Transcription
SPINE Volume 26, Number 5, pp E93–E113 2001, Lippincott Williams & Wilkins, Inc.Nomenclature and Classification of LumbarDisc PathologyRecommendations of the Combined Task Forces of the NorthAmerican Spine Society, American Society of Spine Radiology, andAmerican Society of NeuroradiologyDavid F. Fardon, MD,* and Pierre C. Milette, MD†PrefaceStandardization of language is difficult, especially amongthose who have expert knowledge of the subject andclear understanding of what their own words mean. Thedifficulties must be overcome because deleterious effectsensue when we do not understand what one another’swords mean. Existing dictionary definitions and previousefforts by experts have lacked the attention to detail andmultidisciplinary consensus we brought to this work.The North American Spine Society (NASS) initiatedefforts to develop detailed definitions of lumbar disc pathology terms and has provided sustained support of theproject. Independent efforts by neuroradiologists led theAmerican Society of Spine Radiology (ASSR) and American Society of Neuroradiology (ASNR) to organize atask force of neuroradiologists and encourage liaisonwith the NASS group. The results are this document andimproved communications between the societies.The Board of Directors of NASS, and the ExecutiveCommittees of both ASSR and ASNR have endorsed thisdocument, as has the Joint Section on Disorders of theSpine and Peripheral Nerves of the American Associationof Neurological Surgeons (AANS) and Congress of Neurological Surgeons (CNS), and the CPT and ICD CodingCommittee of the American Academy of OrthopaedicSurgeons (AAOS). Endorsement by other North American, European, and international societies is currentlypending. This work is being simultaneously posted to thewebsite of the journal Spine and on the ASSR and ASNRwebsites owing to special arrangements between the editors and publisher of Spine and the American Journal ofNeuroradiology (AJNR).The hope of all of us who have worked on this projectis that it will ultimately improve the care of patients withspinal disorders.David F. Fardon, MD, Chairperson, Clinical TaskForcePierre C. Milette, MD, Chairperson, Imaging TaskForce*Chairperson, Clinical Task Force. †Chairperson, Imaging TaskForce.See the appendix for a complete listing of the members of the TaskForces and consultants and advisors.IntroductionPhysicians need reliable terms that describe normal andpathologic conditions of lumbar discs. Terms that can beinterpreted accurately, consistently, and with reasonableprecision are particularly important for communicatingimpressions gained from imaging for clinical diagnosticand therapeutic decision making. Although clear understanding of disc terminology between radiologists andclinicians is the focus of this work, such understandingcan be critical, also, to patients, families, employers, insurers, jurists, social planners, and researchers.In 1995, a multidisciplinary task force from the NorthAmerican Spine Society (NASS) addressed deficiencies instandardization and current practice of the language defining conditions of the lumbar disc. It cited several documentations of the problem3–5,13,14,16,28 and made detailed recommendations for standardization. Its workwas published in a copublication of NASS and the American Academy of Orthopedic Surgeons (AAOS).15 Thework has not been otherwise endorsed by major organizations and has not been recognized as authoritativeby radiology organizations. Many previous2,4,13,27–29,31,33,39,43– 45,46,49and some subsequent12,19,22,24,25,26efforts have addressed the issues, but have been of morelimited scope, and none has gained widespread compliance or formal endorsement.Although the NASS 1995 effort has been the mostcomprehensive to date, it remains deficient in clarifyingsome controversial topics, lacking in its treatment ofsome issues, and does not provide recommendations forstandardization of classification and reporting. To address the remaining needs, and in hopes of securing endorsement sufficient to result in universal standardization, joint task forces were formed by NASS, theAmerican Society of Neuroradiology (ASNR), and theAmerican Society of Spine Radiology (ASSR). This workis the product of those task forces.A few general principles guided the generation of thisdocument. The definitions should be based on the anatomy and pathology. Recognizing that some criteria, under some circumstances, may be unknowable to the observer, the definitions of diagnoses should not bedependent on or imply value of specific tests. The definitions of diagnoses should not define or imply externaletiologic events such as trauma. The definitions of diagnoses should not imply relationship to symptoms. DefiE93
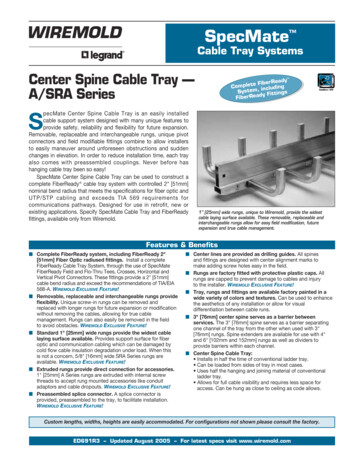
E94 Spine Volume 26 Number 5 2001nitions of diagnoses should not define or imply need forspecific treatment.The task forces worked from a model that could beexpanded from a primary purpose of providing understanding of reports of imaging studies. The result wouldprovide a simple and relatively imprecise classification ofdiagnostic terms, based on pathology, which could beexpanded, without contradiction, into more precise subclassifications. When reporting pathology, degrees of uncertainty would be labeled as such rather than compromising on the definitions of the terms.All terms used in the classifications and subclassifications were to be defined, and those definitions would beadhered to throughout the model. For practical purpose,some existing English terms were given meanings different from those found in some contemporary dictionaries.The task forces would provide a list and classification ofrecommended terms, but, recognizing the nature of language practices, would discuss, and include in a glossary,commonly used and misused nonrecommended termsand nonstandard definitions.Although the principles and most of the definitions ofthis document could be easily extrapolated to the cervical and dorsal spine, the focus is on the lumbar spine.While clarification of terms related to posterior elementsand disorders related to dimensions of the spinal canalare also needed, this work is limited to discussion of thedisc. Although it is not always possible to fully discussthe definition of anatomic and pathologic terms withoutsome reference to symptoms and etiology, the definitions, themselves, stand the test of independence frometiology, symptoms, or treatment. Because of the focuson anatomy and pathology, this work does not definecertain clinical syndromes that may be related to lumbardisc pathology.Guided by those principles, this document provides auniversally acceptable nomenclature that is workable forall forms of observation, that addresses contour, content,integrity, organization, and spatial relationships of thelumbar disc; and that serves a system of classification andreporting built on that nomenclature.RecommendationsThese recommendations present diagnostic categoriesand subcategories, intended for classification and the reporting of imaging studies. The terminology usedthroughout these recommended categories and subcategories remains consistent with detailed explanationsgiven in the Discussion section and with the preferreddefinitions presented in the Glossary.The diagnostic categories are based on pathology.Each lumbar disc can be classified in terms of one, andoccasionally more than one, of the following diagnosticcategories: Normal; Congenital/Developmental Variation; Degenerative/Traumatic; Infectious/Inflammatory;Neoplastic; and/or Morphologic Variant of UncertainSignificance (Table 1). Each diagnostic category can besubcategorized to various degrees of specificity accord-Table 1. General Classification of Disc Lesions* Normal (excluding aging changes) Congenital/developmental variant Degenerative/traumatic lesionAnular generationSpondylosis deformansIntervertebral osteochondrosis Inflammation/infection Neoplasia Morphologic variant of unknown significance*Adapted with permission from Milette PC. Classification, diagnostic imaging,and imaging characterization of a lumbar herniated disc. Radiol Clin North AM2000;38:1267–1292.ing to the information available and purpose to beserved. The data available for categorization may leadthe reporter to characterize the interpretation as “possible,” “probable,” or “definite.”NormalNormal defines young discs that are morphologicallynormal, without consideration of the clinical context andnot inclusive of degenerative, developmental, or adaptivechanges that could, in some contexts (e.g., normal aging,scoliosis, spondylolisthesis) be considered clinically normal. However, the bilocular appearance of the adult nucleus resulting from the development of a central horizontal band of fibrous tissue is considered a sign ofnormal maturation.Congenital/Developmental VariationThe Congenital/Developmental Variation category includes discs that are congenitally abnormal or that haveundergone changes in their morphology as an adaptationto abnormal growth of the spine such as from scoliosis tive and/or Traumatic changes in the disc areincluded in a broad category that includes subcategoriesof Anular Tear; Herniation; and Degeneration. Characterization of this group of discs as Degenerative/Traumatic does not imply that trauma is necessarily afactor or that degenerative changes are necessarilypathologic as opposed to the normal aging process.Anular tears, also properly called anular fissures, areseparations between anular fibers, avulsion of fibersfrom their vertebral body insertions, or breaks throughfibers that extend radially, transversely, or concentrically, involving one or many layers of the anular lamellae. The terms “tear” or “fissure” describe the spectrumof such lesions and do not imply that the lesion is consequent to trauma (Figure 1).Degeneration may include any or all of real or apparent desiccation, fibrosis, narrowing of the disc space,diffuse bulging of the anulus beyond the disc space, extensive fissuring (i.e., numerous anular tears), and muci-
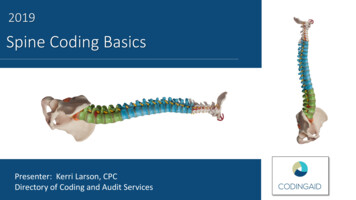
Lumbar Disc Pathology: Recommendations North American Spine Society et al E95Figure 1. Schematic sagittal anatomic sections showing the differentiating features of an anular tear (radial tear in this case) anda disc herniation. The term “tear” is used to refer to a localizedradial, concentric, or horizontal disruption of the anulus withoutassociated displacement of disc material beyond the limits of theintervertebral disc space. Nuclear material is shown in black, andthe anulus (internal and external) corresponds to the white portionof the intervertebral space. The same convention is used in Figures 2, 11, 12, and 13. (Adapted with permission from Milette PC.The proper terminology for reporting lumbar intervertebral diskdisorders. AJNR Am J Neuroradiol 1997; 18: 1859 –1866.)nous degeneration of the anulus, defects and sclerosis ofthe endplates, and osteophytes at the vertebral apophyses. A disc demonstrating one or more of these degenerative changes can be further qualified into two subcategories: spondylosis deformans, possibly representingchanges in the disc associated with a normal aging process;or intervertebral osteochondrosis, possibly the consequences of a more clearly pathologic process (Figure 2).Herniation is defined as a localized displacement ofdisc material beyond the limits of the intervertebral discspace (Figure 1). The disc material may be nucleus, cartilage, fragmented apophyseal bone, anular tissue, or anycombination thereof. The disc space is defined, craniadand caudad, by the vertebral body endplates (Figure 3)and, peripherally, by the outer edges of the vertebral ringapophyses, exclusive of osteophytic formations (FigureFigure 2. Schematic sagittal anatomic sections showing the differentiating characteristics of the normal disc, spondylosis deformans, and intervertebral osteochondrosis. The distinction between these three entities is usually possible on all imagingmodalities, including conventional radiographs. (Adapted withpermission.25)Figure 3. The term “herniated disc,” as defined in this work, refersto localized displacement of nucleus, cartilage, fragmented apophyseal bone, or fragmented anular tissue beyond the intervertebral disc space (disc space, interspace). The interspace isdefined, craniad and caudad, by the vertebral body endplates. Twointravertebral herniations, one with an upward orientation and theother with a downward orientation with respect to the disc space,are illustrated schematically.4). The term “localized” contrasts to “generalized,” thelatter being arbitrarily defined as greater than 50% (180degrees) of the periphery of the disc (Figure 5).Localized displacement in the axial (horizontal) planecan be “focal,” signifying less than 25% of the disc circumference (Figure 6), or “broad-based,” meaning between 25 and 50% of the disc circumference (Figure 7).Presence of disc tissue “circumferentially” (50 –100%)beyond the edges of the ring apophyses may be called“bulging” and is not considered a form of herniation(Figure 8), nor are diffuse adaptive alterations of discFigure 4. The interspace is defined, peripherally, by the edges ofthe vertebral ring apophyses, exclusive of osteophytic formations.The line drawing schematically illustrates a localized extension ofdisc material beyond the intervertebral disc space, in a left posterior direction, which qualifies as a disc herniation.
E96 Spine Volume 26 Number 5 2001Figure 5. For classification purposes, the intervertebral disc is considered as a two-dimensional round or oval structure having four 90 quadrants. By convention, a herniation is a “localized” process involving less than 50% (180 ) of the disc circumference.contour secondary to adjacent deformity as may bepresent in severe scoliosis or spondylolisthesis (Figure 9).Herniated discs may take the form of protrusion orextrusion, based on the shape of the displaced material(Figure 10). Protrusion is present if the greatest distance,in any plane, between the edges of the disc material beyond the disc space is less than the distance between theedges of the base, in the same plane. The base is definedas the cross-sectional area of disc material at the outermargin of the disc space of origin, where disc materialdisplaced beyond the disc space is continuous with discmaterial within the disc space. In the cranio-caudal direction, the length of the base cannot exceed, by definition, the height of the intervertebral space. Extrusion ispresent when, in at least one plane, any one distanceFigure 6. By convention, a “focal herniation” involves less than25% (90 ) of the disc circumference.Figure 7. By convention, a “broad-based” herniation involves between 25% and 50% (90 –180 ) of the disc circumference.between the edges of the disc material beyond the discspace is greater than the distance between the edges ofthe base, or when no continuity exists between the discmaterial beyond the disc space and that within the discspace (Figure 11). Extrusion may be further specified assequestration, if the displaced disc material has lost completely any continuity with the parent disc (Figure 12).The term migration may be used to signify displacementof disc material away from the site of extrusion, regardless of whether sequestrated or not (Figure 13). Becauseposteriorly displaced disc material is often constrainedby the posterior longitudinal ligament, images may portray a disc displacement as a protrusion on axial sectionsFigure 8. Symmetrical presence (or apparent presence) of disctissue “circumferentially” (50 –100%) beyond the edges of the ringapophyses may be described as a “bulging disc” or “bulgingappearance” and is not considered a form of herniation. Furthermore, “bulging” is a descriptive term for the shape of the disccontour and not a diagnostic category.
Lumbar Disc Pathology: Recommendations North American Spine Society et al E97Figure 9. Asymmetrical bulging of the disc margin (50 –100%),such as what is found in severe scoliosis, is also not considereda form of herniation.and an extrusion on sagittal sections, in which cases thedisplacement should be considered an extrusion. Herniated discs in the cranio-caudal (vertical) directionthrough a break in the vertebral body endplate are referred to as intravertebral herniations.Disc herniations may be further specifically describedas contained, if the displaced portion is covered by outeranulus, or uncontained when absent any such covering.Displaced disc tissues may also be described by location,volume, and content, as discussed later in this document.Table 2 lists the proposed categories for description andclassification of disc herniations.Inflammation/Infection The category of Inflammation/Infection includes infection, infection-like inflammatorydiscitis, and inflammatory response to spondyloarthropathy. It also includes inflammatory spondylitis ofsubchondral endplate and bone marrow manifested asModic Type 1 magnetic resonance imaging (MRI)changes and usually associated with pathologic changesin the disc. To simplify the classification scheme, theFigure 10. Herniated discs may take the form of protrusion orextrusion, based on the shape of the displaced material (seedefinitions in text).Figure 11. When a relatively large amount of disc material isdisplaced, distinction between protrusion (A) and extrusion (B orC) will generally only be possible on sagittal magnetic resonance(MR) sections or sagittal computed tomography (CT) reconstructions. C, Although the shape of the displaced material is similar tothat of a protrusion, the greatest cranio-caudal diameter of thefragment is greater than the cranio-caudal diameter of its base atthe level of the parent disc, and the lesion therefore qualifies as anextrusion. In any situation, the distance between the edges of thebase, which serves as reference for the definition of protrusionand extrusion, may differ from the distance between the edges ofthe aperture of the anulus, which cannot be assessed on CTimages and is seldom appreciated on MR images. In the craniocaudal direction, the length of the base cannot exceed, by definition, the height of the intervertebral space. (Reprinted withpermission from Milette PC. Classification, diagnostic imaging andimaging characterization of a lumbar herniated disc. Radiol ClinNorth Am 2000; 38:1267–1292.)category is inclusive of disparate conditions; therefore,when data permit, the diagnosis should be subcategorized for appropriate specificity.NeoplasiaPrimary or metastatic morphologic changes of disc tissues caused by neoplasia are categorized as Neoplasia,with subcategorization for appropriate specificity.Figure 12. Schematic representation of various types of posteriorcentral herniations. A, Small subligamentous herniation (or protrusion) without significant disc material migration. B, Subligamentous herniation with downward migration of disc material underthe posterior longitudinal ligament (PLL). C, Subligamentous herniation with downward migration of disc material and sequesteredfragment (arrow). (Reprinted with permission from Milette PC.Classification, diagnostic imaging and imaging characterization ofa lumbar herniated disc. Radiol Clin North Am 2000; 38:1267–1292.)
E98 Spine Volume 26 Number 5 2001ture that facilitates description of surgical or endoscopicfindings as well as images; and also, with the caveat thatit addresses only the morphology of the disc, it facilitatescommunication for patients, families, employers, insurers, and legal and social authorities, and permits accumulation of more reliable data for research.Figure 13. Relationship of typical posterior disc herniations withthe posterior longitudinal ligament. A, Midline sagittal section:Unless very large, a posterior midline herniation usually remainsentrapped underneath the deep layer of the PLL and sometimes afew intact outer anulus fibers joining with the PLL to form a“capsule.” The deep layer of the PLL (arrow) also attaches to theposterior aspect of the vertebral body so that no potential spaceis present underneath. B, Sagittal para-central section: The PLLextends laterally at the disc level (arrowhead) but, above andbelow the disc, an anterior epidural space (as), where disc fragments are frequently entrapped, is present between the lateral(peridural) membranes and the posterior aspect of the vertebralbodies. (Adapted with permission from Milette PC. Classification,diagnostic imaging and imaging characterization of a lumbar herniated disc. Radiol Clin North Am 2000;38:1267–1292.)Morphologic Variant of Unknown SignificanceInstances in which data suggest abnormal morphology ofthe disc but are not complete enough to warrant a diagnostic categorization can be categorized as MorphologicVariant of Unknown Significance.DiscussionAcceptance and standardization occur most easily whenrecommendations are close to common practice. However, there are many contradictory views of commonpractice and some common practices are contradictoryto our primary purpose, which is clear communicationbetween those who interpret images and those who makeclinical decisions.This document defines a nomenclature that describesdiscs and leaves to the clinician the description of thepatient. In so doing, however, this provides a nomenclaTable 2. Description of a Disc Herniation MorphologyProtrusionExtrusionIntravertebral Containment Continuity Relation with PLL complex Volume Composition LocationNormalCategorization of a disc as “Normal” means the disc isfully and normally developed and free of any changes ofdisease, trauma, or aging. Only the morphology, and notthe clinical context, is considered. In common practice,people with a variety of harmless congenital or developmental variations of discs, minor bulging of anuli, anterior and lateral marginal vertebral body osteophytes, etc.are normal people. By this nomenclature and classification, however, such individual discs are not considered“normal.” Therein lies a significant difference of thismethod from what many would consider common practice. Some people are clinically “normal” even thoughthey have morphologically abnormal discs.Anular Tears/FissuresThere is general agreement about the various forms ofloss of integrity of the anulus, such as radial, transverse,and concentric separations. Some, including the 1995NASS document,15 have recommended that such lesionsbe termed “fissures” rather than “tears,” primarily forfear that the word “tear” could be misconstrued as implying a traumatic etiology. Common practice, as documented by review of contemporary specialty journal literature12 shows preference, among authors of variousdisciplines, for the term “tear,” and frequent synonymous use in the same articles of the terms “tear” and“fissure.”In this instance, it is unwise to recommend contrary toingrained common usage but wise to reiterate the caveatthat the term “anular tear” does not imply traumaticetiology. In the case where a single, traumatic event isclearly the source of loss of integrity of a formally normalanulus, such as with documentation and findings of violent distraction injury, the term “rupture” of the anulusis appropriate, but use of the term “rupture” as synonymous with commonly observed tears or fissures is contraindicated. In conclusion, therefore, “anular tear” and“anular fissure” are both acceptable terms, can be usedproperly as synonyms, and do not imply that a significanttraumatic event has occurred or that the etiology isknown.Some tears may have clinical relevance and othersmay be asymptomatic and inconsequential componentsof the aging process. Correlation of the characteristics ofthe tear with responses to discography and other clinically relevant observations may enable the observer tomake such distinctions, but such is beyond the scope ofthis morphologically based definition and classificationmodel.
Lumbar Disc Pathology: Recommendations North American Spine Society et al E99Disc DegenerationBecause there is confusion in differentiation of changes ofpathologic degenerative processes in the disc from thoseof normal aging,8,30,38 the classification category “Degenerative/Traumatic” includes all such changes, thusdoes not compel the observer to differentiate the pathologic from the normal consequences of aging. However,this model allows the observer with adequate data topresent a more enlightening report by making such adistinction, with appropriate notation of the degree ofconfidence.Perceptions of what constitutes the normal aging process of the spine have been greatly influenced by postmortem anatomic studies involving a limited number of specimens, harvested from cadavers from different age groups,with unknown past medical histories, and the presumption of absence of lumbar symptoms.7,9,17,20,23,34 Withsuch methods, pathologic changes are easily confusedwith consequences of normal aging. Resnick and Niwayama35 emphasized the differentiating features of twodegenerative processes involving the intervertebral disc,which had been previously described by Schmorl andJunghanns37: “spondylosis deformans,” which affects essentially the anulus fibrosus and adjacent apophyses, and“intervertebral osteochondrosis,” which affects mainlythe nucleus pulposus and the vertebral body endplates,but also includes extensive fissuring (numerous tears) ofthe anulus fibrosus, which may be followed by atrophy(Figure 2). Although Resnick and Niwayama stated thatthe cause of the two entities was unknown, other scientific studies suggest that spondylosis deformans is theconsequence of normal aging, whereas intervertebral osteochondrosis, sometimes also called “deteriorateddisc,” results from a clearly pathologic, although notnecessarily symptomatic, process.32,36,37,40,41With normal aging, fibrous tissue replaces nuclearmucoid matrix, but the disc height is preserved and thedisc margins remain regular.22 Radial tears of the anulusare found only in a minority of postmortem examinations of individuals over 40 years of age,23 so cannot beconsidered a usual consequence of aging. Slight symmetric bulging of the disc may occur in the elderly remodeling associated with osteoporosis.41 On conventional radiographs and computed tomography (CT), smallamounts of gas can be detected in some elderly individuals at the anular/apophyseal enthesis, probably locatedin small transverse anular tears, and possibly signifyingearly manifestations of spondylosis deformans49; however, a large amount of gas in the central disc space isalways pathologic and is a feature of intervertebral osteochondrosis.35 Anterior and lateral marginal vertebralbody osteophytes have been found in 100% of skeletonsof individuals over 40, so are consequences of normalaging, whereas posterior osteophytes have been found inonly a minority of skeletons of individuals over 80, so arenot inevitable consequences of aging.32 Endplate erosions with osteosclerosis and chronic reactive bone marrow changes also appear to be pathologic. Slight to mod-erate decrease in central disc signal intensity found onT2-weighted MRIs can be a nonpathologic age-relatedobservation but, if the result of a normal process, shouldbe relatively uniform among all discs studied in the individual. Intervertebral osteochondrosis, or deteriorateddisc, also sometimes called “chronic discopathy,” shows,on microscopic examination, total structural disorganization and general replacement of normal disc tissue byfibrosis. Radiographically, intervertebral osteochondrosis is characterized by narrowing of the intervertebralspace, irregular disc contour often associated with bulging, multidirectional osteophytes often involving the central spinal canal and foramina, endplate erosions withreactive osteosclerosis, and chronic vertebral body bonemarrow changes. On T2-weighted images, the centraldisc signal intensity is usually markedly decreased, and atdistinct variance, to that seen in unaffected discs of thesame individual. The distinction is made at the time ofthe reading and does not imply that early manifestationsof a pathologic process are always distinguishable fromchanges of normal aging.Herniated DiscThe needs of common practice make necessary a diagnostic term that covers the various permutations of discmaterial displaced beyond the intervertebral disc space.Herniated disc, herniated nucleus pulposus, ruptureddisc, prolapsed disc (used nonspecifically), protrudeddisc (used nonspecifically), and bulging disc (used nonspecifically) have all been used in the literature in variousways to denote imprecisely defined displacement of discmaterial beyond the interspace. The absence of clear understanding of the meaning of these terms and lack ofdefinition of limits that should be placed on an idealgeneral term have created a great deal of confusion inclinical practice and in attempts to make meaningfulcomparisons of research studies.For the general diagnosis of displacement of disc material, the single term that is most commonly used andcreates least confusion is “herniated disc.” Attempts toavoid whatever confusion has been created by lack ofdefinition of the term “herniated disc” have included therecommendation to substitute the term “disc materialbeyond the interspace” (DEBIT),4 but that is more awkward and runs counter to common practice. “Herniatednucleus pulposus” (HNP) is inaccurate because materialsother than nucleus (cartilage, fragmented apophysealbone, fragmented anulus) are common components ofdisplaced disc material.6,47,48 “Rupture” casts an imageof tearing apart and therefore carries more implication oftraumatic etiology than “herniation,” which conveys animage of displacement rather than disruption.Though “protrusion” has been used by some authorsin a nonspecific general sense to signify any displacement, the term has a more commonly use
(Figure 10). Protrusion is present if the greatest distance, in any plane, between the edges of the disc material be-yond the disc space is less than the distance between the edges of the base, in the same plane. The base is defined as the cross-sectional area of disc material at the outer margin of the disc space of origin, where disc material