referring provider or referror while the health provider to whom thepatient/client is being transferred is called the receiving provider.This manual is written to guide the health care providers in setting up a Family PlanningReferral System that will standardize the referral procedures among participating FPservice providers and/or commodity dispensers to help ensure a safe and efficient transferof services in the network As necessary, the municipality may also improve the systemsor procedures contained herein so that it may respond to other conditions existing in thelocality.4
SCOPE OF THE FP REFERRAL SYSTEMThe local health landscape consists of the private sector and the public health sector. Todate, the bulk of family planning services are still availed of from the public sector. Withthe phase-down of donated contraceptives, the private sector will now have a more activeinvolvement in the effort to address the challenges of the national family planningprogram. One of the ways this can be done is through organizing a referral network.Broadly speaking, the referral network can be established along the following types:1. Referrals from Public Sector Facilities/Providers to other PublicFacilities/Providers2. Referrals from Public Sector Facilities/Providers to PrivateFacilities/Providers3. Referrals from Private Sector Facilities/Providers to PublicFacilities/Providers4. Referrals from Private Sector Facilities/Providers to other rThis manual will focus on the second referral type (i.e. from Public to Private) althoughmuch of the procedures may be applicable to any of the other three sectors.In addition, within each sector, there are different geographic levels of health servicedelivery such as:1.2.3.4.BarangayMunicipalityInter-local Health ZoneProvincialThese guidelines herein address the inter-provider referral of family planning clients atthe municipality level to cover FP referrals made for any of the following reasons:1. Directing paying patients to the private sector and non-paying to the publicsector for FP services and commodities.2. Accessing services not available in a particular FP facility (i.e. BTL,Vasectomy, diagnostics)3. Consulting for an expert opinion (e.g. consultation with a specialist for clientswith medical conditions)4. Accessing a technical intervention (e.g. referring complications arising fromcontraceptive use)These guidelines do not include inter-facility transfers of acutely ill patients due tomedical conditions. This is already covered by existing policies & guidelines in the healthsystem.5
ELEMENTS OF A FUNCTIONAL REFERRAL SYSTEMGood referral systems help family planning and other clinics offer clients the right care atthe right place. Linking services with delivery sites offers clients access to appropriatecare at every level of the health care system—from community facilities for basic care todistrict, regional, or higher-level facilities for specialized care. Referral systems can giveclients access to a complete range of services without inconvenience and unnecessaryrepetition of diagnosis or treatment. They also enable health centers to offer serviceswhich are not cost-efficient to offer elsewhere because the demand for the service is onlya handful.A referral system is essentially a relationship between two or more health providers. Thisrelationship is formalized through an agreement indicating the elements and themechanics behind such a relationship. These providers help each other complete thetreatment of their patients through a referral. They provide feedback of the results of thereferral and regularly update each other on the effectiveness of the system.Thus, the important elements needed to ensure a functional referral system are:1. Providers’ consent to participate in the referral system2. An agreement to formalize the referral relationships3. Set of guidelines to detail the elements of the referral system (what, when, andhow to refer, and a fee schedule)4. An administrative mechanism to oversee/coordinate the system5. Monitoring/evaluation/feedback systemIn this referral model, the suggested elements to operationalize these five elements in thereferral system are:1. Memorandum of Agreement for participating providers2. Referral Manual that contains specific guidelines to govern the referral system3. The MHO as the central organization and the PHO as the provincialconsolidator of information6
ORGANIZING THE PUBLIC HEALTH SECTOR REFERRALSYSTEMIn 1991, with the passage of the Local Government Code, the responsibility for theprovision of basic services, including family planning, was devolved to the localgovernment units. This is specifically provided for in section 17, of Republic Act 7160otherwise known as the Local Government Code of 1991. Thus Family Planning Servicesform part of the basic services that local government units now provide (source D.O.H.Administrative Order 158). In preparation for the phase out period, the Municipal HealthOffice (MHO) will need to engage other health providers and dispensers to share in theprovision and dispensing of FP services and commodities. The most logical way is tokeep the clients who are unable to pay for FP services and commodities in the publicsector and refer clients with the capacity to pay to the private sector. To build up thissystem, the Municipal Health Office may follow the following steps in organizing its FPClient referral system:1. The Municipal Health Office convenes existing FP providers around its catchmentarea. A criteria for selection of private providers is herewith provided.(Attachment B)2. The Municipal Health Office gives an orientation on the following topics forbetter decision-making of the providers in joining the referral network:a. Key points of the D.O.H. A.O. 158 (Attachment C)b. The referral system guidelines contained in this manualc. Benefits of executing a Memorandum of Understanding (Attachment D) inconsonance with the Referral System guidelines.3. The Municipal Health Office then formally recruits the FP providers who haveupdated Licenses To Operate or Business Permits to join the network by signingthe MOA.4. All participating providers submit their complete contact information and servicecapabilities to be entered in a directory. Copies of this directory are laterdistributed to the members of the network.5. As applicable, Municipal Health Office prepares an addendum contract(Attachment E) for providers who opt to cover arrangements not included in theMOU with specific referral partners. Some of these arrangements may typicallyinclude the fee structure, terms of payment, the clinic hours, and other specialinstruction to clients.6. The Municipal Health Office monitors the referral activities and submits reportsto the Provincial Head Office.7
7. Trainings in family planning are organized as appropriate in the network. Thesemay be organized with the help of the Provincial Health Office, ProvincialPopulation Office and other Project Offices who offer technical assistance for freeor for a nominal fee.8
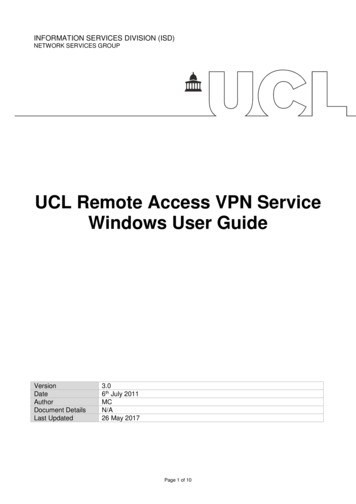
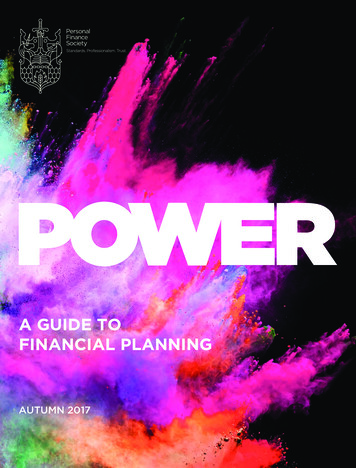
REFERRAL PROCEDURESA. Referral for FP contraceptives and pillsReferror:1. The client enters any FP provider in the public health system. If the providerhas the capability, he/she provides counseling. If the provider does not havecapability to do counseling he/she provides basic information and makesappropriate referral to the next higher level (Attachment A) of public healthsector FP service provider.2. After counseling has been done, the client together with the FP providermakes a decision on the type of FP method (i.e. pills or injection) to avail of.3. Next, the FP Provider determines the client’s ability to pay based on existingsystems or criteria for client classification in the local health center.4. Clients who have the ability to pay are given the following choices:a. Advise the client that because of the phasing out of the freecontraceptive supplies, the introduction of fees and charges forcommodities is now underway. Explain the details of fess and charges.ORb. There are existing private service providers in the catchment area towhom they maybe referred to. Make sure that there is priorinformation as to what is available in the private service providersbefore making a referral to avoid client inconvenience. A referralslip/prescription (Attachment F) is prepared (in duplicate copies). Theoriginal copy is given to the client together with directions to thenearest provider/dispenser of FP contraceptive. The client shall presentthis to the seller of the contraceptive every time a purchase is made.This slip will be valid for a limited period of time (example threemonths only) so that a follow-through examination can be performedby the service provider to monitor on the client’s condition. Thesecond copy is kept for filing as basis for follow-up and reportpreparation later on.5. Those who have no capacity to pay are retained in the government facility andare given free FP contraceptives.Receiving Provider:9
1. The dispenser asks for the referral slip/prescription from the client.2. The client presents the referral slip/prescription for each purchase of pills orinjections. The referral slip/prescription will be valid for 3 to 6 months asexplained earlier by the referror.3. The FP commodity is dispensed.4. The dispenser signs at the appropriate space in the referral slip/prescriptionindicating the items and number of times the commodities were dispensed.Same time, it shall list down the client’s name and purchase details in theReport on Referrals form.5. Every month, the Report on Referrals will be furnished to the MHO so thatthis may be shared with the respective Referrors.6. At the end of the validity of the referral slip, the dispenser shall advise theclient to get another referral slip.10
11
12
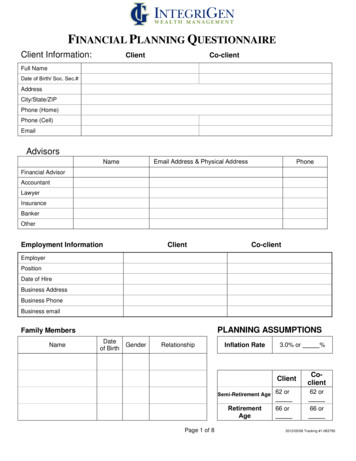
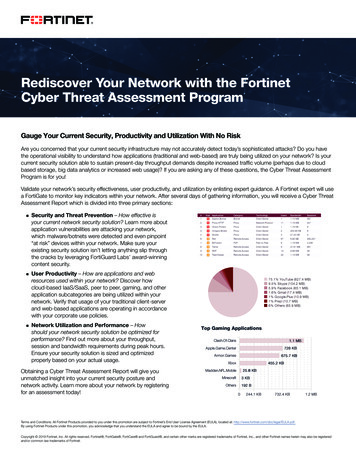
B. Referral procedure for BTL/NSVReferror1. Conducts counseling to the client2. If the client decides on surgical sterilization, the FP service provider explains the elements of the Informed Consent form(Attachment G) which the client is to sign afterwards to confirm acceptance/agreement to avail of the procedure.3. Evaluates client’s ability to pay. Non-paying clients are referred to the nearest government facilities while paying clientsare referred to private facilities pre-certified for this particular service.4. Fills up the referral form (in duplicate copy), gives pre-operative instructions to the client. For those referred to a privateprovider, informs them of the fee schedule and other relevant instructions contained in the Addendum Contract signed bythe receiving provider.5. Coordinates with the receiving provider for the schedule of the procedure.6. Gives one copy of the referral form to the client and files the duplicate copy which will serves as basis for follow-up andreport preparation later on.7. Makes arrangements for transportation if requested by the client. If not, directions on the receiving provider’s location aregiven.8. Calls the client or the receiving provider to determine the status of the referral and resolves problems that may arise.Receiving Provider:1. Upon the referral call of the referror, the designated person in the receiving facility reserves an operating room schedule forthe client.13
2. Informs the surgeon of the operating time slot.3. When the surgeon and operating schedule are confirmed available, accepts the referral.4. Upon the arrival of the client on the day of surgery, examines the records, evaluates the client.5. The client is asked to sign an Informed Consent Form to ensure his/her confirmation or acceptance of the procedure.6. When all requirements are in order, performs the procedure.7. Files the referral form.8. Every month, the Report on Referrals is furnished to the MHO so that this may be shared with the respective Referrers.14
15
16
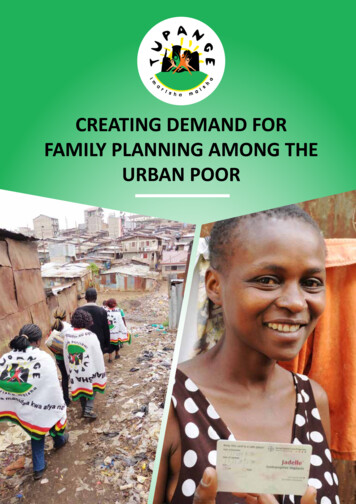
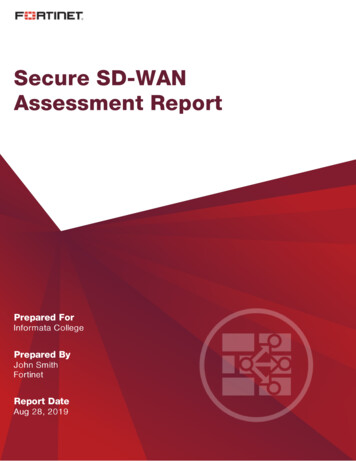
C. Referral procedure for consultation or technical evaluation.Referror:1. Evaluates the client’s condition.2. If needed, she orders laboratory tests to confirm his/her assessment.3. If a condition is beyond her expertise, a referral is made.4. Explains to the client the reason for referral.5. If the referral requires a technical intervention, informs the receiving provider of the referral. Upon consent to accept thereferral, proceeds in referring the client.6. Fills up the referral form (in duplicate) (Attachment H) has the client sign the consent statement of the form and providesthe following information:a.b.c.d.e.Patients nameImpression or diagnosisTime of referralThe name of the referring providerThe requested service7. Gives the referral form and instructs the client on the fee schedule (if there is any) and directions on the receivingprovider’s location.8. Retains the management of the patient under her/his care in transit.9. Keeps the duplicate copy for filing which will serve as basis for follow-up and report preparation later on.17
10. Follows up the client or the receiving provider to determine the status of the referral.Receiving Provider:1. Receives the client and studies the referral note.2. If the condition is within the provider’s capability level, accepts the referral and proceeds in treating the client. If beyond,refers the client to the appropriate provider.3. Files the referral form.4. Every month, the Report on Referrals is furnished to the MHO so that this may be shared with the respective Referrers.18
19
20
21
RECORDING AND REPORTINGReferror:A. Recording Proceduresa. The referror always fills up a referral slip/form in duplicate copies.b. The original copy is given to the client to be presented to the receiving provider.c. The duplicate copy is kept on file.d. Daily, the duplicate copies are segregated as: a) referral for dispensing, b) for surgical sterilization, c) for consultationand technical evaluation.e. Based on the duplicate copies, the following tables are filled up at the end of the day (Attachment I)i. Table for dispensing referralsii. Table for surgical sterilization, consultation and technical evaluationB. Reporting Proceduresa. Every month end, the tables are sent to the Municipal Health Office via fastest means possible.b. The Municipal Health Office summarizes the report for the municipalities covered and submits this to the ProvincialHead Office.Receiving ProviderA. Recording Procedures22
a. Receives the referral slip/form and files.b. Daily segregates the referral forms as: a) referral for dispensing, b) for surgical sterilization, c) for consultation andtechnical evaluation. The following tables are filled up (Attachment J)i. Table for dispensing referralsii. Table for surgical sterilization, consultation and technical evaluationB. Reporting Proceduresa. Every month end, the tables are sent to the Municipal Health Office via fastest means possible.b. The Municipal Health Office summarizes the report for the municipalities covered and submits this to the ProvincialHead Office.Collation of information is done at the provincial level. The data is summarized and the indicators are assessed. A report is generatedand distributed in the referral network.23
MONITORING AND EVALUATIONThe referral system needs to be monitored and evaluated to find out if it addressed the objectives for which it was established.Monitoring is checking something at regular intervals in order to find out how it is progressing or developing while evaluation is theact of considering or examining something in order to judge its value, quality, extent, or condition. Monitoring therefore involves theregular collection of data and arranging these data elements in a manner where periodic comparison of the level of performance can bemade. Once a certain benchmark of performance is reached, evaluation of that specific aspect is performed and remedial action isdesigned and instituted.The following table shows the suggested data elements, their sources, purpose and suggested thresholds and steps to follow ifthresholds are reached.SourceNumber of out goingreferrals by typeNumber of referrals receivedNumber of serviced referralsFor clinical referrals, reasonfor referralNumber of participatingprovidersComplaints from providersComplaints from clientsPurposeBenchmarkActionsTo determine level of participationof providersTo determine level of acceptanceby providersTo determine effectivenessTrend must be maintained or increasingExamine cases that may be inappropriatelytreatedDetermine reason for non-acceptanceTo determine specific areas ofconcernTo determine the status of thesystemTo determine areas forimprovementTo determine areas forimprovementNo unjustified referral upon evaluationNumber of out going referrals must matchreceived referrals by 100%95% of received referrals must be servicedMust not be decreasing in numberDetermine reason for inability to serviceclientDetermine the cause of unjustified referralsMust be 0%Determine reason for withdrawal ofproviders from the systemExamine the systemMust be 0%Examine the system24
ANNEXES25
LEVELS OF PUBLIC HEALTH CARE AND SERVICE CAPABILITY FOR FAMILY PLANNINGHEALTH FACILITY /PERSONFP SERVICEPOORNON-POOR*BHWs and BSPOs Pill re-supplyBHS Pill initial and re-supply IUD insertion (case to case basis) & checkup Injectables Pill initial and re-supply IUD insertion (case to case basis) & check-up InjectablesRHUs Pills IUD insertion Injectables Pills IUD insertion InjectablesMUNICIPALHOSPITAL PillsIUDInjectablesVenue for VSS procedures of itinerant teams PillsIUDInjectablesVenue for VSS procedures of itinerant teamsDISTRICT ANDPROVINCIALHOSPITAL PillsIUDInjectablesSurgical sterilizationsProvides resources for itinerant teamsMgt. Of complications PillsIUDInjectablesSurgical sterilizationsProvides resources for itinerant teamsMgt. Of complications26
CRITERIA FOR SELECTION OF PRIVATE PROVIDERSTypes of Private Providers:Private Doctors–Obstetrician-GynecologistFamily Medicine / Family PhysicianPrivate MidwivesDrugstores/PharmaciesHospitalsGeneral Criteria:The important considerations in choosing a private provider are 1. Accessibility to your paying clientele. Check the geographic clustering of your paying clients to be able pinpoint which areasprivate providers are most suitably needed. Decide on a ratio of paying clients to private providers to be able to decide how manyproviders are essential. An oversupply of private providers may also result in unnecessary competition in turn leading to disinterestin joining the network.2. Willingness/ Capability/ Competence to provide quality Family Planning service/contraceptives. Some private providers are notautomatically willing to provide the modern methods of family planning which this program is promoting. Therefore, this shouldbe clarified early on to ensure non-coercion in joining the network. Subsequently, you need to determine if the skills in providingthis service is still up-to-date. First and foremost is that the private provider should have undergone DOH-prescribed FP training.Moreover, there may be a need to enroll in some refresher courses for family planning service that are available from a number oftraining suppliers. Finally, please check if the private provider has the basic clinical equipment and facility as stipulated by theDepartment of Health to render family planning service.27
3. Track record of outstanding medical practice – it is important that the integrity of the network is protected especially since somesectors of society might associate the family planning program with some illegal medical practice (e.g. abortion. ) resulting inrejection of family planning.4. Active Membership in a Professional Organization – preferably the private provider is a member of a relevant professionalorganization such as Philippine Obstetrics and Gynecology Society (P.O.G.S), Philippine Academy of Family Physicians(P.A.F.P.), Integrated Midwives Associated of the Philippines (IMAP), Philippine League of Government and Private Midwives(PLGPMI), and Drugstore Association of the Philippines (D.S.A.P.). Membership in such organization helps ensure that theprivate provider has the basic qualifications as a medical practitioner. On occasion, the organization provides access to relevanttraining programs for family planning and access to supplies necessary for family planning services.Additional Criteria:For those providing Contraceptives / temporary Methods 1. Maintains affordable and continuous supply of contraceptives including variety of types and brands prescribed by the providerto the client.2. Compliant to the practice of requiring client to show a prescription from a private provider before selling a contraceptiveFor those providing Permanent Methods 1. Available service time for family planning surgical procedures2. Preferably Philhealth-accredited so that clients may have the option to apply for reimbursement for VSS services obtainedfrom the private provider.3. Preferably Hospital-based or hospital-affiliated to ensure access to complete facilities in providing quality family planningservices, as well as, handling of complications that may arise after the procedure is performed.28
MEMORANDUM OF UNDERSTANDINGKNOW ALL MEN BY THESE PRESENTS :The undersigned PARTIES, all Filipinos, of legal ages, residents of the municipalities/city as specified hereunderwithin the Province of Pangasinan, in their capacities or as representatives of the Local Government Units or entities forwhich they have been legally and duly authorized to act as such, hereby agree to enter into a Memorandum ofUnderstanding to establish a CLIENT REFERRAL SYSTEM wherein the PARTIES may, altern
Thus, the important elements needed to ensure a functional referral system are: 1. Providers' consent to participate in the referral system 2. An agreement to formalize the referral relationships 3. Set of guidelines to detail the elements of the referral system (what, when, and how to refer, and a fee schedule) 4.