Transcription
Santoro and Steffensen Journal of Congenital -7(2021) 5:1Journal ofCongenital CardiologyREVIEWOpen AccessCongenital heart disease in Downsyndrome – A review of temporal changesStephanie L. Santoro1,2*and Ellen Hollands Steffensen3,4AbstractBackground: Congenital heart disease (CHD) is a well-known co-occurring condition in Down syndrome (DS). Weaimed to review the literature to evaluate the current evidence to address key questions.Methods: A series of key questions were formulated a priori to inform the search strategy and review process.These addressed the topics of prevalence, type of CHD, severity, and screening. Using the National Library ofMedicine database, PubMed, detailed literature searches were performed. The quality of available evidence wasthen evaluated, the existing literature was summarized, and knowledge gaps were identified.Results: Fifty-six relevant original articles were identified which addressed at least one key question. Study details,including: research design, internal validity, external validity, and relevant results are presented. The total prevalenceof CHD reported in DS ranged from 20 to 57.9%. In later decades, the prevalence remained constant at 40—55%.The types and classification of CHD varied considerably between studies. Some studies indicate a trend towards amilder phenotype, but this was not consistent. Over time, some studies observed an improved prognosis for CHDin DS. Studies investigating screening for CHD by physical examination, chest X-ray, and electrocardiogram reportsensitivities of 71–95%.Conclusion: To further improve knowledge on CHD in DS, we suggest that future studies cover a wide range ofnations and regions, with a longitudinal design, and account for potential confounding factors.Keywords: Down syndrome, Trisomy 21, Cardiology, Cardiac, Congenital heart diseaseIntroductionDown syndrome (DS) is present in one in 800 infants bornin the United States, making it the most common chromosomal condition associated with a unique medical and developmental profile [1, 2]. Congenital heart disease (CHD) isone of the co-occurring medical diagnoses associated withDS [3, 4]. Among patients with DS, the presence of CHD isa known contributor to morbidity and mortality [5].Although the association of CHD with DS has beenknown for decades, much has changed over time interms of available diagnostics, medical care, andtreatments. We conducted this project to present an updated literature review on CHD in DS. The overarchinggoals of this review were to: 1) Formulate key questionsa priori and identify which original articles address thesekey questions. 2) Search PubMed to identify original research articles that address the cardiac phenotype ofindividuals with DS. 3) Assess these articles using UnitedStates Preventative Services Task Force (USPTF)methods [6]. 4) Summarize the published literature andidentify gaps in evidence.* Correspondence: ssantoro3@mgh.harvard.edu1Division of Medical Genetics and Metabolism, Massachusetts GeneralHospital, Boston, MA, USA2Department of Pediatrics, Harvard Medical School, Boston, MA, USAFull list of author information is available at the end of the articleMethodsKey questionsIn accordance with USPSTF practice we formulated aseries of key questions as outlined in a prior review [7]. The Author(s). 2021 Open Access This article is licensed under a Creative Commons Attribution 4.0 International License,which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you giveappropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate ifchanges were made. The images or other third party material in this article are included in the article's Creative Commonslicence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commonslicence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtainpermission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.The Creative Commons Public Domain Dedication waiver ) applies to thedata made available in this article, unless otherwise stated in a credit line to the data.
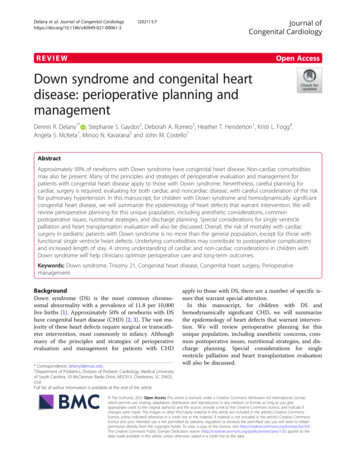
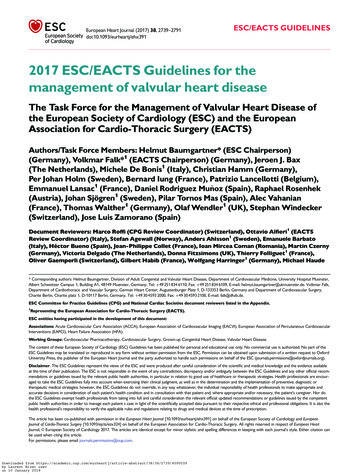
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1By consensus, the following key questions were formulated by the authors:1. What is the total prevalence of congenital heartdisease in DS? And, has the prevalence ofcongenital heart disease in DS changed over time?2. What is the type of congenital heart disease in DS?And, has the type of congenital heart disease in DSchanged over time?3. What is the severity of congenital heart disease inDS in terms of treatment and prognosis? And, hasthe severity of congenital heart disease in DSchanged over time?4. What screening for congenital heart disease in DSis performed in studies? And, has the screening forcongenital heart disease in DS changed in thepublished literature over time?Page 2 of 14of DS (e.g. surgical patients) which would not generalizeto answer our key questions.Using only the PubMed articles meeting inclusion, datapertaining to key questions were extracted from the abstract, methods, and results sections and entered into apreformatted Excel data template for analysis. For graphical representation of temporal changes, we grouped reported CHD’s according to [15]. to facilitate comparisonsacross studies [8]. See Fig. 1 for an overview of the identification, inclusion and exclusion process and Supplemental Table for details of extracted data.Factors which may impact these key questions such as:publication year, population details (number of subjectsstudied, age of sample, location, source of subjects anddemographics: gender, race, prenatal or postnatal diagnosis of CHD, prenatal or postnatal diagnosis of DS) ifprovided, and research methodology were recorded.PubMed literature searchEvidence ratings by conditionLiterature searches were conducted in August – September 2020 using the National Library of Medicine (NLM)biomedical literature database PubMed (MEDLINE)(NCBI 1946–2020) to identify original research manuscripts addressing our prioritized topics. We used theMedical Subject Headings (MeSH) (the NLM controlledvocabulary thesaurus for indexing) to capture relatedentry terminology in our searches. For example, theMeSH term “Down syndrome” included the search entryterms: Downs syndrome, Down’s syndrome, Mongolism,Trisomy 21, Partial Trisomy 21. The MeSH term “Downsyndrome” was combined using the Boolean operator‘AND’ with the MeSH term “congenital heart defect”which included the search entry terms of specific cardiacmalformations, to capture the unfiltered literature. Then,the limiters “Human”, “English” were applied to narrowthe scope of the search to filtered literature. We did notuse subject age as a limiter. We also did not exclude articles based on timing of study either prenatal or postnatal, and did not filter our search to only live births.Abstracts were reviewed and included according to theirrelevance to key questions. Whenever an abstract mademention of any key question (or there was doubt) thefull article was procured. The methods and results sections were then reviewed to determine which articlesmet inclusion or exclusion criteria. A single reviewerconducted the literature searches, reviewed articles forinclusion, and extracted data. Article inclusion criteriaincluded: data addresses at minimum one key questionand supporting data is original (not previously published). Exclusion criteria included: data does not address at least one key question, study uses anuninterpretable methodology, case series 5, does notprovide supporting data, did not present data specific toDS, focused on a single type of CHD, is a unique subsetIncluded articles were critically appraised by a single reviewer to determine each study’s research design, subjectascertainment, total number of subjects, source of control subjects, and the extent of internal validity and external validity. The evaluation of internal validityconsiders study design factors such as ascertainment andselection bias, test procedures and consideration of confounding variables. For example, the internal validity ofa cohort study is rated as good if it “Meets all criteria:comparable groups are assembled initially and maintained throughout the study (follow-up greater than orequal to 80%); reliable and valid measurement instruments are used and applied equally to all groups; interventions are spelled out clearly; all important outcomesare considered; and appropriate attention to confoundersin analysis. In addition, intention-to-treat analysis is usedfor RCTs” (USPSTF Procedure Manual (2015), p. 70[6]). External validity considers the generalizability offindings to a broader (more representative) population[6]. See appendix VII in the USPSTF report for criteriaon research design hierarchy and the rating system usedfor scoring internal and external validity [6]. See Fig. 1for summary of evidence rating, and the SupplementalTable for rating of each article.ResultsOriginal literature reviewThrough review of the literature, we identified 56 articleswhich fit our criteria of having original data, answering akey question about DS and types of CHD, in humans,and reported on more than 5 cases (Fig. 1, Table 1).These studies were published from 1950 to 2019, andused various study designs including: cohort studies[N 22], cross-sectional studies [24], case-control studies [10], and case-series [2]. The study methods
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1Page 3 of 14Fig. 1 PRISMA Diagram of Articles Identified, Screened, Eligible, and Included in Review of CHD Phenotype in Down Syndrome. Research designhierarchy in accordance with United States Preventative Services Task Force methodsincluded: retrospective review [24] registries and databases [26], prospective screening programs [5], and parent survey [3]. Nearly all studies reported on a cohort, ofwhich some were population-based samples [23] andsome reported data longitudinally [5]. Some studiescompared those with DS and CHD to those with DSwithout CHD. In addition to the bracketed number ofstudies, please see the Supplemental Table for specificdetails on each of the 56 studies.Data extracted from original literature review whichaddressed one of our four key questions are presentedbelow. We report studies based in the United Statesfollowed by international results.1. What is the total prevalence of congenital heartdisease in DS? And, has the prevalence ofcongenital heart disease in DS changed over time?Eighteen articles answered this key question from a varietyof locationsIn the United States, in national discharge data of 11,372DS births, approximately 36% recorded selected cardiacmalformations in 2007 [9]. Publications from thepopulation-based National DS Project reported prevalence of CHD in infants with DS; in 2008, 649 of 1469(44.2%), and in 2011, 483 of 1079 (44.8%) [10, 11]. Prior,data from the population-based registry, the CaliforniaBirth Defects Monitoring Program, reported CHD in385 of 687 (56%) infants with DS in one publication[12], and in another 1620 of 2894 (56%) infants with DShad a cardiovascular system birth defect [13].Publications from the population-based MetropolitanAtlanta Congenital Defects Program (MACDP) found227 DS cases, of which 44% had CHD in 1989 to 1995[14], and in 1968 to 1989 saw that 173 of 552 DS cases(33%) had cardiovascular malformations [15]. Over time,the frequency of these defects increased dramaticallyfrom about 20% in the early 1970s to more than 50% inthe late 1980s (p 0.0001), which the authors attributedto improvement in the ascertainment of cardiovascularmalformations among infants with DS in a surveillancepopulation [15].To describe prevalence in CHD over time, eight additional international studies provided longitudinal data.In Sweden, among 2588 singleton live-born infants withDS between 1992 and 2012, 1387 infants had a diagnosed congenital heart defect, giving an overall birthprevalence of 54% which was similar over time [8]. In amulti-site European study of 14,109 cases with DS, ofwhom 6738 were live births, 306 fetal deaths, and 7065terminations of pregnancy for fetal anomaly in 2000–2010, the overall prevalence of cardiac anomaly was43.6% (95% confidence interval (CI): 42.4–44.7%) andhad remained nearly constant [16]. A study of birth defects registries in France, Italy and Sweden in 1978–1993, found that cardiac defects were registered in 26%of the 5581 infants with DS [17]. In a Norwegian studyno apparent increasing or decreasing trend in the prevalence of CHD in live born infants with DS was observedduring 1994–2009 [18]. No significant change in prevalence was seen in Thailand with 64 of 149 with DS bornin 2009–2013 who had CHD (43%) compared with 112in 295 (38.6%) DS patients born in 1992–2002 [19]. Inthe United Kingdom, 342 of 821 live born infants (42%)in 1985–2006 had CHD [20]. Present a figure showingan increasing prevalence from approx. 30% in the late
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1Page 4 of 14Table 1 Overview of included articles. Studies from the United States are presented followed by international studiesCountry or regionStudy designBean et al.(2011) [9]United States; Georgia, NewYork, Arkansas, Iowa, NewJersey, CaliforniaBogarapu et al.(2016) [25]Cleves et al.(2007) [8]Year of birthor studyperiodStudyparticipantswith DS (n)Internal validity /external validity(good, fair, poor)Case-control,National registrypopulation-basedBorn 2001–20041097Good / GoodUnited States; Utah, IdahoCohort,Regional databasepopulation-based and medical recordsBorn 2000–2012408Good / FairUnited States; multiple statesCase-control,National 211,372Good / GoodCua et al. (2017) United States; multiple states[15]Cohort,National databasepopulation-basedBorn 2000–20145737Good / FairFerencz et al.(1989) [31]United States; Maryland,Washington DC, VirginiaCross-sectional,Review of recordspopulation-basedEnrolled ( 1year of age)1981–1986218Fair / FairFreeman et al.(1998) [13]United States; GeorgiaCross-sectional,Regional databasepopulation-basedBorn 1989–1995227Good / GoodFreeman et al.(2008) [10]United States; Georgia, NewYork, Arkansas, Iowa, NewJersey, CaliforniaCase-control,National registry,Born 2000–population-based review of records, and 2004parent survey1469Good / GoodGreenwoodUnited states; Massachusettset al. (1976) [27]Cohort, singlecenterReview of recordsAdmitted1962–1973369Fair / FairKhoury et al.(1992) [14]Repeated crossRegional databasesectional,population-basedBorn 1968–1989532Good / GoodMcElhinneyUnited States; Pennsylvaniaet al. (2002) [29]Cohort, singlecenterReview of recordsNeonatalexamination1988–1999114Fair / FairPark et al.(1977) [32]United States; Maryland,PennsylvaniaCohort, twocenterReview of recordsReferred toclinics 1964–1972251Fair / FairSpahis et al.(1999) [30]United States; TexasCohort, singlecenterReview of recordsAttendingclinic 1993–1999216Good / FairTandon et al.(1973) [28]United States; MinnesotaCross-sectional,single-centerPost mortemexaminationsNot reported55Poor / FairTorfs et al.(1998) [12]United States; CaliforniaCross-sectional,Regional databasepopulation-basedBorn 1983–19932894Good / GoodTorfs et al.(1999) [12]United States; CaliforniaCase-control,Regional databasepopulation-based and interview ofmothersBorn 1991–1993687Good / FairWells et al.(1994) [26]United States; AlabamaCase series,single-centerReview of recordsBorn 1988–1992102Good / GoodAli et al. (2009)[61]SudanCohort, singlecenterReview of recordsAttendingclinic 2004–200780Poor / FairAynaci et al.(1998) [55]TurkeyCohort, singlecenterReview of recordsNot reported31Fair / FairBenhaourechMoroccoet al. (2016) [59]Cohort, singlecenterHospital registryDiagnosed128with DS 2008–2014Fair / FairBergstro et al.(2016) [15]SwedenRepeated crossNational registrysectional,population-basedBorn 1992–20122588Good /GoodBermudez et al.(2015) [39]BrazilCross-sectionaland cohort,single-centerAttendingclinic 2005–20131207Fair / FairUnited States; GeorgiaData sourceReview of records
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1Page 5 of 14Table 1 Overview of included articles. Studies from the United States are presented followed by international studies (Continued)Country or regionStudy designData sourceYear of birthor studyperiodBoussouf et al.(2017) [58]AlgeriaCase-control,multicenterClinical examinationand medical historyEnrolled 2009– 1102010Fair / FairBrodwall et al.(2018) [18]NorwayCohort,National registrypopulation-basedBorn 1994–20091251Good / FairCorona-RiveraMexicoet al. (2019) [34]Case-control,single-centerHospital registryBorn 2009–2018231Good / FairEl-Gilany et al.(2017) [21]EgyptCase-control,single-centerReview of recordsBorn 1992–20161720Good / FairElmagrpy et al.(2011) [60]LibyaCross-sectional,single-centerReview of recordsReferred toclinic 1995–20081193Good / FairEvans et al.(1950) [47]EnglandCross-sectional,single-centerPost mortemexaminationsNecropsies1911–194928Fair / PoorIrving et al.(2011)United KingdomCohort,Regional databasepopulation-basedBorn 1985–2006821Fair / FairJaruratanasirikul Thailandet al. (2017) [19]Cohort,Regional registry andpopulation-based medical examinationBorn 2009–2013153Good / FairKällén et al.(1996) [17]Cross-sectional,Regional and national Born 1976–population-based registries19935571Fair / GoodKim et al. (2014) Korea[24]Cross-sectional,National databasepopulation-basedBorn 2005–2006394Good / FairKörten et al.(2016) [41]GermanyCohort,National registrypopulation-basedBorn 1950spost 20001549Good /FairLiu et al. (1959)[46]EnglandCase series andcase-control,single-centerReview of recordsand post mortemexaminationsAdmitted to216hospital 1944–1958Fair / PoorLivingstoneSinclair et al.(2018) [35]JamaicaCohort, singlecenterReview of recordsAttendingclinic 2012–201541Fair / PoorMatsuo et al.(1972) [56]JapanCross-sectional,single-centerClinical examinationand post mortemexaminationsReferred toclinic 1966–1968106Fair / FairMokhtar et al.(2001) [22]EgyptCase-control,single-centerReview of recordsand parent surveyAttendingclinic 1995–2000514Fair / FairMorris et al.(2014) [16]Europe, 28 countriesRepeated crossNational and regionalsectional,registriespopulation-basedBorn 2000–20107044Good / GoodMorsy et al.(2016) [49]Saudi ArabiaCross-sectional,single-centerLocal databaseReferred toclinic 2008–2013302Fair / FairMuntha et al.(2019) [57]EthiopiaCohort, singlecenterReview of recordsBorn 2010–2015116Fair / PoorNarayanan et al. India(2014) [52]Cross-sectional,single-centerClinical examinationAttendingclinic 2005–2012418Fair / FairNisli et al. (2008) Turkey[54]Cross-sectional,single-centerReview of recordsAttendingclinic 1994–20071042Fair / FairPinto et al.(1990) [44]PortugalCross-sectional,single-centerReview of recordsAttendingclinic 1970–1987210Fair / FairRowe et al.(1961) [33]CanadaCohort, singlecenterClinical and postmortem examinationReferred toclinic 1955–1957174Fair / PoorFrance, Italy, SwedenStudyparticipantswith DS (n)Internal validity /external validity(good, fair, poor)
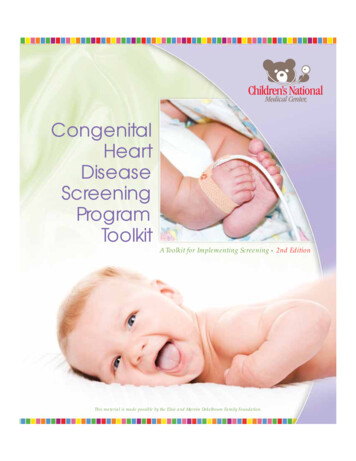
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1Page 6 of 14Table 1 Overview of included articles. Studies from the United States are presented followed by international studies (Continued)Country or regionStudy designSantoro et al.(2018) [40]ItalySelikowitz et al.(1992) [62]AustraliaYear of birthor studyperiodStudyparticipantswith DS (n)Internal validity /external validity(good, fair, poor)Cross-sectional,Regional registrypopulation-basedBorn 2003–2015230Fair / FairCross-sectionalParent survey,recruited atconferenceBorn 1974–1987204Poor / FairSica et al. (2015) Brazil[38]Cross-sectional,single-centerReview of recordsAttendingclinic 2011–201268Fair / FairStoll et al.(1998) [45]FranceCase-control,Regional registrypopulation-basedBorn 1979–1996398Fair / FairStoll et al.(2001) [42]Europe; 12 countriesCross-sectional,National and regionalpopulation-based registriesRegistered1996–1998239Good / GoodTan et al. (2013) Singapore[51]Cross-sectional,two-centerReview of recordsBorn 1996–2010588Fair / FairTomlinson et al. Jamaica(2010) [36]Cohort, singlecenterHospital registryBorn 1995–200476Fair / FairTubman et al.(1991) [43]Cohort,Clinical examinationpopulation basedBorn 1987–198981Fair /FairVenugopalanOmanet al. (2003) [53]Cross-sectional,single-centerReview of recordsAttendingclinic 1995–199854Fair / FairVida et al.(2005) [37]Cross-sectional,single-centerReview of recordsAttendingclinic 1997–2003349Fair / FairIrelandGuatemalaData sourceWeijerman et al. The Netherlands(2010) [23]Cohort,National registrypopulation-basedBorn 2003–2006482Good / GoodYaqoob et al.(2019) [50]PakistanCohort, singlecenterReview of recordsAttendingclinic 2010–2016350Poor / FairZahari et al.(2019) [48]MalaysiaCohort, twocenterHospital database and Born 2006–review of records2015754Good / FairYear of birth denotes birth of the DS cases included in each studyDS Down syndrome1980s to approx. 50% in the early 1990s following whichthe prevalence seemed to stabilize around 40–50% until2006 [20]. In Egypt, a downward trend in the prevalenceof CHD (from 56.2% in the birth cohort 1992–1996 to25% in the birth cohort 2012–2016) was observed in oneclinic (p .001) [21], while in another, the proportion ofinfants with DS and CHD increased from 29.8% in 1995to 48.2% in 2000 [22].Prevalence of CHD was reported at single time pointsin two international studies, including: 207 of 482 (43%)children with DS in the Netherlands born 2003–2006[23] and 224 of 394 (56.9%) infants with DS in Korea in2005–2006 [24]. One article was initially included, buton critical review was identified to have exclusion criteria which would make results regarding prevalence notgeneralizable, and is excluded from Fig. 2 [25].In summary, in the eighteen studies cited above, wefound that the total prevalence of CHD in DS rangedfrom 20 to 57.9%, mean 44.8% in DS patients born fromthe early 1970s to 2015 (Fig. 2). Over time, studies showan increasing prevalence in the late 1980s-early1990sfrom around 30% to around 50% following which theprevalence seems to stabilize around 40–55% until 2015(Fig. 2). The findings indicate an apparent increase in reported CHD prevalence in the first 10–15 years of thisperiod from around 20–30% to around 40–55%. Thetotal prevalence rates varied over time: increased in Atlanta from 1970s to 1980s due to increased CHD ascertainment [15], decreased in Egypt from 1992 to 1996 to2012–2016 [21], and was unchanged in Sweden from1992 to 2012, in Europe from 2000 to 2010, and inThailand from 1992 to 2013 [8, 16, 19].2. What is the type of congenital heart disease in DS?And, has the type of congenital heart disease in DSchanged over time?
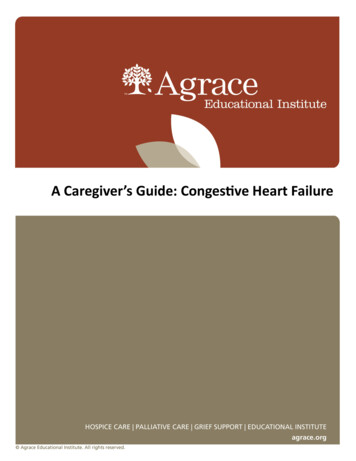
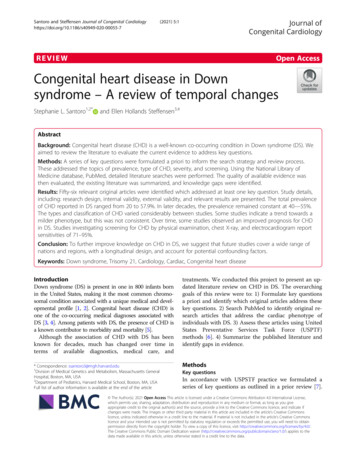
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1Page 7 of 14Fig. 2 CHD total prevalence. Overview of studies (assessed as population-based) reporting total prevalence of CHD among all DS patients.Studies are ordered according to period of birth midpoint/study period midpoint. CHD: congenital heart defect. DS: Down syndromeFifteen studies in the United States specified the types ofCHDWith the study population in a single city [2] of Atlanta[14, 15], specific states [7] including Alabama [26], California [12, 13], Massachusetts [27], Minnesota [28],Pennsylvania [29] and Texas [30], regions [2] of Maryland / Washington DC / Virginia [31], and Maryland /Pennsylvania [32], or multiple states [4] [5, 10, 11, 25].These studies used databases, registries, and clinical records, and were all retrospective reviews. None of thesefifteen studies described the type of CHD longitudinally.Thirty-nine articles outside the United States provided dataon the type of CHD in DSFive studies in North America including: Canada [33],Mexico [34], Jamaica [35, 36], and Guatemala [37]. Twostudies in South America, including: Brazil [38, 39].Eleven in Europe including: Italy [40], Norway [18],Germany [41], United Kingdom [20], Netherlands [23],Europe (multiple countries) [42], Ireland [43], Portugal[44], France [45], England [46, 47]. Eleven studies in Asiaincluding: Malaysia [48], Thailand [19], Saudi Arabia[49], Pakistan [50], Korea [24], Singapore [51], India[52], Oman [53], Turkey [54], Turkey [55], Japan [56].Seven studies in Africa including: Ethiopia [57], Algeria[58], Egypt [21], Morocco [59], Libya [60], Sudan [61],Egypt [22]. One study from Australia [62]. The type ofCHD for all studies is reported in the SupplementalTable and summarized in Fig. 3 (including studies whereCHD types are reported as proportion of DS patients)and Fig. 4 (including studies where CHD types are reported as proportion of all CHD types found). The figures show variable proportions of types of defects acrossperiods of birth/study periods. In Fig. 3, the majority ofstudies covering the period approx. Late 1960s to mid1990s observe a greater proportion of complex defects(atrioventricular septal defect (AVSD), aortic arch abnormalities, tetralogy of Fallot, transposition of the greatarteries, and single ventricle hearts) compared withshunt defects (isolated ventricular septal defect (VSD),isolated atrial septal defect (ASD), and isolated patentductus arteriosus). In contrast, studies covering lateryears more often find the proportion of shunt defects exceeding the proportion of complex defects. In studies
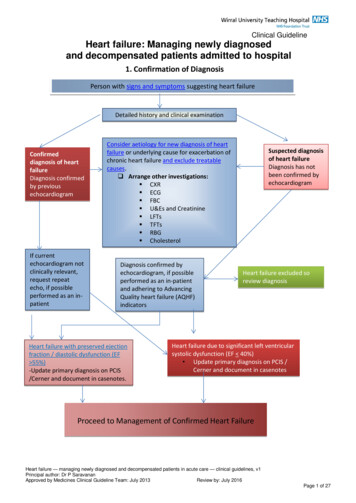
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1Page 8 of 14Fig. 3 Distribution of CHD types among DS patients. Proportion of DS patients with a given CHD grouped according to [15, 8]: complex defects (AVSD, aorticarch abnormalities, tetralogy of Fallot, transposition of the great arteries, and single ventricle hearts), valve defects (aortic, pulmonary, and mitral-tricuspid valvedefects), shunt defects (isolated VSD, isolated ASD, and isolated patent ductus arteriosus), and other defects [15]. do not report prevalence rates for the latterthree groups according to year of birth, so for this study only proportions of complex defects are displayed in the figure. CHD: congenital heart defect. DS:Down syndrome. AVSD: atrioventricular septal defect. VSD: ventricular septal defect. ASD: atrial septal defectreporting on the number of CHD types out of all CHDscovering the period 1968–2018 (Fig. 4) shunt defectswere consistently reported at higher proportions thancomplex defects.Six articles described the type of CHD longitudinallyIn the United States, one study found an increasingprevalence during the 1980s of ascertained patent ductusarteriosus, endocardial cushion defects and ASD [15]. InSweden, the risk of complex CHD (as defined in Figs. 3and 4) decreased over time: compared with 1992 to1994, the risk in 2010 to 2012 was reduced by almost40% (adjusted risk ratio 0.62, 95% confidence interval0.48–0.79) [8]. In contrast, chances for isolated VSD orASD showed significant increases during later years, andalthough AVSD was far more common than VSD in1992 to 1994, they were equally common in 2010 to2012 [8]. Results from the United Kingdom, may supportthis finding [20]. Here, the proportions of ASD increasedfrom approx. 9% in 1985–1989 to approx. 19% in 2000–2006 (our estimates based on the Fig. 3 in the article byIrving et al. [20]).However, a 28-country, population-based study usingcongenital anomaly registries in Europe in 2000–2010found no evidence of a trend in the proportions of birthswith DS with a severe cardiac anomaly (either of: singleventricle, hypoplastic left heart, hypoplastic right heart,Ebstein anomaly, tricuspid atresia, pulmonary valve atresia, common arterial truncus, AVSD, aortic valve atresia/stenosis, transposition of great vessels, tetralogy of Fallot,total anomalous pulmonary venous return, and coarctation of aorta) since 2000 [16]. There was no observedchange in prevalence of ASD and VSD among birthswith DS over the 10 years of study [16]. The authorssuggested that population screening for DS and subsequent terminations has not influenced the prevalence ofspecific congenital anomalies in these European infants[16]. Similarly, there was no apparent trend towards
Santoro and Steffensen Journal of Congenital Cardiology(2021) 5:1Page 9 of 14Fig. 4 CHD types as proportion of all CHDs. Frequencies of CHD types out of the total number of CHDs grouped according to [15, 8]: complexdefects (AVSD, aortic arch abnormalities, tetralogy of Fallot, transposition of the great arteries, and single ventricle hearts), valve defects (aortic,pulmonary, and mitral-tricuspid valve defects), shunt defects (isolated VSD, isolated ASD, and isolated patent ductus arteriosus), and other defects.CHD: congenital heart defect. DS: Down syndrome. AVSD: atrioventricular septal defect. VSD: ventricular septal defect. ASD: atrial septal defectlower prevalence of AVSD among live born DS patientsin Norway in 1994–2009 [18]. An Egyptian studyfound a decreasing prevalence of isolated CHD (asopposed to multiple CHD) from 56.2% in the birthcohort 1992–1996 to 19.8% in the birth cohort 2012–2016 [21].In summary, in the included articles, the type of CHDreported varies greatly (Fig. 3). The studies which provided longitudinal data differed in the location and year;there was no clear consensus if, or how, the prevalenceof specific types (complex, or severe) of CHD were changing over time.3. What is the severity of congenital heart disease inDS in terms of treatment and prognosis? And, hasthe severity of congenital heart disease in DSchanged over time?Seven articles addressed this key question regarding CHDseverityIn the United States during 2000–2014, neonates withDS who died
Full list of author information is available at the end of the article Journal of Congenital Cardiology Santoro and Steffensen Journal of Congenital Cardiology (2021) 5:1 . And, has the type of congenital heart disease in DS changed over time? 3. What is the severity of congenital heart disease in