Transcription
Interpreting Safety Culture Survey Resultsand Action PlanningKatherine J. Jones, PT, PhDUniversity of Nebraska Medical Center1
Objectives Measure to Understand What did you measure?– Define organizational culture, safety culture– Identify 3 types, 3 levels, and 4 universal components Why did you measure safety culture?When should you measure safety culture?How do you measure?How do you interpret results?– Frameworks/Concepts– Role of leadership in engineering culture Develop an action plan to implement specificbehaviors2
DefinitionsCategoriesTypesLevelsComponentsWHAT DID YOU MEASURE?3
What is organizational culture?The shared, learned beliefs and behaviors of stablegroup members Allow us to make sense of our environment Reflect common language (think TeamSTEPPStools) and behavior .thus is heard and observed Leaders create/teach culture as they reward/provide feedback/hold accountable Can be measured with self-report toolsWe can not change what we do not measure!Schein, E.H. Organizational Leadership and Culture 4th ed. San Francisco:John Wiley & Sons; 2010.4
Categories of CultureMacrocultureSubcultureOrganizational Culture(Schein, 2010)Microculture5
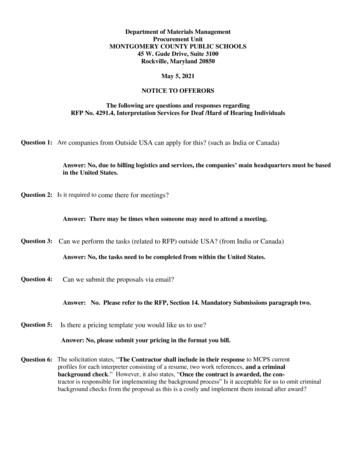
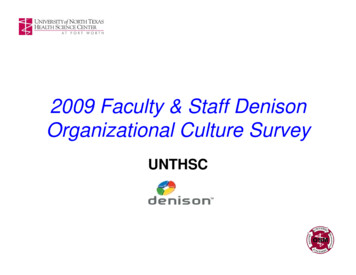
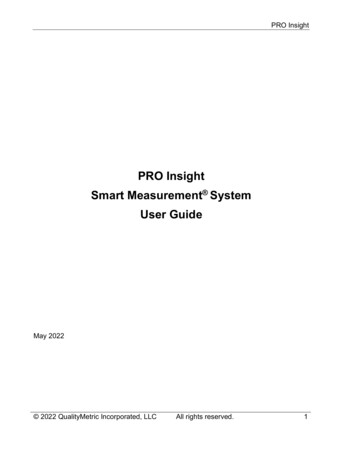
Three Types of Organizational Culture Pathological—use of information to enhancepersonal power– Punitive environment Bureaucratic—use of information to adhere torules, positions, and protect turf– Information collected but use of information forlearning and change is limited Generative—use of information to achieve themission– Practices interact to support 4 componentsWestrum, R. A typology of organizational cultures. Quality and Safety inHealthcare 2004;13:22-27.
Three Types of Organizational CulturePathologicalLow cooperationBureaucraticRule ibilitiesshirkedare narrowSharing infoSharing infodiscouragedtoleratedFailurescapegoat FailureJusticeMessengers shotChangecrushed rsencouragedResponsibilities aresharedSharing um, R. A typology of organizational cultures. Quality and Safety inHealthcare 2004;13:2-27.
Three Levels of Organizational CultureBehaviorsBeliefs &Values“ in manyorganizations, valuesreflect desiredbehavior but are notreflected in observedbehavior.”UnderlyingAssumptionsSchein, E.H. Organizational Leadership and Culture 4th ed. San Francisco:8John Wiley & Sons; 2010, p.24, 27.
What is a Culture of Safety? Enduring, shared, LEARNED1 beliefs andbehaviors that reflect an organization’swillingness to learn from errors2 Four beliefs present in a safe, informed culture3––––Our processes are designed to prevent failureWe are committed to detect and learn from errorWe have a just culture that disciplines based on riskPeople who work in teams make fewer errors1. Schein, E. Organizational Culture and Leadership. 4th ed. San Francisco, CA: John Wiley &Sons; 2010.2. Wiegmann. A synthesis of safety culture and safety climate research; rsPDFs/TechReport/02-03.pdf3. Institute of Medicine. Patient safety: Achieving a new standard of care. Washington, DC:The National Academies Press; 2004.9
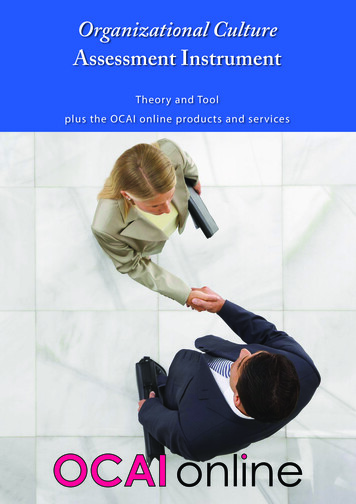
Four Components of Safety CultureA culture ofsafety isinformed. Itnever forgetsto be afraid Reason, J. (1997). Managing the Risksof Organizational Accidents. Hampshire,England: Ashgate Publishing Limited.Battles et al. (2006). Sensemaking ofpatient safety risks and hazards. HSR,41(4 Pt 2), 1555-1575.SENSEMAKINGTRUST10
Institute of Medicine Reports Role of Culture in Chain of Impact Joint Commission and National QualityForum High Reliability Organizations engage incontinuous improvementWHY MEASURE SAFETY CULTURE?11
The Problem and Challenge “The problem is not bad people; theproblem is that the system needs to bemade safer . . .”IOM (2000). To Err is Human: Building a Safer Health System“The biggest challenge to moving toward asafer health system is changing the culturefrom one of blaming individuals for errors toone in which errors are treated not aspersonal failures, but as opportunities toimprove the system and prevent harm.”IOM (2001). Crossing the Quality Chasm: A New Health System forthe 21st Century, p. 7912
Chain of Impact at the Point of CareHealthcare SystemStructures & ProcessesOrganizationalStructures & ProcessesBeliefs -- Culture – BehaviorsIndividual ProviderStructures & ProcessesInterpersonalCareQuality at Point of CareTechnicalCareThe quality, safety and value of care can be no better than the structures and processesused by providers in direct contact with the patient. Culture is a lens through whichorganizations must support providers at the point of care.Adapted from:Nelson et al. (2002) Joint Commission Journal on Quality Improvement, 28, 472-493.Swuste P. (2008). Human Factors and Ergonomics in Manufacturing, 18, 438-453.1313
Joint Commission & NQF Joint Commission 2010 Leadership Standards forhospitals (Standard LD.03.01.01)– Leaders create and maintain a culture of safety– Leaders evaluate the culture on a regular basis– Leaders encourage teamwork; they createstructures, processes, and programs to support it National Quality Forum Safe Practice 2: CultureMeasurement, Feedback, and /OnlineExtras/JCLS09/JCLS09 H.pdfhttp://www.qualityforum.org/News And Resources/Press Kits/Safe Practices forBetter Healthcare.aspx
HROs Engage in Continuous ImprovementMeasureBeliefs andBehaviorsActionPlanImplementPracticesWe can not change what we do not measure!15
Goals of Culture Assessment Identify areas of culture in need of improvement– Identify impairments in organizational learning Increase awareness of patient safety concepts Evaluate effectiveness of patient safetyinterventions over time Conduct internal and external benchmarking, Meet regulatory requirements Identify gaps between beliefs and observedbehaviors within subcultures and microcultures16
Goals of Culture AssessmentReferences Jones, Skinner, Xu, Sun, Mueller. (2008). The AHRQHospital Survey on Patient Safety Culture: a tool to planand evaluate patient safety programs. Advances in PatientSafety: New Directions and Alternative 99/ Nieva VF, Sorra J. Safety culture assessment: A tool forimproving patient safety in healthcare organizations. QualSaf Health Care 2003; 12(Suppl II): ii17-ii23. Schein, E.H. Organizational Leadership and Culture 4th ed.San Francisco: John Wiley & Sons; 2010, p.327.17
Baseline prior to patient safety intervention18 – 24 month intervalsWHEN SHOULD YOU MEASURESAFETY CULTURE?18
Qualitative Focus Groups Structured Interviews ObservationQuantitative Survey Tools use best tool for your settingHOW DO YOU MEASURE SAFETYCULTURE?19
Measure Beliefs and Behaviors with HSOPS Survey tool kit ture/hospsurvindex.htm Comparative Database for 567,703 respondents from 1,128 hospitals in 2012 database 42 items categorized in 12 dimensions– 2 dimensions outcome measures at dept/unit level– 7 dimensions measure culture at dept/unit level– 3 dimensions measure culture at hospital level 2 additional outcome measures at dept/unit level Comments2020
UNMC Adapted HSOPS Available at www.unmc.edu/rural/patient-safety Developed by UNMC as part of AHRQ Partnerships inImplementing Patient Safety Grant 05 -07 Collapses work areas and positions to reflect CriticalAccess Hospital (CAH, 25 beds) environment Allows sorting by Work Area/Position if 5 respondents Creates valid HSOPS benchmarks for CAHs Supports use of HSOPS to evaluate patient safetyinterventions over time in CAHs Evaluates impact of TeamSTEPPS by adding 10 items toassess training, knowledge, and adoption of behaviors21
Original AHRQ HSOPS 2012 Comparative Database30%UNMC Adapted HSOPS2.3%22
Original AHRQ HSOPS 2011 Comparative DatabaseUNMC Adapted HSOPS21%0.9%
UNMC Adapted HSOPSExtent of TeamSTEPPS Training24
UNMC Adapted HSOPSImpact of TeamSTEPPS Training on Knowledge of Toolsalpha 0.7125
UNMC Adapted HSOPSImpact of TeamSTEPPS Knowledge on Implementation of Toolsalpha 0.7926
Reason’s Components of Safety CultureYour ResultsReverse Worded ItemsGap between values/beliefs and behaviorKirkpatrick’s Taxonomy of Training CriteriaResponse Shift Bias9 Step PlanHOW DO YOU INTERPRET HSOPSRESULTS?27
HSOPS Dimension orReason’s ComponentsOutcome MeasureReporting Culture - a safeorganization is dependent onthe willingness of front-lineworkers to report their errorsand near-missesJust Culture - managementwill support and rewardreporting; discipline occursbased on risk-taking Frequency of EventsReported (O) Number of EventsReported (O) Nonpunitive Response toError (U)O Outcome measureU Measured at level of unit/departmentH Measured at level of hospital28
HSOPS Dimension orReason’s ComponentsOutcome MeasureFlexible Culture - authoritypatterns relax when safetyinformation is exchangedbecause those with authorityrespect the knowledge offront-line workers Teamwork w/in Units (U) Staffing (U) Communication Openness (U) Teamwork ax Units (H) Hospital Handoffs (H) Hospital Mgt Support (H)Learning Culture organization will analyzereported information andthen implement appropriatechange Manager Actions (U) Feedback & Communication (U) Organizational Learning (U) Overall Perceptions (O) Patient Safety Grade (O)29
Your ResultsResourcePurposeExcel ToolANALYSIS - Contains raw dataGenerates spreadsheet to upload for national databaseInstructions for interpretationDemographics of respondentsContains dimension and item level results in the aggregate, bydepartment, position, direct patient care, action planning sheetBenchmarkGraphsCOMMUNICATIONCompare aggregate results to peer group (external benchmark)Compare aggregate results over timeCompare results by work area and job title to the aggregateItem Level OverTimeCOMPARISONS AND COMMUNICATIONCompare item level results over time and to peer groupIncludes responses to teamwork questionsComments Codedby ThemeCONTEXTOpen ended comments coded by culture-related themesProvides respondents’ direct feedbackAction PlanPLAN – Exec Summary and work sheet to anchor plan in history, missionand strategic goals; identify practices needed to support safety culture
SAMPLE HOSPITAL FROM SUMMER 2012EXEC SUMMARYREVERSE-WORDED ITEMSOPPORTUNITIES & RECOMMENDATIONSDEFINE THE PROBLEMSTRENGTHS, WEAKNESSES, CHANGESVARIATIONS – WORK AREA, JOB TITLE, TEAMGAPS BETWEEN BELIEFS & BEHAVIORSCOMMENTSMATCH PROBLEMS WITH OPPORTUNITIESSKILLS
Reverse-Worded Items If Item labeled with “R” then it is positive toDISAGREE Bigger numbers always better Positive is positive for patient safety12. Nonpunitive Response to ErrorPositive1. Staff feel like their mistakes are held against them.(A8R)2. When an event is reported, it feels like the person isbeing written up, not the problem. (A12R)3. Staff worry that mistakes they make are kept in theirpersonnel file. %Weakness*Green Bar % DISAGREE/STRONGLY DISAGREE for REVERSE-WORDED ITEMS
Define the Problem Benchmark Graphs– Overall strengths & areas in need ofimprovement from Peers & National Database– Changes over time– Variations by work area, job title, Team skills Action Planning Worksheet from Excel Tool– Values reflect the desired behavior within each of thefour components– Are observed behaviors consistent with values?
ComponentExample CommentReporting Culture People need to understand the importance of reporting so we can change thesystem, not think they will be punished if they do report.Just CultureManagement does not care for your suggestions. If you write them up they finda way to get you in trouble for reporting it.A few people in the hospital have abrasive personalities and this makes them hardto approach. .patient care would be smoother and safer if not for their attitudes.Also if an employee is not demonstrating the skills expected of their professionthat person should be remediated and or let go.TeamworkCultureWe help each other well within our department and we are responsive torequests from other departments when they ask help of us.I have not been trained in the two challenge rule, SBAR, or CUS. I feel thatcommunication and cooperation between departments could be improved.Learning CultureWhen a problem is reported in another department, I never get a report orcomment back about what is going to be done to prevent the problem or aresolution to the current problem.Safety ConcernComputerized charting has made Emergency nursing much less efficient and lesssafe.Patient SafetySystemsFeedbackWe have lots of policies and procedures in the hospital . It's okay to know whereto find them but if you don't have time to sit and read them how are we supposedto know what they contain?Evidence PositiveSafety CultureI have worked here for many years and have seen many changes and I do have tosay we have always had the patient's safety and care front and foremost. 34
Match Problems to OpportunitiesIV. Inventory of Safe PracticesDateRate the extent to which practices that support the four components of safety culture are in place. Indicate ifthe inventory is for:Hospital as a wholeWork AreaScoring: 0 Not in place1 ineffective2 moderately effective3 very effectiveNA not applicableReporting PracticesScoreFormal reporting of adverse events with standardized taxonomies (e.g. National Coordinating Council forMedication Error Reporting and Prevention A – I Error Severity Taxonomy)Near misses are frequently reported, valued, and learned from4Non-harmful errors that reach the patient are frequently reported, valued, and learned fromSafety Briefings (also considered a Learning Practice)Leadership WalkRounds (also considered a Learning Practice)Other (Describe):Just Culture PracticesTraining provided on role of human factors in error and active vs. latent sources of errorThe principles of Just Culture are understood and used by managementDiscipline is based on risk-taking and not on outcomesManagers use Algorithms to balance individual and system accountabilityPolicy/procedures in place to manage disruptive behaviorsOther (Describe):Flexible Culture Practices: Teamwork and Communication SkillsBriefs are used to assign roles, establish expectations, and establish contingency plansHuddles are used to assess the need to change a planDebriefs are used to learn by reviewing team performance and conducting after action reviewsMonitoring actions of other team members (e.g. Cross Monitoring to “watch each other’s back”)Front-line providers use a structured approach to monitor patient care situations (e.g. STEP: Status of thepatient, Team members, Environment, Progress toward goals)Task assistance is sought by individuals when their work load increasesTask assistance is offered to others when their work load increasesStructured communication is used to resolve information conflicts and enable all employees to advocate forthe patient (e.g. CUS: “I’m Concerned/I need Clarity, I’m Uncomfortable, Stop this is a patient safetyconcern”)Structured communication is used to resolve personal conflictsStructured communication is used to communicate information that requires immediate attention (e.g.SBAR: Situation Background Assessment Recommendation)Structured communication is used to communicate critical information during emergent situations (e.g. CallOut: Information directed at a responsible individual and conveyed to all to anticipate next steps)Structured communication is used to ensure that information conveyed by a sender is understood by thereceiver (e.g. Check Back)Structured handoff communication is used to transfer information, responsibility and accountability whenpatients transition from department to department or from one hospital to another (e.g. I PASS the BATON)Other (Describe):Learning PracticesProcess MappingIndividual Root Cause AnalysisAggregate Root Cause Analysis of Non-Harmful EventsFailure Mode and Effects AnalysisSafety Briefings (also considered an informal Reporting Practice)Leadership WalkRounds (also considered an informal Reporting Practice)Other (Describe):35
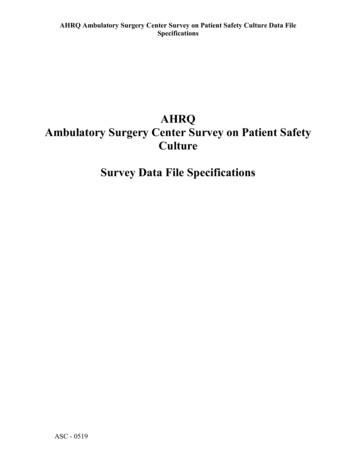
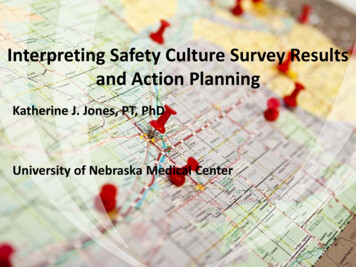
Kirkpatrick’s TaxonomyDefinition: a four-level framework to evaluate theimpact of training programs. The four levels are: (1)learner reactions to the training, (2) changes in learnerknowledge as a result of the training, (3) transfer ofnew knowledge/skill to behavior in work environment,and (4) changes in desired outcomes at the level of theorganization, practitioner, and/or patient.Alliger GM, Tannenbaum SI, Bennett W, Traver H. A meta-analysis of therelations among training criteria. Personnel Psychology. 1997;50:341.See Item Level Over Time to understand relationshipbetween training, knowledge, and behavior changerelative to TeamSTEPPS training.See Benchmark Graph for variation by Adoption ofTeam Behaviors36
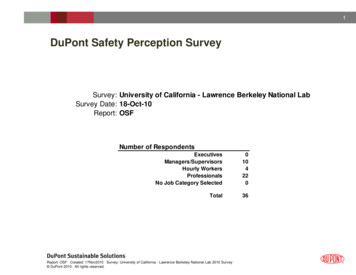
Kirkpatrick’s Taxonomy0%10%No formal team trainingCompleted all TeamSTEPPS modulesCompleted some training in TeamSTEPPS41%0%1%4%Correctly defined Brief9%Correctly defined SBARCorrectly defined CUSCorrectly defined STEP39%2%4%Use SBAR within dept Most of time/AlwaysUse CUS to advocate Most of time/AlwaysUse SBAR or I PASS the BATON across depts Most 26%12%24%Used huddle to adjust plans Most of time/AlwaysUse debrief for improvement Most of time/Always50%KnowledgeTeamSTEPPS Master Trainer40%29%Behavior2012% of Respondents20%30%23%37
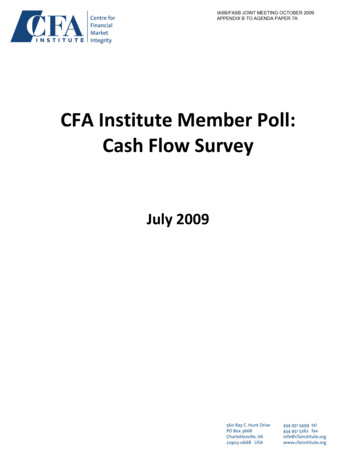
Kirkpatrick’s Taxonomy20122014% of Respondents0% 10% 20% 30% 40% 50% 60% 70% 80%No formal team trainingTeamSTEPPS Master TrainerCompleted all TeamSTEPPS modulesCorrectly defined BriefCorrectly defined SBARCorrectly defined CUSCorrectly defined STEPKnowledgeCompleted some training in TeamSTEPPSUse CUS to advocate Most of time/AlwaysUse SBAR or I PASS the BATON across depts Most Used huddle to adjust plans Most of time/AlwaysBehaviorUse SBAR within dept Most of time/AlwaysUse debrief for improvement Most of time/Always38
Kirkpatrick’s TaxonomyWhy care about Kirkpatrick’s Taxonomy? Training and changes in knowledge account forjust 20% of impact from an intervention Greatest impact is from what leaders do, changein p/p, performance appraisals, what ismeasured, what is role-modeled, rewarded--hard-wired Bottom line: Implementing change must include– Training– Explicit plan to sustain desired behavior changes39
Response Shift BiasDefinition: tendency for an individual to overestimatetheir knowledge, skills, and behaviors in a pretestbecause their understanding of a concept is limitedprior to the program intervention.Pratt, et al. Measuring program outcomes: Using retrospective pretest methodology.American Journal of Evaluation. 2000;21(3):341-349.20072009 201140
Define the problem Match problems to interventions (useInventory of Safe Practices) Create SMART Goals: Specific, Measurable,Achievable, Relevant, and Time bound.HOW DO YOU CREATE AN ACTIONPLAN?41
Interpreting Results to Develop an Action PlanExecutive SummaryBackgroundDefine the problemA. Identify overall strengths, weaknesses, and changes in yourHSOPS scores over timeB. Identify variations within four key components of safety1)2)Work area, job title, team skillsGaps between beliefs and behaviorsC. Relate themes in open-ended comments to survey resultsD. Summarize problems and opportunities for improvement2. Create the appropriate change team3. Define your aims and goals4. Choose measures to monitor implementation
Interpreting Results to Develop an Action Plan5. Review your overall plan (who is doing what, when?)6. Determine how you will sustain and spread changesembedded in your intervention(s)7. Develop a strategy to communicate your surveyresults and action plan to key stakeholders8. Write the final action plan9. Obtain a review and approval of final action plan bykey stakeholders
Action Planning: A Reporting culture is engineered Practices/Tools Successful– Reporting Systems that usereporting systemsstandardized taxonomies– Near miss log– Chart audit– Secret Shopper– Safety Briefings– Leadership WalkRoundsTM– Bulletin board/ suggestionbox/telephone hotline– Nonpunitive– Confidential– Independent– Expert analysis– Timely– Systems-oriented– Responsive
Reporting Action Plan & Aims1. Staff will value reporting of near misses as a way tolearn about system risks without harming patients.a. Goal: Greater than 50% of all respondents will indicate thatnear misses are reported “Always / Most of the Time” at thenext HSOPS reassessmentb. We will do this by implementing the following interventions:i. Conducting quarterly aggregate root cause analyses of “near miss”and non-harmful event reportsii. Discussing near misses during departmental Safety Briefs (includingshift change), huddles, and debriefsiii.Discussing near misses during regular Leadership WalkRoundsc. Identify where this change will occur hospital-wide or aspecific work area?d. Identify when this change will occur
Action Planning: A Just culture is engineered Practices/Tools Understanding human error (Reason 2003, 2006)– Active errors (sharp end)– Latent errorsHuman Factors Just Culture principles and behavior (Marx, 2001)– Conduct: human error, negligence, reckless,intentional rule violation– Shared accountability: managers &individuals/systems & individual behavior– Disciplinary decision-making: outcome-based,rule-based, risk-based Unsafe Acts Algorithm Disruptive Behavior Policy/Standards
UNSAFE ACTS ALGORITHMNOWere the actionsas intended?Evidence of illnessor substance use?NOKnowingly violatedsafe procedures?Pass substitutiontest? (Couldsomeone elsehave done thesame thing)?NOYESHistory ofunsafe acts?NOYESYESWere theconsequencesas intended?YESWere proceduresavailable, workable,intelligible, correctand routinely used?Known medicalcondition?NOYESNODeficiencies intraining, selection,or inexperienced?YESSubstance abusewithout mitigationYESNOYESBlamelesserrorBlameless error,corrective training,counseling indicatedNOSystem inducedviolationYESNOPossible recklessviolationSabotage,malevolent damageCulpableSubstance usewith mitigationSystem inducederrorPossible negligentbehaviorGray AreaBlamelessAdapted from James Reason. (1997). Managing the Risks of Organizational Accidents.
Just Culture Action Plan1. A consistent approach to operationalizing a just andfair culture across the hospital regardless ofprofession or hierarchy.a. Goal: Improve aggregate perceptions of Nonpunitive Response toError by 5% or more at the next HSOPS reassessmentb. We will do this by implementing the following interventions:i. Providing training about human factors and active vs. latent causes of errorsii. Training managers to use Algorithms to balance individual and systemsaccountabilityiii. Training managers to collaborate with human resources and discipline individualsbased on at-risk and reckless behavior and not on outcomesiv. Implement a policy/procedure to manage disruptive behavior.c. Identify where this change will occur hospital-wide or a specific workarea?d. Identify when this change will occur
Action Planning: A Flexible culture is engineered Team Strategies &Tools to EnhancePerformance &Patient Safetyhttp://teamstepps.ahrq.gov Essential component of safetyculture KSAs of teamwork createflexibility and adaptability– Manage complexity– Learn from experience Developed by Dept of Defenseand AHRQ Four key categories of skills 18 specific tools Effective adoption improves allcomponents of safety culture Focus on hard-wiring behaviors– Training/Sustainment 20/80
Flexible Action Plan & Aims3. Use team skills to manage changing workloads.a. Goal: 75% of all respondents will agree thatthey help each other out when it gets busyb. We will do this by teaching staff to use briefs,huddles, debriefs, situation monitoring, andseeking/offering task assistance to managechanging work loads.c. Identify where this change willoccur hospital-wide or a specific work area?d. Identify when this change will occur
Flexible Action Plan & Aims4. Use team skills to make it psychologicallysafe for staff to advocate for patients tothose with more authority.a. Goal: 60% of all respondents will agree thatthey feel free to question the decisions andactions of those with more authority.b. We will do this by teaching staff to use the TwoChallenge Rule and CUS from theTeamSTEPPS mutual support skills.c. Identify where this change will occur hospitalwide or a specific work area?d. Identify when this change will occur
Flexible Action Plan & Aims5. Use team skills to standardize handoffswithin and across hospital departments.a.Goal: Improve Hospital Handoffs & Transitionsby 5% or moreb.We will do this by implementing the followinginterventions:i.Teaching staff to use SBAR when communicatingcritical information that needs immediate attentionii. Teaching staff to use I PASS the BATON whenhanding off responsibility and accountability forpatients across hospital departmentsc.Identify where this change will occur hospitalwide or a specific work area?d.Identify when this change will occur
Action Planning: Reporting, Just, and Flexiblepractices support LearningPractices/Tools Process MappingIndividual RCAAggregate RCAFMEASafety BriefingsLeadershipWalkRoundsTM Close the loop withreporting feedbackUltimately, the willingnessof workers to reportdepends on their beliefthat the organization willanalyze reportedinformation and thenimplement appropriatechange—organizationalpractices support alearning culture.
Learning Action Plan & Aims6. Close the loop with front-line workers about reportedevents and actions taken as a result those events.a. Goals: Improve Organizational Learning and Feedback andCommunication about Error by greater than 5%b. We will do this by implementing the following interventions:I. Providing feedback to font-line staff about the results of individual and aggregateRCAsII. Ensuring relevant front-line staff are involved in conducing individual and aggregateRCA at the unit and department levelIII. Implementing Safety Briefings within unitsIV. Implementing patient safety-focused Leadership WalkRoundsV. Creating a "high reliability academy" for managers; a regular meeting to learn patientsafety principles, human factors, and high reliability concepts using AHRQ PatientSafety Primers available at http://psnet.ahrq.gov/primerHome.aspx .c. Identify where this change will occur hospital-wide or aspecific work area?d. Identify when this change will occur
Role of Leaders in Transformational Change Create a compelling positive vision Concretely define the goal as a performanceproblem not “changing culture” Ensure new behaviors are formally taught ingroups Ensure new behaviors are reinforced– Provide opportunities for practice, coaching, feedback– Be a positive role model Create structures consistent with new way ofthinking/working/behavingSchein, E.H. Organizational Leadership and Culture 4th ed. San Francisco:John Wiley & Sons; 2010.55
Leaders Engineer Culture“ it is the unique function of leadership toperceive the functional and dysfunctionalelements and to manage cultural evolutionand change.”Schein, E.H. OrganizationalLeadership and Culture 4th ed. SanFrancisco: John Wiley & Sons; 2010.56
Contact InformationKatherine Jones, PT, PhDkjonesj@unmc.eduAnne Skinneraskinner@unmc.edu57
Joint Commission 2010 Leadership Standards for hospitals (Standard LD.03.01.01) -Leaders create and maintain a culture of safety -Leaders evaluate the culture on a regular basis -Leaders encourage teamwork; they create structures, processes, and programs to support it National Quality Forum Safe Practice 2: Culture