Transcription
Stroke:Challenges, Progress,and PromiseFebruary 2009National Institute ofNeurological Disordersand StrokeNational Institutes of Health
ContentsIntroduction 11IntroductionStroke Basics 3Ischemic Stroke and Transient Ischemic Attack 3Hemorrhagic Stroke 5Vascular Cognitive Impairment 62Stroke Diagnostics and Brain Imaging 73Stroke Risk Factors 94Unmodifiable Risk Factors 9that nearly everyone.Modifiable Risk Factors 10.reading this has already had an unwelcomeintroduction to stroke, perhaps throughfirsthand experience or by witnessing its effectson a relative. Research sponsored by the NationalInstitutes of Health (NIH) shows that about onein six Americans will experience a stroke at somepoint after age 65. Stroke is fatal in about 10 to20 percent of cases and, among survivors, it cancause a host of disabilities, including loss of mobility,impaired speech, and cognitive problems. Thesetrends have made stroke the third leading causeof death in the U.S. (behind heart disease andcancer) and a major cause of disability.Current Stroke Treatment and Prevention 14Medications 14Surgeries and Other Procedures 17Rehabilitation 195Chances areResearch and Hope for the Future 20Prevention 20Acute Stroke and Post-Stroke Therapy 23Neuroprotection 256A stroke is a sudden event affecting the brain’sblood supply. In an ischemic stroke, a bloodvessel that supplies the brain becomes blocked.In a hemorrhagic stroke, a blood vessel in thebrain bursts. Although stroke is most common inolder people, it can occur in individuals of any age,including young adults, children, infants, andfetuses in the womb.Fortunately, the prospects for preventing andtreating stroke are far better than they were justa few decades ago, thanks in part to researchsupported by the NIH’s National Institute ofNeurological Disorders and Stroke (NINDS).NINDS-funded investigators have identified many riskfactors for stroke, such as hypertension (high bloodpressure), arming people with the ability to reducetheir risk through lifestyle changes or medication.Clinical trials supported by NINDS also led tothe only drug approved by the Food and DrugAdministration specifically for treating acuteischemic stroke—the “clot-buster” tPA. When givenwithin three hours of stroke onset, the drug significantlyreduces the likelihood of long-term disability.Current NINDS priorities in stroke research are setby its Stroke Progress Review Group (SPRG),an advisory body made up of scientists, clinicians,patient advocates, and industry representatives.One such priority is to develop new and moreeffective treatments for acute stroke. NINDS issupporting research on novel ways to restoreblood flow to the ischemic brain, as well astreatments that would act directly on brain cells toprotect them from the effects of stroke.Another priority is to improve post-stroke recoveryby tapping into the brain’s capacity to repairitself; for example, by using drugs to stimulatethe growth of new brain cells or physical therapyregimens to stimulate the re-wiring of existing cells.Finally, stroke prevention and the identification ofstroke risk factors remain important parts of theNINDS portfolio.Changing Stroke’s Impact by Changing Attitudes 32Stroke: Challenges, Progress, and Promise1
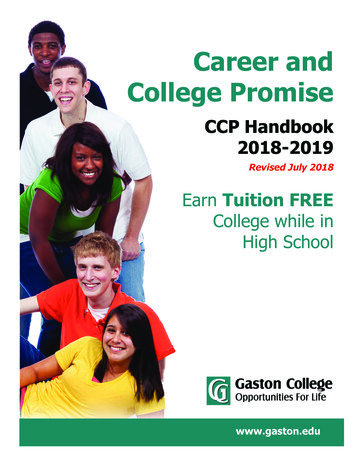
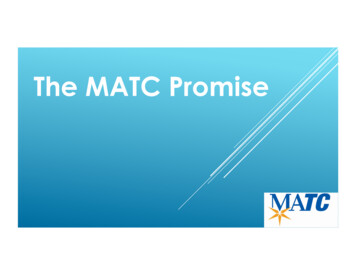
1. StrokebasicsAn ischemic stroke occurs when a blood ve selsupplying the brain becomes blocked, as by a clot.NINDS supports several complementarynetworks of research centers aimed atimproving treatment and care for individualswith acute stroke. The Specialized Programof Translational Research in Acute Stroke(SPOTRIAS) helps move experimental therapiesfor acute stroke from the lab into early-phaseclinical studies. SPOTRIAS sites are locatedat major academic medical centers acrossthe country, where scientists studying themolecular and cellular mechanisms of strokecan work closely with clinicians who haveexpertise in acute stroke care. The NeurologicalEmergencies Treatment Trials (NETT) networkcreates a similar collaborative framework amongneurologists, neurosurgeons, and emergencymedicine physicians to facilitate clinical trialson stroke in the emergency room. Meanwhile,through the Stroke Preclinical Trials Consortia,NINDS is forging collaboration amonginvestigators who are testing potential stroke2Stroke: Challenges, Progress, and PromiseA hemorrhagic stroke occurs when a blood vesselbursts, leaking blood into the brain.treatments in animal models. Finally, NINDSoutreach programs help bridge research andpractice by educating individuals, their lovedones, and healthcare providers about the latestadvances in treatment and prevention.TnnnNINDS is supportingresearch on novel ways torestore blood flow to theischemic brain, as well astreatments that would act directlyon brain cells to protect themfrom the effects of stroke.nnhe effects of stroke manifest themselves rapidly.The five most common symptoms of stroke are:Sudden weakness or numbness of the face orlimbs, especially on one side of the body.Sudden confusion or difficulty speaking orunderstanding speech.Sudden trouble seeing in one or both eyes.Sudden trouble walking, dizziness, or loss ofbalance or coordination.Sudden severe headache with no known cause.The exact symptoms depend on where in thebrain’s vascular system the blockage or rupturehas occurred. Strokes that predominantly affectone hemisphere of the brain are common. Sinceeach hemisphere controls the opposite side ofthe body, a stroke in the left hemisphere willcause motor and sensory deficits on the right sideof the body, and vice versa.The long-term outcomes after a stroke varyconsiderably and depend partly on the typeof stroke and the age of the affected person.Although most stroke survivors regain theirfunctional independence, 15 to 30 percent willhave a permanent physical disability. Some willexperience a permanent decline in cognitivefunction known as post-stroke or vascular dementia.Unfortunately, many stroke survivors face adanger of recurrent stroke in the future. About20 percent of people who experience a first-everstroke between ages 40 and 69 will have anotherstroke within five years. Finding treatments tohelp prevent stroke in this high-risk group is amajor focus of NINDS-supported research.Ischemic Stroke andTransient Ischemic AttackIschemic strokes make up about 80 percentof all strokes. Just as a heart attack occurswhen there is insufficient blood flow to theheart, an ischemic stroke (sometimes calleda “brain attack”) occurs when there is a suddeninterruption in blood flow to one or moreregions of the brain. Like all cells in the body,neurons and other brain cells require oxygenand glucose delivered through the blood inorder to function and survive. A few minutes ofoxygen deprivation—called ischemia—is enoughto kill millions of neurons. Moreover, ischemiacan provoke inflammation, swelling (edema),and other processes that can continue to causedamage for hours to days after the initial insult.Obstructive blood clots are the most commoncause of ischemic stroke. Clotting (or coagulation)is a vital function that helps prevent bleedingwhen a blood vessel is damaged, but clots canalso obstruct normal blood flow. When a clotforms in association with the wall of a bloodStroke: Challenges, Progress, and Promise3
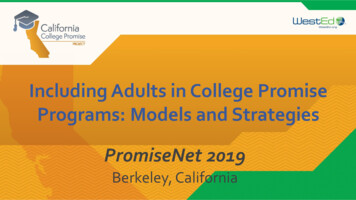
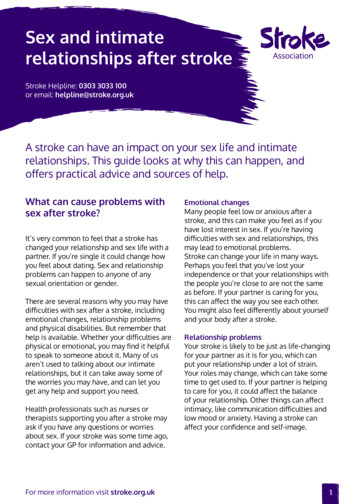
Cerebral AmyloidAngiopathyMedical Terms for CommonStroke Symptoms and DisabilitiesHemiplegia: paralysis on one side of the body.Hemiparesis: weakness on one side of the body.Hemineglect: lack of awareness of one side ofImmediately after an ischemic stroke, the brainusually contains an irreversibly damaged coreof tissue and an area of viable but at-risk tissuecalled the ischemic penumbra. Restoringnormal blood flow—a process known asreperfusion—is essential to rescuing thepenumbra. The longer reperfusion is delayed,the more cells in the penumbra will die. Theregion of brain tissue that is finally damaged iscalled an infarct.the body or one side of the visual field.Dysphagia: difficulty swallowing.Dysarthria: difficulty talking, caused byfacial weakness.Aphasia: difficulty speaking or understanding speech,caused by damage to the brain’s language centers.vessel and grows large enough to impair bloodflow, it is called a thrombus; a clot that breaksoff the vessel wall and travels through the bloodis an embolus. A cardioembolic stroke iscaused by a clot that originates in the heart.Cardiac emboli are most likely to form in peoplewith heart conditions such as atrial fibrillation(AF, an irregular heartbeat), heart failure, stenosis,or infections within the valves of the heart.They may also occur post-heart attack.Another contributor to ischemic stroke is chronicatherosclerosis, which is a buildup of fatty depositsand cellular debris (plaque) on the inside of theblood vessel wall. As atherosclerotic plaquesgrow, they cause narrowing of the blood vessel(a condition called stenosis). Atherosclerosis can alsoactivate cells involved in clotting.4Curing Epilepsy: The Promise of ResearchIf a stroke were a storm, a transient ischemicattack (TIA), or “mini-stroke,” would be anominous thunderclap. Symptoms of a TIAare similar to those of a full-blown stroke butresolve within 24 hours, typically in less than onehour. Still, the short-lived nature of TIAs doesnot mean that they leave the brain unharmed.In about 40 to 50 percent of people who haveexperienced a TIA, a tiny dot of infarct can beseen by brain imaging.Even when there is no sign of brain infarction,a TIA is both a warning and an opportunityfor intervention. While someone who hasexperienced a full-blown stroke has a two toseven percent risk of having another strokewithin the next 90 days; the 90-day risk of strokefollowing a TIA is 10 to 20 percent. In manycases, TIAs may be caused by an unstable clotthat could create a more permanent blockagewithin the brain’s blood supply at any moment.Fortunately, there are a variety of treatmentsthat can reduce the risk of stroke followinga TIA, including medications to lower bloodpressure and inhibit blood clotting. If necessary,surgical procedures can clear away plaque in thearteries that supply the brain, or a procedurecalled stenting can be used to widen the arteries.Severe strokes could be avoided if more peoplesought medical attention after a TIA. (For moreabout these treatments, see the chart on p. 10and “Current Stroke Treatment and Prevention”on p. 14.)Cerebral amyloid angiopathy (CAA) refers to aHemorrhagic Strokecontributing factor to intracerebral hemorrhageAn intracerebral hemorrhage occurs whena blood vessel ruptures within the brain.Several conditions can render blood vesselsin the brain prone to rupture and bleeding.Chronic hypertension and a condition knownas cerebral amyloid angiopathy can weaken theblood vessel wall. Poor blood clotting abilitydue to blood disorders or blood-thinningmedications like warfarin further increasethe risk of bleeding. Finally, structuralabnormalities that can form in blood vesselsduring brain development also a play a role.For instance, an arteriovenous malformation(AVM) is a tangled mass of thin-walled cerebralblood vessels in the brain. AVMs are thought tobe present from birth in one percent or less ofthe population.small ischemic infarctions and vascular cognitiveaneurysmbuildup of protein deposits known as amyloidon the inside wall of blood vessels. It is a majorin older people and is sometimes associated withimpairment.CAA is regarded as a disease of aging. It is rarelyobserved in individuals under age 50, but isseen in about 50 percent of individuals over age90. The proportion of intracerebral hemorrhagecases in older people that are causally linked toCAA is unclear, but recent estimates place thatnumber as high as 50 percent.The buildup of amyloid inside blood vesselsweakens the vessel wall and may lead toblood vessel rupture. In recent years, apoorly understood connection has emergedbetween CAA and Alzheimer’s disease.Beta-amyloid—the toxic protein fragment thataccumulates in clumps (called plaques) withinthe brain tissue of people with Alzheimer’sdisease—is a component of the amyloiddeposits found in people with CAA. Moreover,Alzheimer’s disease and CAA share similargenetic risk factors, such as the gene encodingapolipoprotein E (APOE). A variant of thisgene known as e4 increases the risk ofAlzheimer’s disease and the risk of recurrentarteriovenousmalformationintracerebral hemorrhage.An aneurysm is a bulge in a blood vessel and anarteriovenous malformation is a tangled massof thin-walled vessels. Both of these structuresare associated with a risk of hemorrhagic stroke.Stroke:Curing Epilepsy:Challenges,TheProgress,Promiseandof ResearchPromise5
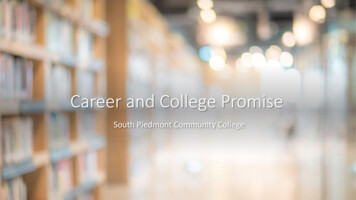
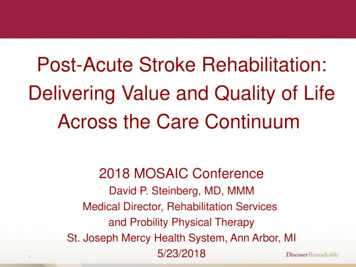
A subarachnoid hemorrhage is the rupture ofa blood vessel located within the subarachnoidspace—a fluid-filled space between layers ofconnective tissue (meninges) that surroundthe brain. The first sign of a subarachnoidhemorrhage is typically a severe headachewith a split-second onset and no known cause.Neurologists call this a thunderclap headacheand it demands immediate medical attention.The rupture may occur in an AVM, but typicallyit occurs at a site where a blood vessel hasweakened and bulged, called an aneurysm.Aneurysms affect as much as one percent ofthe population, and are sometimes hereditary.NINDS-funded studies have shown that the riskthat an aneurysm will rupture is related to itssize and shape, its location, and the person’s age.The risk is increased by smoking. Information aboutthese risks helps doctors advise individuals on whetheran asymptomatic aneurysm should be treated.Immediately after an ischemic stroke (top left), a coreof irreversibly damaged brain tissue (red) is surroundedby an area of viable but at-risk tissue called thepenumbra (green). Unless blood flow is restored quickly,the tissue within the penumbra will be lost (bottom right).6Stroke: Challenges, Progress, and PromiseUnlike other tissues in the body, neural tissuenormally is shielded from direct contactwith blood by the blood-brain barrier, whichis a tightly sealed network of cellular andextracellular components that lines bloodvessels in the brain. The blood-brain barrieris permeable to oxygen and other nutrients inthe blood, but generally impermeable to redand white blood cells, and large molecules.During a hemorrhagic stroke, these cells andmolecules are released en masse into thedelicate environment that surrounds neurons.Meanwhile, the accumulation of blood, knownas a hematoma, can cause an increase inintracranial pressure that further impairsnormal blood flow and damages the brainby compression.Vascular CognitiveImpairmentEven in the absence of a clinically obvious strokeor TIA, impaired blood flow in the brain mayeventually lead to vascular cognitive impairment(VCI). At one extreme, VCI includes vasculardementia, but it also refers to a gradual declinein mental function caused by multiple strokes,some silent, over time. It is often associatedwith a more diffuse small vessel disease, causedby narrowing of small-diameter blood vesselsthat supply limited territories within the brain.Clinically, VCI may resemble Alzheimer’sdisease (AD) and many older individuals withdementia meet the diagnostic criteria for bothdiseases. However, while AD primarily affectsmemory, VCI appears to primarily affect thebrain’s executive function—the ability to planactivities from getting dressed in the morning tonegotiating a business deal.2. StrokeDiagnosticsand brainImagingWhen a stroke is suspected, a physicianwill carry out a detailed assessment of theindividual’s signs and symptoms. One commonassessment tool is the NIH Stroke Scale,developed by NINDS. This is a checklist ofquestions and tasks that scores an individual’slevel of alertness and ability to communicate andperform simple movements. Other commondiagnostic procedures include blood tests and anelectrocardiogram to check for cardiac abnormalitiesthat might have contributed to the stroke.Brain imaging techniques play an importantrole in stroke diagnosis, in the evaluation ofindividuals with stroke for clinical trials, and,to a growing extent, assessment of stroke risk.Several imaging techniques can be used togenerate visual “slices” of the brain or eventhree-dimensional reconstructions. This in-depthlook at the brain helps to: rule out other potentialneurological conditions such as a brain tumor,differentiate ischemic from hemorrhagic stroke,identify which blood vessels have been damaged,and determine the extent and location of the infarct.Computed tomography (CT) and magneticresonance imaging (MRI) are the two mostcommon imaging techniques used to identifyinfarctions caused by stroke. CT uses X-raybeams passed through the head at multiple anglesto generate high-resolution brain images. It isfaster, more widely available, and less expensivethan MRI.MRI, which does not involve X-rays, exposes thebrain to a magnetic field in combination with aradio wave pulse. The brain’s absorption of thispulse and the rate at which energy is releasedwhen the pulse ends varies in different braintissues and yields an image. Diffusion-weightedimaging (DWI) is a highly sensitive type of MRIthat measures the diffusion of water in braintissue, which changes during an ischemic stroke.DWI is especially useful for detecting smallinfarcts and is superior to CT for diagnosingischemic stroke. Research studies suggest thatDWI in combination with a brain blood perfusionstudy can be used to help identify the ischemicpenumbra—brain tissue that is blood-starved, butsalvageable if blood flow can be restored quickly.In many individuals, the extent of ischemicpenumbra is related to the degree of diffusionperfusion mismatch, which is a DWI signal thatoccurs in brain tissue with normal water diffusionbut abnormal blood flow.Several imaging techniques are used to examinecerebral blood vessels. These techniques canreveal the site of blockage in an ischemic strokeor detect stenosis or vascular malformations (suchas an aneurysm or AVM) that put a person at riskfor stroke. Angiography of the brain involvesStroke: Challenges, Progress, and Promise7
Unmodifiable Risk Factors3. Stroke riskFactorsThe risk of stroke varies by age, sex, race, andeven where we live. Although these risk factorsare considered unmodifiable, they help informstroke prevention strategies at the individual andpopulation levels.Stroke and AgeMRI scans are commonly used to check for damage to the brain and the brain’s vasculature in people suspected of having a stroke.Brain imagingtechniques play an importantrole in stroke diagnosis.andto a growing extent, in theassessment of stroke risk. Severalimaging techniques can be usedto generate visual “slices” of thebrain or even three-dimensionalreconstructions.8Stroke: Challenges, Progress, and Promiseimaging after a contrast agent that shows up darkon a scan has been injected into a vein in the armor leg, which yields a map of the brain’s blood vessels.A procedurally similar technique called perfusionimaging is sensitive for detecting abnormalblood flow in the brain. Doppler ultrasoundinvolves passing high-frequency, inaudible soundwaves into the neck or head. These sound wavesbounce off of cells moving through the blood,producing an image and providing informationon how fast the blood is traveling. In general,blood cells speed up as they move through anarrow vessel.Given that stroke is caused by blockage orrupture of a blood vessel, it should be nosurprise that similar modifiable risk factorscontribute to stroke and cardiovascular disease,including hypertension, smoking, diabetes,high cholesterol, and lack of physical activity. Itis possible to dramatically reduce these risksthrough healthier lifestyle choices or medications(such as blood pressure-lowering drugs). In fact,since 1950, there has been about a 60 percentdecline in the mortality rate from stroke and asmaller but significant decline in the age-adjustedannual incidence of stroke—the number ofpeople who have a stroke each year, adjusted toaccount for the increasing age of the population.Many experts attribute these trends to increasingawareness and control of stroke risk factors.(For quick facts about the most potent modifiablestroke risk factors and ways to counteract them,see “Modifiable Risk Factors ” on p. 10.)The effects of age on the cardiovascular system,combined with the insidious nature of othertypes of risk over the life span, make it a key riskfactor for stroke. A major source of informationabout stroke risk is the Framingham HeartStudy, which began tracking the cardiovascularhealth of some 5,000 individuals from theFramingham, Massachusetts area in 1948 andhas since expanded to include their children.The study, which receives primary support fromNIH’s National Heart, Lung, and Blood Institute(NHLBI) and support for its stroke componentfrom NINDS, has shown that the risk of strokedoubles for each decade between the agesof 55 and 85.Stroke in young adults is relatively infrequent,but it does happen. The Northern ManhattanStudy, supported by NINDS, found that, amongpeople living in that area in the mid-1990s, theannual incidence of stroke was about two per10,000 among people age 20 to 44, and about56 per 10,000 among people ages 45 and older.This study and others in the U.S. have found thathemorrhagic and ischemic strokes tend to occurin roughly equal proportion in young people.The increased risk of stroke that occurs with agetherefore appears to be mostly an increased riskof ischemic stroke. (Also see “Stroke in Infantsand Children” on p. 11.)Stroke: Challenges, Progress, and Promise9
Modifiable Risk FactorsRisk factorHow much it affects stroke riskWhy it affects stroke riskHypertensionHypertension causes a two- tofour-fold increase in the risk ofstroke before age 80. after age80, the impact of hypertensiondeclines and other risk factorsbecome more important.Hypertension promotesblood pressure medications,atherosclerosis and causes mechanical such as thiazide diuretics anddamage to the walls of blood vessels. angiotensin-converting enzyme(aCe) inhibitors, can reduce therisk of stroke by 30 to 40 percent.early treatment is essential.among older people withnormal blood pressure, priormid-life hypertension increasesstroke risk up to 92 percent.Guidelines from the Centers forDisease Control and Preventionrecommend a target blood pressureof less than 140/90 mm Hg.Cigarette smokingSmoking causes about a two-foldincrease in the risk of ischemicstroke and up to a four-fold increasein the risk of hemorrhagic stroke.Smoking promotes atherosclerosisand aneurysm formation, andstimulates blood clotting factors.Stroke risk decreases significantlytwo years after quitting smokingand is at the level of nonsmokersby five years.DiabetesIn terms of stroke and cardiovasculardisease risk, having diabetes is theequivalent of aging 15 years.In diabetes, glucose is notefficiently taken up by the body’scells and accumulates in the bloodinstead, where it can damage thevascular system. Hypertensionis common among diabeticsand accounts for much of theirincreased stroke risk.blood pressure medications,dietary changes, and weight losscan lower stroke risk. Controllingblood sugar appears to reduce therisk of recurrent stroke.Waist-to-hip ratio equal to orabove the median (mid-value forthe population) increases the riskof ischemic stroke three-fold.Obesity is associated withhypertension, diabetes,and heart disease.While no clinical studies havetested the effects of exercise orweight loss on stroke risk, bothtend to reduce hypertension andboost cardiovascular health.Physical inactivity andobesity10What you can doatrial fibrillation (aF)aF affects fewer than one percentof people under age 60, but ismore prevalent in older people.It is responsible for one in fourstrokes after age 80, and is associatedwith high mortality and disability.aF refers to irregular contraction ofthe atrium—the chamber whereblood enters the heart. aF canlead to blood stagnation andincreased clotting.Warfarin, a blood-thinningmedication, can reduce the risk ofstroke in people with aF. Peopleunder age 60 with aF and no otherstroke risk factors may benefit fromaspirin. Importantly, pacemakershave no effect on the risk of strokeassociated with aF.Cholesterol imbalanceHigh-density lipoprotein (HDL)cholesterol is generally consideredprotective against ischemic stroke.Low-density lipoprotein (LDL)cholesterol, when present in excess,is considered harmful.LDL and HDL are needed to carrycholesterol (a fatty substance)through the blood (made upmostly of water), and deliver itto cells. because LDL deliverscholesterol to cells throughoutthe body, excess LDL can causecholesterol to build up in bloodvessels, leading to atherosclerosis.HDL sends cholesterol to the liverto be eliminated.Clinical trials have shown thatcholesterol-lowering drugs knownas statins reduce the risk of stroke.However, some studies point toonly a weak association betweenstroke and cholesterol, and thereis speculation that statins reducestroke risk by acting through someunknown mechanism.Stroke: Challenges, Progress, and PromiseStroke in Infants and ChildrenCompared to stroke in the adult brain, strokein the young, growing brain is associated withunique symptoms, risk factors, and outcomes—and with more uncertainty in all three of theseareas. Although stroke is often considered adisease of aging, the risk of stroke in childhoodis actually highest during the perinatal period,which encompasses the last few months of fetallife and the first few weeks after birth.As in adults, the symptoms of stroke in infantsand children include headache, hemiplegia, andhemiparesis. But very young children with strokeare more likely than adults to experience othersymptoms, such as seizures, breathing problems,or loss of consciousness. Because the incidenceof childhood stroke is relatively low, parentsand doctors often mistakenly attribute thesesymptoms to other causes, leading to delays indiagnosis. Moreover, the time of onset is usuallyunknown for strokes during the perinatal period.Investigators know less about the risk ofchildhood stroke than they know about therisk of adult stroke. However, well-documentedrisk factors include congenital (inborn) heartabnormalities, head trauma, and bloodclotting disorders. An important risk factorfor African American children is sickle celldisease. Although sickle cell disease is knownfor its effect on red blood cells—causing themto take on a sickle shape—it can also cause anarrowing of cerebral arteries. A 1998 study ofsome 3,000 people with sickle cell disease foundthat 11 percent experienced a stroke before age20. Fortunately, that same year, a study fundedby NHLBI showed that repeated transfusions toreplace sickled blood cells with normal bloodcells reduced the risk of stroke by 92 percent.Yearly Doppler ultrasound imaging is recommendedfor young children with sickle cell disease and,if stenosis is found, repeated transfusions canbe used as a means of stroke prevention.Strokes during the perinatal period have beenassociated with premature birth, maternalinfections, maternal drug abuse, prior infertilitytreatments, and maternal health conditions suchas autoimmune disease and preeclampsia (apotentially serious combination of hypertensionand kidney problems that affects about sixpercent of pregnant women).The outcome of stroke in the very young isdifficult to predict. A stroke during fetaldevelopment may lead to cerebral palsy—apermanent problem with body movement andmuscle coordination that appears in infancy orearly childhood. A stroke that occurs duringinfancy or childhood can also cause permanentdisability. Generally, outcomes are worse inchildren under age one and in those whoexperience decreased consciousness or seizures.Fortunately, the developing brain is also knownfor its remarkable capacity to replace lost nervecells and fix damaged connections between them.Healthy areas of the brain are often still pliableenough to compensate for damaged areas.Stroke: Challenges, Progress, and Promise11
A child with serious deficits immediately after astroke can make an impressive recovery.Treatment of stroke in children presents uniquechallenges. Delays in diagnosis, which can beespecially prolonged in cases of perinatal stroke,mean that valuable time is lost. Moreover, mosttreatments for acute stroke were developedbased on studies in adults and the guidelines fortheir use in children are still being refined. Toaddress some of these issues, NINDS and NIH’sNational Institute of Child Health and HumanDevelopment (NICHD) sponsored a workshopon per
A stroke is a sudden event affecting the brain’s blood supply. In an ischemic stroke, a blood vessel that supplies the brain becomes blocked. In a hemorrhagic stroke, a blood vessel in the brain bursts. Although stroke is most common in . older people, it can occur in individuals o