Transcription
57418 CNE12 sw5/15/0711:05 AMPage 1VOLUME 29 NUMBER 12June 15, 2007A BIWEEKLY PUBLICATION FOR CLINICAL NEUROSURGICALCONTINUING MEDICAL EDUCATIONSpinal Artificial Disc Replacement: Cervical ArthroplastyPart I: History, Design, and Types of Artificial DiscsAlan T. Villavicencio, MD, Sigita Burneikiene, MD, Robert Pashman, MD, andJ. Patrick Johnson, MDLearning Objectives: After reading this article, the participant should be able to:1. Describe the various cervical artificial disc replacement devices currently undergoing experimental clinical trials in the United States.2. Explain the advantages, shortcomings, and controversies related to various cervical artificial disc designs.3. Describe the results of the primary completed clinical trials of cervical artificial discs.This article is the first of two parts.Cervical arthroplasty is a rapidly developing surgical treatment option for degenerative disc disease of the cervical spine.This article reviews design features, indications for cervicalarthroplasty, surgical technique, available preliminary clinical outcomes, and complications of the cervical devices currently being evaluated in FDA-controlled Investigational DeviceExemption (IDE) prospective randomized clinical trials.Neural decompression and arthrodesis have been the mainstays of treatment for many cervical spinal conditions formore than 50 years. Artificial disc replacement surgery allowsfor effective decompression without sacrificing segmentalmotion, theoretically preserving the patient’s functional capacity. The importance of preservation of the spinal motion segment and restoration of normal physiologic biomechanics ofthe cervical spine is becoming increasingly recognized.Arthrodesis alters the biomechanics of the spine, possiblyleading to further degeneration at adjacent levels. Early clinical studies have shown promise, but whether arthroplastyis capable of reducing adjacent level degeneration has not yetbeen proved in long-term prospective clinical trials.History of Cervical ArthroplastyDr. Villavicencio is Director of Research and Development, and Dr.Burneikiene is a Clinical Research Physician, Boulder Neurosurgical Associates, 1155 Alpine Avenue, Suite 320, Boulder, CO 80304;E-mail: atv@bnasurg.com ; Dr. Johnson is Director, Institute forSpinal Disorders, Cedars Sinai Medical Center, Los Angeles, CA,and Dr. Pashman is Director of Scoliosis and Spinal Deformity,Cedars Sinai Medical Center, Los Angeles, CA.Dr. Villavicencio has disclosed that he is/was the recipient ofgrant/research funding from Medtronic Sofamor Danek (as principal investigator in the Maverick Artificial Disc Replacement Trial).Dr. Johnson has disclosed that he is/was a consultant/advisor toSpineWave, Alphatec, Flexuspine, and Johnson & Johnson and is/wasa stock shareholder of SpineWave, Alphatec, Flexuspine, and Pioneer. Dr. Burneikiene and Dr. Pashman have disclosed that they haveno significant relationships with or financial interests in any commercial organizations pertaining to this educational activity.The authors have disclosed that the use of the artificial discs asdescribed in this article for the treatment of cervical disorders hasnot been approved by the U.S. Food and Drug Administration.Lippincott CME Institute, Inc., has identified and resolved all faculty conflicts of interest regarding this educational activity.The first cervical artificial disc prototype was created andimplanted by Fernstrom in 1966. Eight patients had 13 corrosion-resistant, stainless steel ball-shaped prostheses withdiameters of 6 to 10 mm implanted. More extensive experience with the same type of implants was reported by Reitzet al., who performed 75 arthroplasties on 32 patients withintractable headache and cervicobrachialgia. Both studieslacked long-term follow-up, and these artificial discs laterwere abandoned due to problems such as subsidence of thedevice and segmental hypermobility.Proximity to the spinal cord, size constraints, and the functional complexity of the intervertebral disc have slowed thedevelopment of cervical arthroplasty and its implementationinto clinical practice. Interest in cervical arthroplasty underwent a resurgence in the 1990s. The first generation of Cummins-Bristol ball-and-socket, metal-on-metal type implantsCategory: SpineKey Words: Arthroplasty, Cervical artificial disc, Spine surgery
57418 CNE12 sw5/15/0711:05 AMPage 2device. Constrained devices, while minimizing facet loadsand conferring improved stability, typically have a fixed axisof rotation that requires more precise placement.Confirmation of the theoretical advantages of arthroplasty, such as prevention of adjacent level degenerationand mobility preservation, will require long-term followup studies. In addition, the effect of disc height restorationon the facet joints also is not known. Liu et al. performedan in vitro study to evaluate changes in the cervical spinefacet articulation after arthroplasty. When the effect of anincremental increase in disc space height was measured asa change in the facet joint space increase and articulationoverlap, a significant decrease in the facet joint articulationoverlap and joint space increase was found. This studyfound that any increase in disc height from the previousposition could alter biomechanics of the facet joint, whichcould result in subluxation and failure of the artificial disc.Therefore, the importance of disc height restoration or thelack thereof must be judged cautiously until time-provenclinical results become available.Ceramic materials recently have been introduced for usein artificial discs. These can provide excellent wear resistance, but they rely heavily on critical manufacturingprocesses that can result in fractures if defective. Metalalloys and polymers are the materials most commonly usedin spine arthroplasty. Polymers have a higher wear rate butlower stiffness, and they may offer some degree of shockabsorption. Metals wear, corrode, and fracture; therefore,metal alloys are used to balance the unwanted qualities ofone metal with desirable features of another: for example,titanium alloys are valued for their imaging characteristicsand cobalt-chromium has excellent wear properties. Sekhonet al. compared MRI characteristics for the Bryan (MedtronicSofamor Danek), Prodisc-C (Synthes Spine), Prestige LP(Medtronic Sofamor Danek), and PCM (Cervitech) devices.Sagittal and axial T2-weighted MRI views at the implantedand adjacent levels were assessed for quality. The spinalcanal, cord and neuroforamina visualization at the operated levels, as well as image quality at the adjacent levels,was significantly impaired in discs that contained metalswas introduced in 1991, and during a 5-year period, deviceswere implanted at Frenchay Hospital in Bristol, United Kingdom. Among the problems identified with use of this devicewere the excessive disc space distraction required during insertion, with subsequent facet joint separation; the fact that onlya single size was available; limited motion with the device;and screw complications. Nevertheless, it showed enoughpromise to warrant design improvements and eventuallyevolved into the Bristol-Cummins/Frenchay/Prestige discs.Along with the advancement and development of the Bristol-Cummins artificial disc, an American inventor, Bryan,develped a new type of metal-on-plastic artificial disc. The firstBryan cervical disc was implanted in January 2000; since then,more than 6000 patients have been treated with this device.Several cervical arthroplasty devices currently are beingevaluated in FDA-controlled IDE prospective randomizedclinical trials, and a number of new cervical devices are justnow entering the IDE stage of investigation, providing thepossibility that neurosurgeons will have multiple alternatives to cervical fusion in the near future.Artificial Disc DesignThe key features of cervical artificial disc design are thecenter of rotation, short- and long-term stability, and material interfaces. Artificial disc designs are classified as metalon metal, metal-on-polymer composite, ceramic-on-polymercomposite, exclusively polymer composite, or ceramic-onceramic. Both modular and nonmodular devices come inthree types: nonarticulating, uniarticulating, and biarticulating artificial discs. In terms of motion, discs may be categorized as constrained, semiconstrained, unconstrained,or biomimetic (i.e., mimicking physiologic movement). Thisvariety of designs and materials represents an evolution ofdevice patents and incorporation of information from experimental and clinical studies as they become available.Unconstrained devices permit translation, which in theory mimics normal physiologic motion, but they also mayincrease shear and torsional loads on the facet joints. The surrounding soft tissues and the posterior longitudinal ligamentare mainly responsible for stability in an unconstrained typeEDITOR: Ali F. Krisht, M.D.*University of Arkansas for Medical SciencesASSISTANT EDITOR: Cargill Alleyne, Jr., M.D.*Medical College of GeorgiaPRODUCTION ASSISTANT: Ronalda WilliamsEDITORIAL BOARD:Badih Adada, M.D.Ossama Al-Mefty, M.D.Rick Boop, M.D.Evandro de Oliveira, M.D.Allan Friedman, M.D.Gerardo Guinto, M.D.Douglas Kondziolka, M.D.Jacques Morcos, M.D.Tom Origitano, M.D.Nelson Oyesiku, M.D.Kalmon Post, M.D.Richard Rowe, M.D.Martin Weiss, M.D.M. Gazi Yaşargil, M.D.* Dr. Krisht has disclosed that he has no significant relationships with or financial interestsin any commercial organizations pertaining tothis educational activity. Dr. Alleyne hasdisclosed that he is a consultant for Cordis.The continuing education activity in Contemporary Neurosurgery is intended for neurosurgeons, neurologists, neuroradiologists, and neuropathologists.Contemporary Neurosurgery(ISSN 0163-2108) is published bi-weekly by Lippincott Williams & Wilkins, Inc., 16522 Hunters Green Parkway,Hagerstown, MD 21740-2116. Customer Service: Phone (800) 787-8981 or (410) 528-8572. 24-Hour Fax (410)528-4105 or E-mail audrey.dyson@wolterskluwer.com. Visit our website at LWW.com.Copyright 2007 Lippincott Williams & Wilkins, Inc. All rights reserved. Priority Postage paid at Hagerstown, MD, andat additional mailing offices. POSTMASTER: Send address changes to Contemporary Neurosurgery, SubscriptionDept., Lippincott Williams & Wilkins, 16522 Hunters Green Parkway, Hagerstown, MD 21740-2116.Publisher: Daniel E. Schwartz Customer Service Manager: Audrey DysonSubscription rates: Personal: 508.98 US, 553 Foreign. Institutional: 428.98 US, 438 Foreign. In-training: 108.98 US, 113 Foreign. GST Registration Number: 895524239. Send bulk pricing requests to Publisher. Single copies: 17. COPYING: Contents of Contemporary Neurosurgery are protected by copyright. Reproduction, photocopying, and storage ortransmission by magnetic or electronic means are strictly prohibited. Violation of copyright will result in legal action, including civil and/or criminal penalties. Permission to reproduce in any way must be secured in writing from: Permissions Dept.,Lippincott Williams & Wilkins, 351 W. Camden Street, Baltimore, MD 21201; Fax: (410) 528-8550; E-mail: arnetta.queen@wolterskluwer.com. For commercial reprints, E-mail matt.westcoat@wolterskluwer.com.PAID SUBSCRIBERS: Current issue and archives (from 1999) are available FREE online at www.lwwnewsletters.com.Contemporary Neurosurgery is independent and not affiliated with any organization, vendor, or company. Opinions expresseddo not necessarily reflect the views of the Publisher, Editor, or Editorial Board. A mention of products or services does notconstitute endorsement. All comments are for general guidance only; professional counsel should be sought for specificsituations. Indexed by Bio-Sciences Information Services. For information on CME accreditation, see back page.2
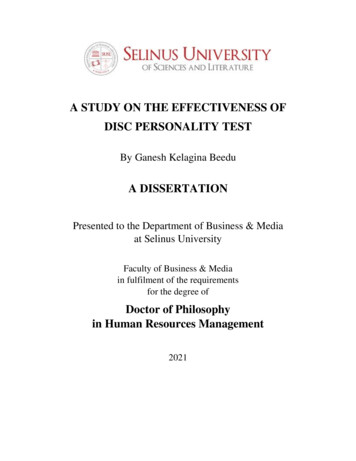
57418 CNE12 sw5/15/0711:05 AMPage 3other than titanium (i.e., PCM, Prodisc-C), compared withthe discs made of titanium (i.e., Bryan, Prestige LP).To address concerns regarding material longevity andwear debris, two devices were tested under physiologicload and motion conditions: a metal-on-metal and a metalon-polymer type. Although the wear debris rate for themetal-on-polymer type device was twice as high as that ofa metal-on-metal type device, both rates were within acceptable limits. Devices tested both in vitro and in vivo (oncethe devices were explanted) showed less wear than predicted. A lesser inflammatory response in metal-on-metalcompared to metal-on-polymer devices was reported. However, wear debris in metal-on-metal discs is composedmainly of heavy metals, and patients with these types ofimplants have been found to have increased serum andurine levels of heavy metals. Long-term clinical or biologiceffects of such deposition are unknown at this time.Various types of keels, teeth, and osteoconductive coatings are used to facilitate short- and long-term fixation ofthe devices. The Bryan cervical disc prosthesis has a porouscoating of titanium to promote bone ingrowth and permanent fixation. In vivo tests confirmed that the prosthesesdemonstrated bony ingrowth despite the lack of postoperative immobilization. Osteoconductive finishes such as calcium phosphate hydroxyapatite also may result indebonding, extra wear debris, and, possibly, osteolysis.Another critical feature is the localization of the axis ofrotation in artificial discs and whether it matches the physiologic center of rotation of an implanted segment. Thephysiologic center of rotation in the cervical spine has shownlevel-to-level differences, but it usually is located in the posterior half of the upper portion of the inferior vertebral body.Some discs, especially those with a ball-and-socket design,have a fixed axis of rotation in the center of the disc andmust be placed slightly posterior to match physiologic kinematics and avoid facet overloading. Other manufacturersclaim that the normal center of rotation can be reproducedwith an unconstrained type of disc design.Types of Cervical Artificial Discs Under InvestigationCurrently, no cervical artificial discs have been FDAapproved and, consequently, none is available for implantation in the United States. All of the cervical devices currently are being evaluated in FDA-controlled IDEprospective randomized clinical trials.Bryan DiscThe Bryan cervical artificial disc consists of a low frictionelastic polymer nucleus and two anatomically shaped titanium alloy shells equipped with anterior rigid wings to prevent posterior migration. A flexible membrane forms a sealedspace that contains saline to diminish friction and wear. Thisis a rotationally unconstrained type of design with a mobileaxis of rotation, which allows 11 degrees in flexion/extensionor lateral bending and 2 mm in translation. Five sizes areavailable, from 14 to 18 mm in diameter. The disc articulatesvia symmetric spherical bearing surfaces and has a porousABFigure 1. Plain lateral x-rays demonstrating straight sagittal alignment (lordosis 0 degrees) before surgery (A) and kyphosis (–5 degrees)after implantation of the Bryan artificial disc (B).3
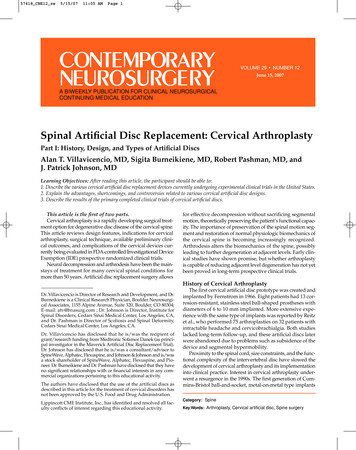
57418 CNE12 sw5/15/0711:05 AMPage 4titanium coating on bone-contacting surfaces of the shells,which promotes high friction between bone and shells, therebyensuring initial stability of the device and supporting bonyin-growth, with subsequent long-term stability.The first Bryan disc was implanted in the United Statesin May 2002 under IDE status. Patients enrolled in the studywere randomized to receive either an artificial disc or fusionwith the Atlantis anterior cervical plate (Medtronic SofamorDanek). Preliminary results reported from one clinical sitewith a mean follow-up period of 19 months demonstratedequivalent clinical outcomes in both groups. This studyfound no device-related complications or osteophyte bridging; however, a few cases of spontaneous fusion have beenalready reported from other sites.During surgery, endplates are prepared to provide a perfect fit for the device shells. Although manufacturers of thedevice claim that the Bryan disc potentially can restore discheight and sagittal alignment, Johnson et al. demonstratedthat the amount of endplate removed during the millingprocess results in actual loss of lordosis and vertebral height(Figure 1). A mean loss of 4.7 degrees of lordosis was reportedfor patients who underwent a single-level arthroplasty procedure. Even greater loss of lordosis was confirmed by Fonget al, who found that nine of 10 patients had kyphotic postoperative endplate angles, with a mean change of 7 degreestoward kyphosis. This correlation was significant with functional spinal unit height reduction, which averaged 1.7 mm.Pickett et al. demonstrated a mean change of 8.2 degrees,which resulted in kypnotic angulation of the functional spinalunit in all 14 patients. Loss of lordosis could have a negative impact on long-term clinical outcomes, even with excellent or good results initially, which could be attributed tothe decompression portion of the procedure.ProDisc-CThe design of the ProDisc-C is similar to that of the lumbar ProDisc prosthesis and consists of two forged cobaltchromium-molybdenum alloy endplates and a polyethyleneinlay component fixed to the inferior endplate. The two metalendplates are covered with a plasma-sprayed pure titaniumcoating to help ensure long-term stability, in addition to thecentral keels that initially provide stability of the implant.This modular device is inserted as a one-piece construct. Itcomes in five anatomic footprint sizes and four heights.Multiple centers in the United States currently areinvolved in a prospective, randomized clinical trial evaluating the safety and efficacy of the ProDisc-C comparedwith anterior cervical discectomy and fusion (ACDF). Preliminary results demonstrated no statistically significantdifferences between ACDF and arthroplasty patient groupswith regard to neurologic function, including scores on theVisual Analogue Scale, Neurologic Disability Index, or ShortForm-36 General Health Survey. An increase of overallmotion was achieved in flexion (3.2 degrees) and extension(7.0 degrees), with lateral bending decreased by 5.5 degrees.PCM DiscThe PCM (“porous-coated motion”) disc was developedin collaboration with cervical spine surgeons from the UnitedStates, Europe, and Brazil and was approved for clinical trials in the United States in December 2004.Two modifications of the PCM disc were developed toaddress the destabilizing effect of resection of the posterior longitudinal ligament (PLL)—a low-profile PCM disc for patientsin whom the PLL is preserved, and a fixed PCM disc withscrews for use when the PLL is removed. This artificial discdesign consists of two cobalt-chrome alloy endplates with anintervening low friction, ultra-high-molecular-weight polyethylene spacer. The spacer allows the upper endplate to slideand rotate forward and backward relative to the lower endplate. A rectangular shape is used to maximize support in thelateral areas. The endplates have serrated surfaces with a titanium-calcium phosphate bony ingrowth coating to enhancepostoperative stability. Two layers of pure titanium plasma aresprayed onto the back of the endplates, followed by an electrochemically applied calcium phosphate hydroxyapatite layer.Biomechanical studies have demonstrated axial rotation slightlyhigher than physiologic and limited (85% to 95%) flexion/extension range of motion for this semiconstrained device.Prestige DiscsTwo modifications of the Prestige disc design currently areavailable—Prestige ST and Prestige LP. New design featuresin the latest generation of Prestige LT disc look promising.The prosthesis is made from a new titanium ceramic composite material that has improved wear characteristics and isimage-friendly on CT and MRI scans. Long-term stability isachieved through a porous titanium spray coating in addition to dual rails on each component, which facilitate the initial implant’s stability. These elements replace the screws thatpreviously were used to affix the device components to thebone. The disc comes in various sizes to accommodate variations in patient size and consists of two articulating components, a ball on the top and a trough on the bottom.At the time this article was written, enrollment was completed for the Prestige LP clinical study, and preliminaryclinical outcome results for the Prestige ST disc had beenpresented at the Annual Meeting of the American Association of Neurological Surgeons. A total of 120 patients hadparticipated in this prospective clinical trial and were randomized (50/50) to the standard treatment of cervical discectomy and fusion or cervical discectomy followed byimplantation of the Prestige ST artificial cervical disc. Preliminary results demonstrated equal clinical outcomes inboth groups, which confirmed previously reported resultsfor the Prestige II artificial disc.Kineflex C DiscThe Kineflex C disc (SpinalMotion) has a mobile bearingdesign, which allows translational movements within limitsdefined by the retention rings. This metal-on-metal disc comesin two sizes and has a locating fin for initial stability (Figure 2).It was used previously in South Africa, but no clinical data reporting clinical experience are available at the time of this writing.Mobi-C Cervical DiscThe Mobi-C (LDR Medical) is the only implant that hasbeen approved for clinical investigation at both one and twolevels in the cervical spine. The Mobi-C uses a self-centeringmobile bearing and semiconstrained design that allows 6degrees of freedom along with a supposedly more-naturalrange of motion (Figure 3). Two peripheral stops incorporated4
57418 CNE12 sw5/15/0711:05 AMPage 5on the inferior plate along with spine compression control system limit the insert’s mobility and theoretically could preventmigration of the device. Initial stability is achieved with thehelp of lateral self-retaining teeth, which have an inclinedshape to facilitate easier insertion of the device and provideanchorage thereafter. The self-centering feature insures selfpositioning of the superior plate vs. the inferior plate, whichalso can simplify device implantation.Secure-C DiscCurrently undergoing clinical trails, the Secure-C (GlobusMedical) disc consists of three parts: two metal, cobalt-chromealloy endplates with porous coated bone-contacting surfacesand a semiconstrained ultra-high-molecular-weight polyethylene core. The clinical study is expected to involve almost400 participants, including 100 nonrandomized training cases.Figure 2. Kineflex C disc (SpinalMotion).CerviCore DiscThe CerviCore disc (Stryker Spine) has a saddle-shaped,metal-on-metal design (Figure 4) with dual centers of rotation. The plates are coated with a titanium spray and havethree spikes that provide initial fixation of the device to thebone. This disc recently has entered a phase of clinical evaluation in U.S. clinical trials.Cerpass DiscThe Cerpass (NuVasive), an original ceramic-on-ceramicdisc, is awaiting FDA approval for investigation. The manufacturers of this device believe that it will provide betterdurability and eliminate potential problems of wear debris.This design incorporates self-centering features that shouldensure correct placement during implantation.ReadingsCoric DF, Finger, Boltes P. Prospective randomized controlled study of theBryan cervical disc: early clinical results from a single investigational site.J Neurosurg Spine 2006;4:31-35.Cummins B H, Robertson JT, Gill SS. Surgical experience with an implantedartificial cervical joint. J Neurosurg 1998;88:943-948.DiAngelo DJ, Foley KT, Morrow BR, et al. In vitro biomechanics of cervicaldisc arthroplasty with the ProDisc-C total disc implant. Neurosurg Focus2004;17(3): E7.Fong SY, DuPlessis SJ, Casha S, Hulbert RJ. Design limitaions of Bryan discarthroplasty. Spine J 2006; 6:233-241.Johnson JP, Lauryssen C, Cambron HO, et al. Sagittal alignment and theBryan cervical artificial disc. Neurosurg Focus 2004; 17(6): E14.Leung C, Casey AT, Goffin J, et al. Clinical significance of heterotopic ossification in cervical disc replacement: a prospective multicenter clinical trial.Neurosurgery 2005;57:759-763.Liu JN, Ebraheim A, Haman SP, et al. How the increase of the cervical disc spaceheight affects the facet joint: an anatomy study. Spine 2006;31:E350-354.Mummaneni PV, Haid RW. The future in the care of the cervical spine: interbody fusion and arthroplasty. Invited submission from the Joint Section Meeting on Disorders of the Spine and Peripheral Nerves, March 2004. J NeurosurgSpine 2004;1:155-159. Oskouian RJ, Whitehill R, Samii A, et al. The future ofspinal arthroplasty: a biomaterial perspective. Neurosurg Focus 2004; 17(3):E2.Pickett GE, Rouleau JP, Duggal N, et al. Kinematic analysis of the cervical spinefollowing implantation of an artificial cervical disc. Spine 2005;30:1949-1954.Porchet F, Metcalf NH. Clinical outcomes with the Prestige II cervical disc:preliminary results from a prospective randomized clinical trial. Neurosurg Focus 2004;17:E6.Sekhon LHS, Duggal N, Lynch JJ, et al. Magnetic resonance imaging clarityof the Bryan, Prodisc-C, Prestige LP, and PCM cervical arthroplasty devices.Spine 2007;32:673-680.Figure 3. Mobi-C disc (LDR Medical).Figure 4. CerviCore disc (Stryker Spine).5
57418 CNE12 sw5/15/0711:05 AMPage 6To earn CME credit, you must read the CME article and complete the quiz on the enclosed form, answering at least 70% of the quizquestions correctly. Select the best answer and use a blue or black pen to completely fill in the corresponding box on theenclosed answer form. Please indicate any name and address changes directly on the answer form. If your name and address do notappear on the answer form, please print that information in the blank space at the top left of the page. Make a photocopy of the completedanswer form for your own files and mail the original answer form in the enclosed postage-paid business reply envelope. Your answerform must be received by Lippincott CME Institute, Inc., by June 14, 2008. At the end of each quarter, all CME participants will receiveindividual issue certificates for their CME participation in that quarter.These individual certificates will include your name, the publicationtitle, the volume number, the issue number, your participation date, and the AMA credit awarded. For subscribers who elect to participatein the CNE program for AANS credit, each certificate will also include the official AANS credit statement. For more information, call (800)787-8981.Online quiz instructions: To take the quiz online, go to http://cme.LWWnewsletters.com, and enter your username and password.Your username will be the letters LWW (case sensitive) followed by the 12-digit account number on your mailing label. You mayalso find your account number on the paper answer form mailed with your issue. Your password will be 1234; this password maynot be changed. Follow the instructions on the site.You may print your official certificate immediately. Please note: Lippincott CMEInstitute, Inc., will not mail certificates to online participants.Lippincott Continuing Medical Education Institute, Inc., is accredited by the Accreditation Council for Continuing Medical Educationto provide continuing medical education for physicians.Lippincott Continuing Medical Education Institute, Inc., designates this educational activity for a maximum of 1.5 AMA PRA Category1 Credits . Physicians should only claim credit commensurate with the extent of their participation in the activity. The AmericanAssociation of Neurological Surgeons attests that this educational activity has been recognized for co-sponsored/endorsement for1.5 Category 1 CME credits of the American Association of Neurological Surgeon’s Continuing Education Award in Neurosurgery.Lippincott CME Institute, Inc., will continue to provide the American Association of Neurological Surgeons, in February of each year,with an annual listing of the participants and their CME credits earned.1.The first cervical artificial disc was implanted by Reitz.6.True or False?2.True or False?The main goals of the arthroplasty procedure are preservation of the motion segment and flexibility.7.True or False?3.8.The Bryan cervical artificial disc is a rotationally unconstrainedtype of artificial disc with a mobile axis of rotation.True or False?Unconstrained artificial discs have a fixed axis of rotation.9.True or False?5.A fixed axis of rotation in the center of the disc perfectlymatches physiologic kinematics of an implanted segment.True or False?Three key aspects of cervical artificial disc design are thecenter of rotation, short- and long-term stability, and material interfaces.True or False?4.Metal-on-polymer discs have a higher inflammatory responsethan metal-on-metal devices.The Bryan cervical disc restores physiologic sagittal alignment.True or False?Metal alloys and polymers are the materials most commonlyused in spine arthroplasty.10. Cervical artificial discs that have been evaluated so far inFDA-controlled Investigational Device Exemption prospectiverandomized clinical trials have demonstrated superior clinical outcomes compared with cervical fusion.True or False?True or False?6
Bryan cervical disc was implanted in January 2000; since then, more than 6000 patients have been treated with this device. Several cervical arthroplasty devices currently are being evaluated in FDA-controlled IDE prospective randomized clinical trials, and a number of new cervical devices are just