Transcription
EnglandPROPOSED CONGENITAL HEARTDISEASE STANDARDS ANDSERVICE SPECIFICATIONSa consultation
NHS England INFORMATION READER ssioning StrategyHuman ResourcesPublications Gateway Reference:Patients and InformationCommissioning Development02196Document PurposeConsultationsDocument NameProposed congenital heart disease standards and servicespecifications: A consultationAuthorNHS EnglandPublication Date15 September 2014Target AudiencePublicAdditional CirculationListN/ADescriptionPublic Consultation Document for the proposed standards and servicespecifications for congenital heart disease.Cross ReferenceN/ASuperseded Docs(if applicable)Previous drafts of the Consultation Document as published on theNHS England -lead/chd/Action RequiredN/ATiming/Deadlines(if applicable)End of Consultation – 8 December 2014Contact Details forfurther informationNew Congenital Heart Disease Review Team (5th Floor)NHS EnglandQuarry HouseQuarry HillLeedsWest YorkshireLS2 7UEengland.congenitalheart@nhs.netDocument StatusThis is a controlled document. Whilst this document may be printed, the electronic version postedon our website is the controlled copy. Any printed copies of this document are not controlled.
NHS England Proposed congenital heart disease standards and service specifications: A consultation 3ContentsForeword. 4Executive summary. 5Part 1:Model of care for CHD services. 13Part 2:Introduction to the individual sections. 19Section A: The network approach. 19Section B: Staffing and skills.22Section C: Facilities.29Section D: Interdependencies. 31Section E: Training and education.34Section F: Organisation, governance and audit. 35Section G: Research. 37Section H: Communication with patients.38Section I: Transition.40Section J: Pregnancy and contraception.42Section K: Fetal diagnosis.44Section L: Palliative care and bereavement.46Section M: Dentistry.48Part 3:Introduction to the proposed service specification.49Part 4:Delivering the standards within existing resources.50Part 5:Making it happen. 53Part 6:What happens next?. 55Annex A:Consultation questions. 57
4 NHS England Proposed congenital heart disease standards and service specifications: A consultationForewordIn June 2013, the board of NHS England resolved tostart a fresh review of services for congenital heartdisease (CHD) with the aim of achieving the bestoutcomes for all patients, consistently across thewhole country, and with excellent patient experience.Reflecting the importance of this work, weestablished a board task and finish group to provideboard-level oversight.There have, of course, been previous reviews.Although we do not feel bound by what has gonebefore, we knew we could learn a great dealfrom those experiences. We embarked upon anapproach of openness and engagement from theoutset. We have been extremely fortunate: wehave been advised and informed by a wide range ofstakeholders, including patients and the public, andthose who represent them; clinicians; and hospitalmanagers. We have also had lively discussions withlocal authority and local Healthwatch representatives.These groups have told us that the key to ourapproach must be a set of national standards,consistently applied, covering the whole of a patient’slife. In that way we can help ensure that whereverpatients live, they will be able to access the bestpossible services.In the following pages we explain more aboutour review. We also set out the proposed nationalstandards, which have been drafted by expertgroups, widely discussed in consultative meetings,and finally considered and approved by the review’sClinical Advisory Panel.The proposed standards are in turn accompanied bydraft service specifications which are the mechanismfor incorporating the standards into our contractswith hospitals. As with every specialised service, thesespecifications were prepared by a Clinical ReferenceGroup with clinical and patient membership. We havesummarised the standards, setting out what we haveheard, what we are proposing and what we think thiswill mean. Where there has not been full agreementin discussions to date we say so, and explain thearguments, setting out our judgements and askingfor your views.Of course the world does not stand still, anddoubtless other initiatives will emerge in the future,but we are confident that the network-based systemwe have proposed for CHD services will be able toflex and adapt as needed. Everyone is aware thatthe NHS faces an extremely challenging financialsituation, and we need to work together to deliverhigh quality care within the resources available to us.The work we have done to assess the financial impactof the proposed standards suggests that for CHD thisis possible.I would like to once again thank the very manypeople who have given their time, good will,expertise and enthusiasm, and have offered supportand challenge in equal measure. The draft standardsand service specifications have been greatly enhancedthrough their input.In the same vein, I hope that as many as possible willrespond to this consultation in the spirit of opennessand engagement to which we are committed, andhelp us to ensure high quality care for all, now andfor future generations.Professor Sir Malcolm GrantChair of the Board Task and Finish Group
NHS England Proposed congenital heart disease standards and service specifications: A consultation 5Executive summaryCongenital heart disease (CHD) is the most commontype of congenital anomaly. It affects the normalworkings of the heart. It ranges from severe lifethreatening conditions that need immediate surgery,at or even before birth, to minor conditions thatoften do not need to be treated. All will requirespecialist diagnosis, monitoring and care throughoutthe person’s life.What difference will theseproposals make?Although relatively small in terms of patientnumbers, (around 9,400 children and adults had atleast one specialist inpatient episode in 2012/13)1and expenditure (around 1% of total spending onspecialised services)2, CHD services are a matter ofgreat public concern. Confidence in the service hasbeen undermined by many years of repeated reviewand investigation. Investment in the service has beenheld back because of continuing uncertainty. It is,therefore, important that this review is brought toa clear conclusion. We have heard that relationshipsbetween some hospitals have become strainedbecause previous reviews made them feel that theyneeded to compete against each other. Our proposalsaim to ensure that CHD services work together withinregions and across the country with the patient’s bestinterests as their prime concern.Early diagnosisMaking a diagnosis of CHD early helps with planningand can improve outcomes. As much as possible wewant to detect the problems before a baby is born.The first indication usually comes from the routinescan at 18-20 weeks. We heard that detection ratesvary across England and could be better. For example,according to 2011/12 data from the National Institutefor Cardiovascular Outcomes Research (NICOR), ofbabies requiring an intervention in the first yearof life, only 35% were diagnosed antenatally andthere is variation by area3. Our proposals aim toensure that patients receive the same high qualityscreening wherever they live and will receive thesupport, care, and information they need if ananomaly is suspected. We also heard that standards,by themselves, could not solve all the problems withlow detection rates. So we are also doing some morework in this area to understand the problems in moredetail and make separate proposals for improvement.Variations in service deliveryBabies born with CHD are among the most vulnerablepatients the NHS cares for. Services in England areconsidered to be good, but they could be evenbetter. We know that there is variation in the waydifferent providers deliver these services. Sometimesthis reflects providers delivering services in differentbut equally effective ways or one hospital developinga new technique or approach to care. But sometimesthere is no good explanation for the differences.Our proposals aim to ensure that every patient getsthe same high quality service wherever they live andwherever they receive their care.1NHS England analysis of Hospital Episode Statistics (HES) admitted patient care data2NHS England analysis of Secondary Uses Service (SUS) data for 2012/133NICOR data on antenatal diagnosis available at:https://nicor4.nicor.org.uk/CHD/an ment
6 NHS England Proposed congenital heart disease standards and service specifications: A consultationMaintaining and improvingoutcomesWhile surgery is only a small part of the patient’sexperience of CHD, it is a very important part.Everyone wants to make sure that every patient hasthe best chance of a good outcome. Results fromsurgery and catheterisation measured as survivalat 30 days, are very good at 98.2% in 2012/134(for providers that report to NICOR). But it is stillimportant to do everything we can to make sure theycontinue to be good and if possible to continue toimprove outcomes overall.We heard5 a lot about the optimal number ofsurgeons to have in a team, how many cases eachsurgeon should do each year to make sure they keeptheir skills, the importance of each surgeon onlytackling cases they have the skills to do, and howto make sure that patients with the rarest and mostcomplex conditions receive the best possible care.These discussions are set out in more detail later inthis document.Our proposals will ensure that each surgeon willdo enough operations to maintain their skills. Ourproposals also aim to ensure that surgeons work inteams big enough to protect against fatigue andburnout, to be able to cope with the loss of a surgeon(for example in the event of illness), to provide24-hour clinical cover all year round and seeingenough cases to develop and maintain skills inoperating on less common or more complexconditions. Finally, our proposals aim to ensure thatwherever patients receive their care, they will be seenby a doctor with the right skills, will be referred toanother doctor if they need more specialist care, orthe hospital will bring in expert support.We have described here the issues about surgery,but many of the same concerns affect interventionalcardiology, so we have made similar proposals forthis too.4NICOR data available at: http://nicor4.nicor.org.uk/CHD/an paeds.nsf/WMortality?Openview5What we have heard, CHD review blog 26 6/
NHS England Proposed congenital heart disease standards and service specifications: A consultation 7Patient-centred carePatients often have other problems as well as CHDand so need care from many specialists not just heartspecialists. We have been told that sometimes it cantake too long to get the help of other teams, andthat sometimes the different teams of doctors do notwork closely together. Our proposals aim to ensurethat wherever patients receive their care, all theexperts they are likely to need are on site or availablevery quickly.CHD is often a lifelong condition. Although muchcan be done to correct the problems this is notusually a complete cure. So it is important thatservices throughout life are joined together andhave a consistent approach. Our proposals includestandards covering every part of the patient’slife from early diagnosis in the womb throughchildhood, adolescence, adult life, planning afamily and onwards. We heard that moving fromchildren’s services to adult services (transition) can beparticularly difficult for young people. Our proposalsaim to ensure that young people and their familiesreceive more support at this difficult time and thatchildren’s CHD services and adult CHD services workmore closely together to manage transition.Adult congenital heart diseaseservices (ACHD)As a complete and systematic register of patientswith CHD is lacking, no reliable data exists on theprevalence of congenital cardiac anomalies. Severalattempts to estimate the prevalence of CHD havebeen undertaken over the past decade.However, we heard that the number of adults livingwith CHD is probably now greater than the numberof children and young people6. The prevalence inadults and median age of patients with severe CHDincreased in the general population from 1985 to2000. In 2000, there were nearly equal numbersof adults and children with severe CHD – based onresearch from North America7.‘Treatment of adults with congenital heart diseaseis relatively new as more children with congenitalheart defects receive treatment and reach adulthood.As a result of the success of paediatric cardiologyand cardiac surgery over the last four decades, itis thought that more adults with congenital heartdisease will require medical care than children.’British Heart Foundation8So, it is particularly important that we are clear whata good service for adults looks like. Our proposals setnational standards for adult congenital heart disease(ACHD) services for the first time. We heard thatsome problems remain in the service for adults thathave already been solved for children’s services. Theseinclude isolated and occasional practice. This couldbe where hospitals do not work in partnership withothers providing CHD services as part of a network,and/or where doctors undertake only a small numberof procedures that may be too low to develop andmaintain the right skills.Quality of careThe quality of care is not just about surgical skills andthe use of technology. We heard that patients wantto be more involved in decisions about their care, toreceive all the information they need to make gooddecisions and to be supported better, especially at themost difficult times. Our proposals aim to ensure thatpatients receive better information in a way they canunderstand and their views are taken into account.We have also set standards that will improvecommunication and support at all times, butparticularly when there is a suspicion that a baby may6Congenital Heart Disease in the General Population Changing Prevalence and Age Distribution, Marelli et al, (2007), Circulation –Journal of the American Heart Association7Delivery of care for adult patients with congenital heart disease in Europe: results from the Euro Heart Survey, Moons et al (2006)European Heart Journal 27, 1324–13308Children and young people: Statistics 2013 (2013) Townsend N, Bhatnagar P, Wickramasinghe K, Williams J, Vujcich D, Rayner M,British Heart Foundation: London
8 NHS England Proposed congenital heart disease standards and service specifications: A consultationhave CHD, when a patient is dying and when a familyis dealing with bereavement. As we have spokenwith patients and families we heard again and againhow important specialist (liaison) nurses were inproviding support and guidance, helping people tofind their way through the system. Our proposals willmake sure that there are enough specialist nurses toprovide that support for patients of all ages and theirfamilies. We also heard that psychologists can makea real difference for patients and families strugglingto come to terms with this illness and to make toughdecisions. So our proposals, for the first time, setstandards for numbers of psychologists and access tothe help they can give.Although most patients do not need to be inpatientsoften, some will need many admissions and somestays can be long. We heard that for patients andfamilies, spending a long time in hospital, especially ifthat is not near home, can be hard. So our proposalsaim to help patients, families and carers to be ableto live as normally as possible during times spentin hospital.Financial impactThe aim of the review is to ensure that servicesachieve the highest possible quality within theavailable resources. The available resources are notopen-ended and it is the duty of the NHS to ensureboth that it lives within its means and that it achievesthe maximum value for every pound it spends.So it is important to think about the cost of newproposals to ensure that they offer good value andto make sure that the NHS can afford to make theimprovements we are suggesting.Our analysis shows that if recent trends continuewe can expect that activity will increase whether ornot new standards are introduced. So spending onthese services by commissioners can be expected toincrease. Our assessment of the financial impact ofintroducing the standards indicates that the highercosts of providing the service to the new standardswill be met from the additional funding hospitalsreceive as activity levels increase. Introducing thestandards will ensure that this increase in spendingwill give us higher quality and not just more activity.
NHS England Proposed congenital heart disease standards and service specifications: A consultation 9The new CHD review: an overviewThe aims of the new CHD review are: securing the best outcomes for all patients, not just lowest mortality but reduced disability andan improved opportunity for survivors to leadbetter lives;tackling variations so that services acrossthe country consistently meet demandingperformance standards and are able to offerresilient 24/7 care; andimproving patient experience including howinformation is provided to patients and theirfamilies, and consideration of access andsupport for families when they have to be awayfrom home.This consultation on draft standards and servicespecifications is one part of the work of the review.We are also: analysing current and future demand for services; looking at the overall shape of the service that is provided;considering how best to commission any requiredimprovement and support the necessary change;reviewing how better, more timely informationcan be provided; andlooking at ways to achieve better earlier diagnosisof CHD.EvidenceTo ensure that we had the most reliable evidence onwhich to base our work, we asked The University ofSheffield’s School of Health Research and RelatedStudies (ScHARR) to undertake an independentreview of the literature. Their review considered‘What evidence is there for a relationship betweenorganisational features and patient outcomes incongenital heart disease services’.In addition NICOR was asked to examine its data andto advise on what this showed about service factorsthat could influence outcomes. Although the finalwrite up of this work is not yet available, NICORsupplied a summary of the main findings.We also benefited from a great deal of expert advice,both from clinicians and from patients and theirfamilies.“In my experience, the amount of quantitativescientific evidence available to guide us in decidinghow best to organise health services is often muchless than we would like. In these circumstances werely heavily on the views of experts, both specialistclinicians and those who are expert because oftheir experience of using the services in question.The views of experts, while qualitative rather thanquantitative, are also valid and an important sourceof evidence in our deliberations.”Professor Sir Michael Rawlins, Chair, ClinicalAdvisory PanelPrevalenceIt is estimated that across England and Walesbetween five and nine in every 1,000 pregnancies areassociated with some form of CHD9. Birth rates arevery difficult to predict but recently they have beenrising10. If this continues, the number of babies bornwith CHD will increase. In their ‘principal’ projections,the Office of National Statistics predict that birthrates will fall over the next ten years, but under their‘high’ projections, they recognise that they could alsocontinue to rise11.9Table 1.1 and 5.1, “Congenital Anomaly Statistics 2011, England and Wales”, BINOCAR, September 2013, found 202011 FINAL 040913.pdf10ONS Population Estimates 2002-2010 available ence-tables.html?edition tcm%3A77-26917111ONS Population projection 2012-2037 available ence-tables.html?edition tcm%3A77-318453
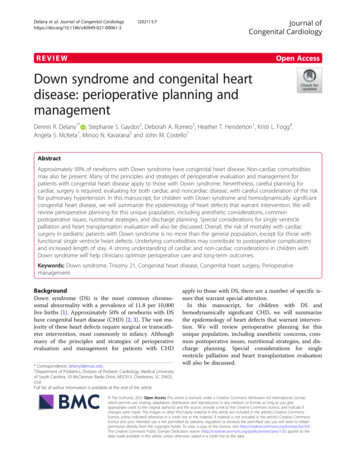
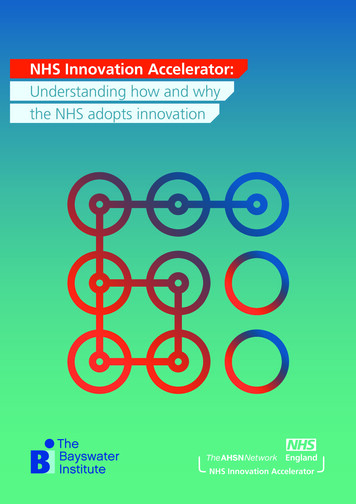
10 NHS England Proposed congenital heart disease standards and service specifications: A consultationBecause of improvements in treatment, peoplewith CHD can now expect to live longer than everbefore. Between 1979-1983 and 2004-2008, thenumber of deaths from CHD in children under 15years fell by 83% in the UK12. While the number ofadults with CHD is known to be increasing there isno reliable estimate of the number of people livingwith CHD. However, we do know that in the futurewe are likely to see the service moving from onethat is focussed on children, to one that is treatinga growing number of young people and adults13,who will continue to have (often complex) healthneeds. Even when anomalies have been treated inchildhood, further problems can develop later in lifethat require medical care or further surgery14. As thenumber of adults living with CHD rises, it will becomedifficult for Specialist Surgical Centres to managethe demand. So, it is important that we develop newways of working. Most patients, children and adults,will only receive a small part of their care at theSpecialist Surgical Centre. Our proposals set standardsfor Specialist and Local Cardiology Centres so thatmore care can be given closer to home, in hospitalsworking closely with the Specialist Surgical Centrewith agreed ways of working.Hospital activityFigure 1 shows how provider volume differs, withsome carrying out relatively low levels of activity15.Our proposals would mean that all doctorsundertaking interventional cardiology or surgeryfor CHD will be required to do a minimum numberof cases each year and decisions on how to treateach case will be made by the multidisciplinary team(MDT). This is designed to bring to an end occasionaland isolated practice.Some hospitals are not reporting their resultscentrally for audit and monitoring. NICOR estimate12Mortality with congenital heart defects in England and Wales, 1959-2009: exploring technological change through period andbirth cohort analysis Knowles RL, Bull C, Wren C, Dezateux C (2012) Arch Dis Child, 2012 Oct: 97(10): 861-513Delivery of care for adult patients with congenital heart disease in Europe: results from the Euro Heart Survey, Moons et al (2006)European Heart Journal 27, 1324–133014Care and Treatment for congenital heart defects (2011) American Heart rt-Defects UCM 002030 Article.jsp15NHS England analysis of HES data. The limitations of ACHD activity data are acknowledged. Providers with fewer than 20 episodesnot included as very low level activity could be data coding issue
NHS England Proposed congenital heart disease standards and service specifications: A consultation 11Figure 1: 2012/13 specialist inpatient episodes of care, for paediatric cardiac and ACHDservices, by provider (anonymised)HES Episodes (Paed cardiac and ACHD) 2012/13160014001200100080060040020001 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36Providers (anonymised)that around 80% of current adult activity is reportedto their congenital audit. Our proposals aim to ensurethat all hospitals providing care for CHD patientsare part of networks and report their results to thenational audit (NICOR).Developing the draft standardsand service specificationsWhen we started our work, patients, the public,clinicians and providers told us that the best wayto improve CHD services was through clear servicestandards, consistently applied.NHS England is responsible for buying all specialisedCHD services in England, so we have an opportunityto ensure consistently high standards for patientseverywhere.Professor Sir Bruce Keogh, NHS England NationalMedical Director noted:“The aim of the review is to ensure that servicesachieve the highest possible quality within theavailable resources, now and for future generations the standards [must] set out what is needed toachieve this”.Taking Sir Bruce’s challenge, we have aimed to set outstandards for services of the highest possible quality.People told us that this was important, even if itlater proved necessary to make tough choices whenconsidering how to put them into practice and whatwe can afford within the available resources.Work on developing standards for children’s andadult CHD services was already underway when thenew review was set up. We have worked with groupsof practising clinicians from most Specialist SurgicalCentres in England and patient representatives todevelop the standards and to draw the differentpieces of work together into a single coherent set.During this process, we have also discussed thestandards with our engagement and advisory groups(patients and public, clinicians, and providers) andwith the Congenital Heart Services Clinical ReferenceGroup (CRG), met with patients and staff in allSpecialist Surgical Centres and with children andyoung people from all over the country. Finally thestandards have been considered by a national, expertClinical Advisory Panel. We have provided updates onour work in a fortnightly blog on the NHS Englandwebsite. For the first time, we can set standards forCHD services right across the whole life-course fromfetal diagnosis through children’s and adult servicesincluding transition and pregnancy, to end of life careand bereavement.
12 NHS England Proposed congenital heart disease standards and service specifications: A consultationThe draft standards in detailThe draft standards will help ensure thatCHD patients across the country receive thebest possible care, within existing resources,now and in the future. The standardspropose a joined-up system where care isprovided through a network of serviceswith the patient at the centre.There are 13 sections, listed from A-M (networks todentistry):Section A:Section B:The network approachStaffing and skillsSection C:FacilitiesSection D:InterdependenciesSection E:Training and educationSection F:Organisation, governance and auditSection G:ResearchSection H:Communication with patientsSection I:TransitionSection J:Pregnancy and contraceptionSection K:Fetal diagnosisSection L:Palliative care and bereavementSection M:DentistryThis consultation document summarises the issuesand lists the consultation questions and providesan introduction to the draft standards and servicespecifications. In the following pages we give anoverview of what each section covers. We then sumup what we have heard so far and what we areproposing. Some sections are longer than others. Thisreflects the level of discussion there has been and thedetail in the standards.The standards describe how services should beorganised and delivered. They do not makerecommendations about what treatments should beused or which patients should receive them.The service specifications bring the standards into thecontractual arrangements between NHS England andhospitals providing CHD services.While this consultation document provides asummary, the full draft standards and servicespecifications are available online congenital-heart-disease-standardsThere are consultation questions throughout thedocument and they are also listed together at AnnexA. We have set out some key questions on which weare keen to hear your views, but if there are otherareas you would like to comment on, we will behappy to receive those too, although we may not beable to reflect those in our analysis of consultationresponses.CHD review reference packAt the same time, the Congenital Heart ServicesCRG has developed service specifications. Thesemake it possible for NHS England to ensure that thestandards are part of its contracts with hospitals.The reference pack includes a selection of keydocuments for convenience of access, though all ofthese and others have previously been posted on theNHS England website.There is broad agreement on most of the proposedstandards, but there are some issues where noteveryone agrees. Where this is the case, we discusst
End of Consultation - 8 December 2014: Contact Details for : further information: New Congenital Heart Disease Review Team (5th Floor) NHS England Quarry House . Congenital heart disease (CHD) is the most common type of congenital anomaly. It affects the normal : workings of the heart. It ranges from severe life