Transcription
Stroke and Brain InjuryWhitney GinesPEP 4370
Overview DefinitionEpidemiologyClinical AspectsTreatmentEffects of ExerciseExercise TestingExercise PrescriptionSummaryReferences
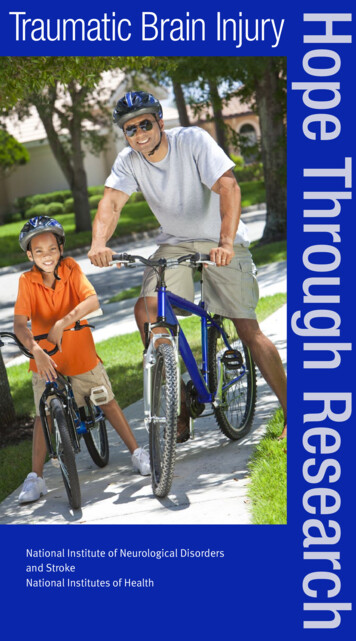
What is a Stroke? A stroke is the rapidly developing loss of brainfunction due to disturbances in the blood supplyto the brain Aka “cerebrovascular accident or brain attack” The majority of strokes (87%) are ischemic, resulting fromthrombosis or embolism. 10% of strokes are due to a hemorrhage or rupture of a vesselin the brain which leads to leaking of blood into the braintissue and cerebrospinal fluid.
Hemorrhagic vs. Ischemic stroke
What is a Brain Injury? Aka “Traumatic Brain Injury” (TBI) Results from a blow or jolt to the head from apenetrating head injury, or from being violentlyshaken. TBI causes permanent damage to the brain,resulting in total or partial functional disabilityor psychosocial impairment, or both.
Epidemiology for Strokeo 3rd leading cause of death in America and number one cause of adult disabilityo About 137,000 Americans die of stroke every yearo Every year 795,000 people in the US have a stroke. 610,000 are first time ornew strokes. 185,000 people who survive a stroke will have another one.o Someone in the US has a stroke every 40 seconds. Every 3-4 minutes someonedies of a strokeo Males are 1.5 times more likely to have a stroke than females until the age of74, when the incidence rate equalizeso 25% of stroke victims die as a result of the event itself or its complications,and roughly 50% will have moderate to severe health impairments and longterm disabilitieso The country’s highest death rates due to stroke are in the southeastern UnitedStates.
Epidemiology for Brain Injury 1.4 million new cases of TBI occur each year in the US; 50,000 of thesepeople die and 85,000 have long-term disability TBI is a contributing factor to a third of all injury-related deaths in the US The typical ages of onset for a TBI are between 0 and 4 years, between 15 and19 years, and then later in life (75 years ) Males aged 0 to 4 years have the highestrates of TBI-related emergency departmentvisits, hospitalizations, and deaths Falls and motor vehicle accidents arethe most common causes Direct medical costs and indirect costs suchas loss productivity of TBI totaled an estimated 60 billion in the US in 2003
ComplicationsStroke Paralysis or problemscontrolling movement Sensory disturbances Problems using orunderstanding language Emotional disturbancesBrain InjuryImpairments in one or more ofthe following: hinking Judgment Problemsolving Sensory Perceptual Motorabilities Psychosocial behavior Physicalfunctions Informationprocessing Speech
Treatment (Stroke) Medical treatments for stroke survivors includesthe following; Short-term use of anticoagulants and long-termuse of platelet inhibiting agents (heparin,coumadin, and aspirin) Vasodilators if vasospasm of the cerebral arteriesis suspected (hydralazine, clonidine, or isordil) Antihypertensive medications after hemorrhagicstroke requiring strict control of blood pressure
Treatment (Brain Injury) Some people with a brain injury may require moreintensive postacute medical management. Seizures and spasticity may necessitate long-termanticonvulsant and antispasmodic medications Some inidividuals receive medical therapy for thetreatment of depression or anxiety after TBI whichcan cause dizziness, hypotension, and alteredarousal states Some drugs may be used to combat cognitive defectsin people with TBI or stroke (tacrine, sinemet,ritalin, etc)
Treatment Physiological responses to medications Vasodilators may increase the cool-down periodrequired after exercise to prevent post-exercisehypotension Medications that limit cardiac output by reducingheart rate may cause lower peak heart rates Diuretics reduce fluid volume and alter electrolytebalance, causing dysrhythmias
How can I Prevent a Stroke? Eat a healthy dietMaintain a healthy weightBe active!!!Don’t’ smokeLimit alcohol use
Effects on the Ability of Exercise Overall functional capacity is typically low inindividuals who have recently sustained a TBI orstroke Functional implications for stroke and TBIsurvivors; Breathe harder with exertion Fatigue 2.5 times more rapidly Less efficient in mobility skills and activities ofdaily living**Thus, they are more likely to adopt a sedentary lifestyle withincreased risk of negative secondary conditions
Effects of Exercise TrainingExercise alone can reducemortality by 20% or more. General Benefits 60% greater VO2peakImproved oxygen consumptionWorkload responseBlood pressureResting heart rateCholesterol levelsIncreased walking speedDecreases ambulation (walking)assistance Functional mobility
Effects of Training Specific exercise programs may have limitedbenefits. The American Heart Association (AHA)recommends stretching, flexibility, balance, andcoordination exercises 2-3 times per week Muscle weakness frequently results from stroke,so the AHA recommends strength training withlight resistance 2-3 days per week.
TBI and Exercise Training Although most individuals with TBI are young, theirphysical capacities and endurance may be severelylimited by multisystem trauma. Exercise benefits specifically for TBIs include; Improved VO2peak Improved endurance Muscle strength These benefits result in greater independence, moreefficient locomotion, and greater employability
Exercise Testing“Exercise is a normal human function that can be undertaken with ahigh level of safety by most people, including stroke survivors.However, exercise is not without risks, and the recommendationsthat stroke survivors participate in an exercise program is basedon the premise that the benefits outweigh the risks. Therefore, theforemost priority in formulating the exercise prescription is tominimize the potential adverse effects of exercise via appropriatescreening, program design, monitoring, and patient education.”
Exercise Testing Biggest challenge in exercise testing is eachclient’s abilities and severity of complications isdifferent from person to person. Many stroke victims currently have or are at riskfor cardiovascular disease, therefore their testsshould be supervised by physician andmonitored with a 12-lead ECG. The mode of exercise testing depends on theseverity of physical impairments.
Modes of Exercise Testing Leg cycle ergometryTreadmillCombined arm-leg ergometrySteppersComputerized dynamometer: muscle strengthFlexibility testsNeuromuscular tests: Berg Balance Scale, gaitanalysis, NIH Stroke Survivor Scale, Postural Sway** Exercise equipment usually must be adapted to accommodateclient’s motor impairments.
Special Considerations forExercise Testing Large percentage of clients on hypertensionmedication (vasodilators) Seizure-prone clients on anticonvulsantmedications Arthritis in common in clients reduced ROM Reduced motor control of limbs Sensation may be impaired
Exercise Prescription The AHA recommends endurance trainingprograms for individuals with brain lesions,citing documented physiological, psychologicaland functional benefits Experts suggest a three tier program First phase: goal of exercise is to return tofunction Second phase: goal is to decrease risk of additionalstrokes Third phase: goal is to improve aerobic fitness
Exercise me togoalAerobic-increase independence40-70% of VO2peak3-5 days/week20-60 min/session (or multiple10 min sessions)2-4 months-increase independenceof ADLs3 sets of 8-12 reps1-2 exercises2 days/week2-4 months-increase ROM of2 days/week (before or afteraerobic or strength activities)2-4 months2 days/week2-4 monthsUpper and lower bodyCycle ergometerTreadmillArm ergometerSeated stepperStrengthIsometric exerciseWeight machineFree weightsFlexibilityof ADLs-Increase walking speed-Decrease risk of CVDinvolved extremitiesNeuromuscularCoordination andbalance activitiesImprove levels of safetyduring ADLs
Exercise Environment Consider behavioral factors when selecting themost appropriate environment for exercise ImpulsivityAggressionLack of judgmentMisunderstanding of directions
Final Considerations Depression and apathy are common following astroke or TBI and might interfere with long-termadherence to an exercise program. Cognitive deficits may interfere with ability tofollow directions in testing and training Inflexibility and imbalance can hinder exerciseand functional mobility Seizures are common and pose safety concernsduring exercise
Summary Recurrent stroke and cardiovascular disease arethe leading causes of mortality in strokesurvivors The main goal of exercise with stroke and braininjury patients is to increase independence inactivities of daily living and reduce risk forrecurrent stroke Each client’s abilities and complications requirehighly individualized exercise testing andprescription
9/16/2031/TBL2Ehrman, J., Gordon, P., Visich, P., & Keteyian, S. (2009).Clinical Exercise Physiology.United States of America: Human Kinetics.Freivogel, Susanna, Mehrholz, Jan, Husak-Sotomayor, Tanya, & Schmalohr, Dieter.(2008). Gait Training for non-ambulatory patients after stroke, spinal cord andbrain injury. Brain Injury. Vol 22 Issue 7/8http://doctor2008.wordpress.com/2010Williams, Jane, Perry, Lin, & Watkins, Caroline. (2010). Acute Stroke Nursing. WileyBlackwell Publishingwww.cdc.gov/stroke/about.htm
What is a Brain Injury? Aka "Traumatic Brain Injury" (TBI) Results from a blow or jolt to the head from a penetrating head injury, or from being violently shaken. TBI causes permanent damage to the brain, resulting in total or partial functional disability or psychosocial impairment, or both.