Transcription
Healthy Profession.Healthy Australia.Standards for general practices5th editionracgp.org.au
Standards for general practices, 5th editionDisclaimerThe information set out in this publication is current at the date of first publication and is intended for use asa guide of a general nature only and may or may not be relevant to particular patients or circumstances. Noris this publication exhaustive of the subject matter. Persons implementing any recommendations containedin this publication must exercise their own independent skill or judgement or seek appropriate professionaladvice relevant to their own particular circumstances when so doing. Compliance with any recommendationscannot of itself guarantee discharge of the duty of care owed to patients and others coming into contact withthe health professional and the premises from which the health professional operates.Accordingly, The Royal Australian College of General Practitioners Ltd (RACGP) and its employees andagents shall have no liability (including without limitation liability by reason of negligence) to any users of theinformation contained in this publication for any loss or damage (consequential or otherwise), cost or expenseincurred or arising by reason of any person using or relying on the information contained in this publicationand whether caused by reason of any error, negligent act, omission or misrepresentation in the information.Recommended citationThe Royal Australian College of General Practitioners. Standards for general practices. 5th edn.East Melbourne, Vic: RACGP, 2020.The Royal Australian College of General Practitioners Ltd100 Wellington ParadeEast Melbourne, Victoria 3002Tel 03 8699 0414Fax 03 8699 0400www.racgp.org.auABN: 34 000 223 807ISBN: 978-0-86906-470-2 (web)ISBN: 978-0-86906-473-3 (print)Published July 2017; updated December 2018, November 2019, March 2020, July 2020, April 2021,May 2021, November 2021, January 2022 The Royal Australian College of General Practitioners 2020This resource is provided under licence by the RACGP. Full terms are available at www.racgp.org.au/usage/licence. In summary, you must not edit or adapt it or use it for any commercial purposes. You mustacknowledge the RACGP as the owner.We acknowledge the Traditional Custodians of the lands and seas on which we work and live, and pay ourrespects to Elders, past, present and future.ID-2261
Standards forgeneral practices5th edition
Standards for general practices, 5th editionContentsIntroduction to the Standards for general practices (5th edition)1Development of this edition1Changes from the previous edition1Revised structure1Numbering of Criteria and Indicators2Indicators that focus on outcomes and patients3Fewer Indicators3Restructured explanatory notes3Use of ‘could’ and ‘must’3Plain English3Reduced citation of federal, state or territory legislation4Evidence-based standards4Accreditation4Practices that can be accredited4Voluntary accreditation4The accreditation cycle5The assessment process5Requirements for accreditation agencies and surveyors6and aspirational Indicators7MandatoryDemonstrating compliance7The Resource guide7Core moduleCore Standard 1910Criterion C1.1 – Information about your practice11Criterion C1.2 – Communications13Criterion C1.3 – Informed patient decisions16Criterion C1.4 – Interpreter and other communication services19Criterion C1.5 – Costs associated with care initiated by the practice22Core Standard 224Criterion C2.1 – Respectful and culturally appropriate care25Criterion C2.2 – Presence of a third party during a consultation30Criterion C2.3 – Accessibility of services32iii
ivStandards for general practices, 5th editionCore Standard 334Criterion C3.1 – Business operation systems35Criterion C3.2 – Accountability and responsibility39Criterion C3.3 – Emergency response plan43Criterion C3.4 – Practice communication and teamwork45Criterion C3.5 – Work health and safety48Criterion C3.6 – Research51Core Standard 4Criterion C4.1 – Health promotion and preventive careCore Standard 5545557Criterion C5.1 – Diagnosis and management of health issues58Criterion C5.2 – Clinical autonomy for practitioners60Criterion C5.3 – Clinical handover61Core Standard 663Criterion C6.1 – Patient identification64Criterion C6.2 – Patient health record systems66Criterion C6.3 – Confidentiality and privacy of health and other information68Criterion C6.4 – Information security72Core Standard 7Criterion C7.1 – Content of patient health recordsCore Standard 8Criterion C8.1 – Education and training of non-clinical staff77788485References87Quality improvement module89QI Standard 190Criterion QI1.1 – Quality improvement activities91Criterion QI1.2 – Patient feedback94Criterion QI1.3 – Improving clinical care97QI Standard 2100Criterion QI2.1 – Health summaries101Criterion QI2.2 – Safe and quality use of medicines103
Standards for general practices, 5th editionQI Standard 3106Criterion QI3.1 – Managing clinical risks107Criterion QI3.2 – Open disclosure109References111General practice module113GP Standard 1114Criterion GP1.1 – Responsive system for patient care115Criterion GP1.2 – Home and other visits119Criterion GP1.3 – Care outside of normal opening hours121GP Standard 2124Criterion GP2.1 – Continuous and comprehensive care125Criterion GP2.2 – Follow-up systems128Criterion GP2.3 – Engaging with other services134Criterion GP2.4 – Transfer of care and the patient–practitioner relationship137GP Standard 3Criterion GP3.1 – Qualifications, education and training of healthcare practitionersGP Standard 4Criterion GP4.1 – Infection prevention and control, including sterilisationGP Standard 5139140144145152Criterion GP5.1 – Practice facilities153Criterion GP5.2 – Practice equipment156Criterion GP5.3 – Doctor’s bag160GP Standard 6Criterion GP6.1 – Maintaining vaccine potency164165References169Glossary170v
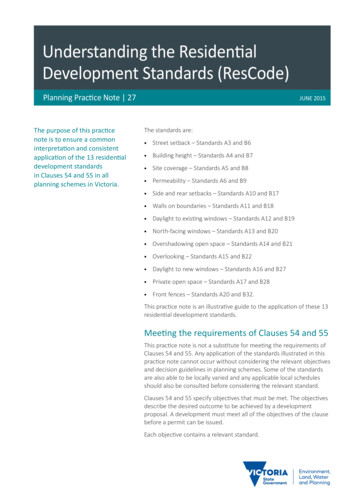
Standards for general practices, 5th editionIntroduction to the Standards forgeneral practices (5th edition)The RACGP’sStandards for generalpractices (5th edition):A benchmark forquality care andrisk management inAustralian generalpractices.The Royal Australian College of General Practitioners (RACGP) hasdeveloped the Standards for general practices (5th edition) (the Standards)with the purpose of protecting patients from harm by improving the qualityand safety of health services. The Standards also support general practicesin identifying and addressing any gaps in their systems and processes.Development of this editionThe fifth edition of the Standards was developed over a three-year periodin consultation with general practitioners (GPs), practice managers,nurses, consumers, technical experts, and many other stakeholders. Theprocess included: targeted stakeholder workshops throughout Australia three rounds of public consultation three rounds of testing and piloting.Changes from the previous editionRevised structureThe fourth edition of the Standards had five sections that accreditationsurveyors used as the basis of their assessments of general practices. Thefifth edition of the Standards has three modules that collectively cover all ofthe areas in the fourth edition, but in a different structure.This modular structure allows the RACGP to update the modulesseparately, and to adapt the Standards for other healthcare settings suchas correctional services and immigration detention centres. For example,the first two modules (the core module and the quality improvementmodule) are relevant for all healthcare settings, but the third module (thegeneral practice module) can be adapted to accommodate the specificneeds of each healthcare setting. Figure 1 (on the following page) illustratesthis modular approach and how it is different to previous editions.1
2Standards for general practices, 5th editionStandards for general practices(4th edition)Section 1PracticeservicesStandards for general practices(5th edition)Section 2Rights andneeds n 3Safety, qualityimprovementand educationSection 5PhysicalfactorsSection 4PracticemanagementStandards for other settings(ie correctional services, immigrationdetention centres, oremoduleOthersettingsFigure 1. Modular structure of the StandardsNumbering of Criteria and IndicatorsThe numbering system works as follows: The Standards in each module are numbered separately (Standards 1–8 in the core module, Standards1–3 in the quality improvement module, and Standards 1–6 in the general practice module). The Criteria for each Standard has a code indicating the module (C for core, QI for qualityimprovement and GP for general practice), followed by sequential numbering that indicates theStandard and Criterion. For example, C1.1 is the first Criterion for the first Standard in the coremodule; C1.2 is the second Criterion for the first Standard in the Core module; GP4.2 is the secondCriterion for the fourth Standard in the general practice module).Table 1 demonstrates the different structure between the Standards fourth and fifth editions.Table 1. Comparison between fourth and fifth edition structureNumbering in the Standards (4th edition)Numbering in the Standards (5th edition)Section 1: Practice servicesStandard 1.1: Access to careCriterion 1.1.1 – Scheduling care in opening hoursCore moduleStandard 1: Communication and patient participationCriterion C1.1 – Information about your practiceIndicatorsIndicatorsA. Our practice can demonstrate thatwe have a flexible system for determiningthe order in which patients are seen, toaccommodate patients’ needs for urgentcare, non-urgent care, complex care,planned chronic disease management,preventive healthcare and longerconsultationsC1.1 A Our patients can access up-to-dateinformation about the practice.At a minimum, this information contains: our practice’s address and telephone numbers our consulting hours and details of arrangements for careoutside normal opening hours our practice’s billing principles a list of our practitioners our practice’s communication policy, including when andhow we receive and return telephone calls and electroniccommunications our practice’s policy for managing patient healthinformation (or its principles and how full details can beobtained from the practice) the process we use to follow up on results how to provide feedback or make a complaint to the practice information about the range of services we provide
Standards for general practices, 5th editionIndicators that focus on outcomes and patientsThe Indicators in this edition have, where appropriate, been written with a focus on outcomes andpatients, instead of on prescribed processes or what the practice does.For example:Process-focused IndicatorOutcome-focused IndicatorOur practice has a documented system to identify, followup, and recall patients with clinically significant resultsOur practice recalls patients who haveclinically significant resultsBy focusing on outcomes, your practice can develop systems and processes that reflect yourpreferred ways of working, and choose how to demonstrate that you meet the intent of eachIndicator. It is important that you can provide evidence of meeting the Indicator, either throughinspection or interview. Focusing on outcomes will give your practice’s team greater ownershipof your processes and systems, making your team more likely to follow them not only duringaccreditation, but also before and after.Fewer IndicatorsThere are 14 fewer Indicators than in the fourth edition. The RACGP achieved this by: removing duplication merging Indicators that shared a similar theme focusing on outcomes rather than processes.Restructured explanatory notesThe explanatory notes for each Criterion now have three sections: Why this is importantThis section explains why the Indicators are important from a quality and safety perspective. Meeting this CriterionThis section sets out ways that your practice can choose to demonstrate that you meet thisCriterion and/or its Indicators. Meeting each IndicatorThis section contains a list of any mandatory activities your practice must do to meet theIndicator, and/or optional ways your practice can choose to meet the Indicator.This change was made as a direct result of feedback collected from stakeholders during theconsultation phases.Use of ‘could’ and ‘must’In the explanatory notes, the words ‘could’ and ‘must’ are used as follows: ‘Could’ is used to indicate that something is optional. ‘Must’ is used to indicate that something is mandatory.Plain EnglishIn response to feedback from stakeholders, this edition is written in plain English, therebyeliminating ambiguity and reducing the use of technical language.3
4Standards for general practices, 5th editionReduced citation of federal, state or territory legislationLegislation has been cited only where it is especially important to a particular aspect of general practice(eg in Criterion 6.3 ‘Confidentiality and privacy of health and other information’ in the core module).Therefore, most of the relevant federal, state or territory legislation has not been cited in this document.As federal, state or territory, and local legislation overrides any non-legislative standards, including thosein this document, your practice is responsible for ensuring that you comply with relevant legislation.If your practice is accredited against the Standards, you will have met some of your legislativerequirements, but this does not mean that you have automatically met all of them, as theStandards do not address all of the relevant state and territory legislation.Evidence-based standardsThe Standards are based on the best available evidence of how general practices can providesafe and quality healthcare to their patients.This evidence is based on two sources: Relevant studies Level IV evidence (where studies are not available). Level IV evidence is otherwise known asevidence from a panel of experts. To ensure that this Level IV evidence is as robust as possible,the Standards have been tested by Australian general practices and consumers, overseen byan expert committee consisting of GPs, academic GPs and nurses, practice managers, andconsumer representatives.AccreditationIf you want your practice to be accredited against the Standards, it must be formally assessed byan accrediting agency approved under the National General practice Accreditation Scheme (theScheme), which commenced on 1 January 2017.Practices that can be accreditedBefore a practice or health service is eligible to be accredited against the Standards, it needs tomeet three core criteria.The three criteria: The practice or health service operates within the model of general practice described in theRACGP’s definition of general practice, available at eneral-practice GP services are predominantly of a general practice nature. The practice or health service is capable of meeting all mandatory indicators in the Standards.Voluntary accreditationThe RACGP supports accreditation as a voluntary scheme.
Standards for general practices, 5th editionThe accreditation cycleThe accreditation cycle is three years. This means that if your practice achieves accreditationagainst these Standards, the accreditation is valid for the remainder of the three-year cycle inwhich you achieved accreditation. To maintain your accreditation, you must be successfully reassessed for the next accreditation cycle.The assessment processIf you want your general practice to be accredited, you must select an approved accreditationagency from the list of agencies available at ce-accreditationEach accreditation agency has trained surveyors who assess general practices. The agency youselect will work with your practice to help you prepare for the accreditation process. They will alsoappoint a team of surveyors who visit each location from which your practice operates to assessyour practice against the Standards.Surveyor teamsSurveyor teams are comprised of at least two surveyors, one of whom must be an appropriatelyqualified GP surveyor and one of whom must be an appropriately qualified nurse, practicemanager, allied health professional or Aboriginal and Torres Strait Islander health worker/healthpractitioner with relevant experience in general practice.Surveyor teams may include a third person, such as a non-health practitioner or consumer whohas been appropriately trained in the Standards.Fair and independent assessmentsAccreditation assessments are based on common sense: the accreditation agencies will not seekto penalise or exclude a practice from accreditation due to technicalities.The RACGP considers that an independent review of your practice that includes two or moresurveyors (one GP and one or more non-GP surveyors) will foster genuine collaboration andsharing of expertise among peers.5
6Standards for general practices, 5th editionRequirements for accreditation agencies and surveyorsThe RACGP has developed requirements that accrediting agencies and surveyors must meet inorder to be granted permission to use the Standards to assess general practices, as outlined below.By ensuring that bodies have appropriate systems, processes and commitment, and thatsurveyors have the appropriate skills, qualifications and experience, the accreditation process hasthe required rigour and level of accountability.Accrediting agenciesIn order to use the Standards, accrediting agencies are required to demonstrate the following tothe RACGP: An in-depth understanding of– the Standards– the nature of general practice in Australia– requirements for training and vocational registration of GPs An accreditation assessment framework that includes a single onsite assessment that isconducted once every three years at each location that the practice operates from The capacity to efficiently accredit general practices across Australia A governance and advisory structure that includes GPs with considerable experience in generalpractice A commitment not to refuse an application for accreditation from a practice that meets theRACGP’s definition of a general practice, regardless of location or size A commitment not to financially or otherwise discriminate against a practice because oflocation or sizeAll surveyorsSurveyors must: demonstrate a good understanding of confidentiality issues relating to general practice,personal health information and patient privacy meet requirements relating to their previous and recent experience complete ongoing surveyor training as required by the Scheme to maintain their competenceand knowledge of the Standards.GP surveyorsGP surveyors must: be vocationally registered under the Health Insurance (Vocational Registration of GeneralPractitioners) Regulations 1989 hold either Fellowship of the RACGP (FRACGP) or the Australian College of Rural and RemoteMedicine (ACRRM) if appointed after 31 October 2017 have at least five years’ full-time or equivalent part-time experience as a vocationally registeredGP and– be working at least two sessions a week in face-to-face patient contact in an accreditedgeneral practice, and have done so for the last two years
Standards for general practices, 5th editionor– have worked at least two sessions a week in face-to-face patient contact in an accreditedgeneral practice within the last two years satisfy their college’s requirements for their continuing professional development (CPD) program.Non-GP surveyorsNon-GP surveyors: can be an appropriately qualified nurse, practice manager, allied health professional orAboriginal and Torres Strait Islander health worker or health practitioner must have at least five years’ full-time equivalent experience, and– must be working at least 16 hours a week in an accredited general practice, and have doneso for the last two yearsor– have worked at least 16 hours a week in an accredited general practice for at least two years,and not more than two years ago.Mandatoryand aspirational IndicatorsIndicators marked with the symbol are mandatory, which means that your practice mustdemonstrate that you meet this Indicator in order to achieve accreditation against the Standards.Indicators that are not marked with the mandatory symbol are aspirational Indicators. The RACGPencourages you to meet the aspirational Indicators, but they are not essential to achieve accreditation.Demonstrating compliancePrevious editions of the Standards dictated how practices must demonstrate compliance with theStandards (eg by interview, document review, observation).However, because this edition of the Standards is outcomes-focused (instead of processfocused), your practice can choose how to demonstrate that you meet the intent of each Indicator,and the evidence that you choose to support this. The accreditation agency must only be satisfiedthat you meet the intent of each Indicator, and that you can provide appropriate evidence of this.This approach gives you greater scope to set up systems and processes that reflect your workingarrangements, which means the systems and processes will be more meaningful and relevant toyour practice.In the explanatory notes of each Criterion, there is a section titled ‘Meeting each Indicator’ that setsout the mandatory requirements of that specific Indicator, and includes some examples of what youcan do to meet it. While you may find some or all of these examples useful, it is not an exhaustivelist, and we encourage you to develop methods that best suit the needs of your practice.The Resource guideThe RACGP has developed a Resource guide that contains useful supplementary information thatwill help your practice meet the Indicators in the fifth edition of the Standards. The Standards,5th edn: Resource guide is available at ards/standards-5th-edition/resource-guide7
RACGP Standards for general practices, 5th editionCore moduleCore Standard 1Communication and patient participation10Core Standard 2Rights and needs of patients24Core Standard 3Practice governance and management34Core Standard 4Health promotion and preventive activities54Core Standard 5Clinical management of health issues57Core Standard 6Information management63Core Standard 7Content of patient health records77Core Standard 8Education and training of non-clinical staff84References879
10Standards for general practices, 5th editionCore Standard 1Communicationand patientparticipationOur practice providestimely and accuratecommunications thatare patient-centred.Communication with patients includes: communication that occurs before the consultation, during theconsultation and after the consultation verbal and written communication, and the use of interpreters,including sign language interpreters communication between the patient and– the practitioner– the practice team– other clinicians in the practice.Communication must be patient‐centred. This means that the practiceteam considers the patient’s values, needs and preferences, and givesthe patient time to provide input and participate actively in decisionsregarding their healthcare.1 Patients must be provided with the appropriateinformation they need to manage their condition.The practice must also consider the communication needs of carers andother relevant parties.
Standards for general practices, 5th editionCriterion C1.1 – Information about your practiceIndicatorC1.1 A Our patients can access up-to-date information about the practice.At a minimum, this information contains: our practice’s address and telephone numbers our consulting hours and details of arrangements for care outside normal opening hours appointment types our practice’s billing principles a list of our practitioners our practice’s communication policy, including when and how we receive and returntelephone calls and electronic communications our practice’s policy for managing patient health information (or its principles and how fulldetails can be obtained from the practice) how to provide feedback or make a complaint to the practice details on the range of services we provide.Why this is importantInformation about the practice, including the range and cost of services provided by the practice,is important to all patients.Meeting this CriterionThe format of the informationYou can provide this information in many formats, such as printed information sheets and text onthe practice’s website. Pictures and simple language versions help patients who would otherwisebe unable to read or understand the information. The practice needs to update this informationregularly so that it remains accurate. Ideally, the information is updated as soon as it changes.If your practice serves specific ethnic communities, provide access to written information in thelanguages most commonly used by your patients. You could also display the languages spokenby the practice team on an information sheet or on your website.Appointment typesThe information you provide to patients about appointment types needs to detail whether in-personand/or telehealth appointments are available and in what circumstances. Your practice could educate,and communicate with, patients about the process and the benefits of an appointment type beforethey take part, especially if a patient is unfamiliar with an appointment supported by technology.You could also advise patients of the different durations available for each appointment type.If your practice offers telehealth appointments, provide your patients with details on how to accessthese appointments, and the types of telehealth appointments available to them, such as: video, phone or other specialist-only telehealth appointments telehealth offered at certain times.11
12Standards for general practices, 5th editionAdvertisements in your practice informationIf any of the material providing information about your practice contains local advertisements,include a disclaimer that states that the inclusion of advertisements is not an endorsement by thepractice of those advertised services or products.Meeting each IndicatorC1.1 A Our patients can access up-to-date information about the practice.You must: make practice information available to patients update practice information if there are any changes.You could: create and maintain an up-to-date information sheet that contains all the required information inlanguage that is clear and easily understood create and maintain an up-to-date website that contains all the required information about thepractice in clear, simple language provide alternative ways to make the information available to patients who have low literacylevels (eg provide versions in languages other than English, and versions including pictures) provide brochures and/or signs in the waiting room, written in English and languages other thanEnglish, explaining– the practice’s policy regarding its collection, storage, use, and disclosure of personal andhealth information– the practice’s fees– available services– after-hours services display a list of names of the practice’s team members on duty make contact details of interpreters available train practice team members so that they can use the interpreter service.
Standards for general practices, 5th editionCriterion C1.2 – CommunicationsIndicatorC1.2 A Our practice manages communications from patients.Why this is importantEffective communication with patients via telephone and electronic communication (eg emails andtext messages) ensures that: patients can contact the practice when they need to patients can make appointments and receive other information in a timely fashion urgent enquiries are dealt with in a timely and medically appropriate way.Meeting this CriterionCommunicating by telephoneBefore putting a caller on hold, reception staff must first ask if the matter is an emergency.When a member of the practice team provides information (such as test results) to a patient bytelephone, they must make sure that the patient is correctly identified so that patient confidentialityis not compromised. To do this, they must obtain at least three of the following approved patientidentifiers (items of information that are accepted for use to identify a patient): Family name and given names Date of birth Gender (as identified by the patient) Address Patient health record number, where it exists Individual Healthcare IdentifierA Medicare number is not an approved identifier. Medicare numbers are not unique and somepeople have more than one Medicare number because they are members of more than onefamily and are on multiple cards. Also, some Australian residents and visitors may not have aMedicare number.2Communicating by electronic meansIf you choose to communicate with patients electronically (eg by telehealth, email, securemessaging or text message), you must: adhere to the Australian Privacy Principles (APPs), the Privacy Act 1988 and any state-specificlaws clearly state what content the practice team can and cannot send using electroniccommunication (eg your practice might require that sensitive information only be communicatedin person by a medical practitioner or other appropriate health professional, unless there areexceptional circumstances)13
14Standards for general practices, 5th edition inform patients that there are risks associated with some methods of electroniccommunications and that their privacy and confidentiality may be compromised obtain consent from the patient before sending health information to the patient electronically(consent is implied if the patient initiates electronic communication with the practice) or throughtechnology to undertake appointments document in patient health record the outcome of your request for consent to communicateelectronically check that the information is correct and that you are sen
Numbering in the Standards (4th edition) Numbering in the Standards (5th edition) Section 1: Practice services Standard 1.1: Access to care Criterion 1.1.1 - Scheduling care in opening hours Core module Standard 1: Communication and patient participation Criterion C1.1 - Information about your practice Indicators A. Our practice can .