Transcription
Hierarchical Condition Category (HCC) CodingMay 5, 2020 Amy H. Kotch, MHA Principal Business ConsultantMaria Nikol, MJ Senior Business ConsultantRyan T. Mackman, MBA, MHA Business Consultant, User Engagement Lead
Check-Up
PurposeHierarchical Condition Category (HCC)Coding aims to predict costs forMedicare beneficiaries based on diseaseand demographic risk factors
What is the Risk Adjustment Factor?Implemented in2004Derived fromICD-10 CodesFound WithinClaims DataUsed to AdjustCapitationPayments to MAPlansAffects ACOBenchmark
Why Should You Care?Use your words andspecific diagnosiscodes to tell the story!This is the only waythat CMS knows howsick your patients areand gives you credit forthe hard work you’redoing.
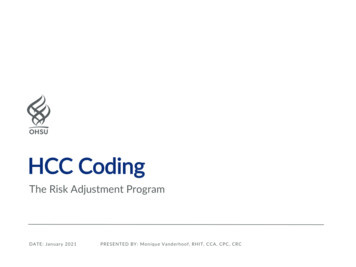
Patient ExampleCommon Primary Care Encounter75-year-old patient with type 2 diabetes a body mass index (BMI) of40.0 with complaints of numbness in his extremities.
Patient ExampleWhich Way Should You Code This Patient?Option 1: Some Conditions CodedICD-10DescriptionRAFE08.9Type 2 Diabetes with noComplications0.106Z68.37BMI of 37.00.106Option 2: All Conditions CodedICD-10DescriptionRAFE10.42Type 2 Diabetes with DiabeticPolyneuropathy0.307E66.01 & Z68.37Morbid Obesity with a BMI of 40.00.2620.569
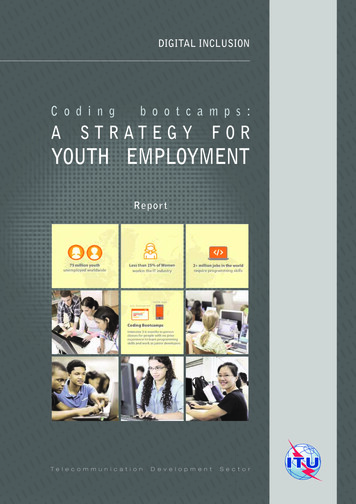
Patient ExampleCommon Primary Care EncounterPatient with DM II presents for routine follow-up.A1C 8.3. stable COPD, oxygen dependent.
Patient ExampleWhich Way Should You Code This Patient?Option 1: Some Conditions CodedICD-10DescriptionRAFJ44.9COPD.328E11.9DM Unspec.118.446Option 2: All Conditions Coded with hronic Resp Failure w/ Hypoxia.318E11.65DM w/ /documents/practice management/webcasts/hcc-crash-course.pdf
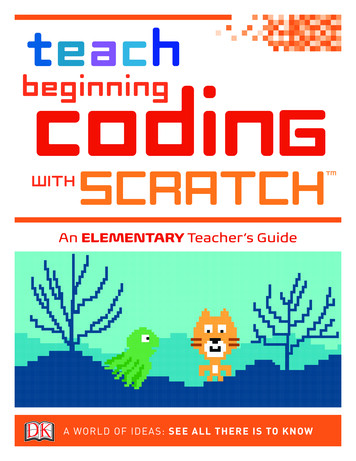
Impact of HCC on an ACOScenarioACO 1ACO 2ACO 3BaselineCostACOActualCostRAFRAF AdjustedBaseline Cost3% CapA 500 500 500B 501 501 501C0.9511.05D (A*C) 475 500 525E 485 500 515* Population Calculation in MillionsSavings/LossF (E-B)( 16,000,000)( 1,000,000) 14,000,000
Example of Provider Settings for CMS-HCCsShort-Term (General & Specialty) HospitalsCritical Access HospitalsChildren’s HospitalsLong-Term HospitalsRehabilitation HospitalsPsychiatric HospitalsReligious Non-Medical Health Care InstitutionsCommunity Mental Health CentersFederally Qualified Health CentersRural Health Clinic (Free-Standing & Provider-Based)
Diagnoses Documented by Select Provider Types areAppropriate for Coding and Reporting for CMS HCC CodingMD or DOOD Doctor of OptometryDC Doctor of ChiropractorDDS Doctor of Dental SurgeryDO Doctor of OsteopathyDPM Doctor of PodiatryAll Nurse Practitioners, Certified Nurse Specialists, CRNAsPhysician’s AssistantsTherapists; Speech, Physical, Occupational (Except “Respiratory”)Licensed Clinical Social Worker or Clinical Social WorkerCertified Wound Care and/or Ostomy Nurse
Using AWVs as Opportunity to Review Problem ListsBenefits of the AnnualWellness Visit Improve quality metrics Reduce churn/increase attribution Accurately reflect patient acuity (HCC scores)Components of theAnnual Wellness Visit Health Risk Assessment to review problem lists Review family & medical histories A maximum of 12 conditions can be coded per claimHCC Coding Opportunity 4 in the header
Pro TipsReview problem lists during the patient’s annual wellness visit and keep them to date and accurate- All chronic conditions need to be documented at least once annuallySelect the most specific ICD-10 and document it in the EHRAvoid using the term “history of” for chronic, but currently stable, conditionsSupport all coding with documentation using M.E.A.T.(Monitor, Evaluate, Assess/Address, and Treat)
M.E.A.T. Monitor: signs, symptoms, disease progression, disease regression Evaluate: test results, medication effectiveness, response to treatment Assess: ordering tests, discussion, review records, counseling Treatment: medications, therapies, other modalitiesFor every condition, follow M.E.A.T. to ensure proper documentationIf it was not documented, it does not exist!
M.E.A.T. ExamplesCHF symptoms, well controlled with Lasix, and ACE inhibitor. Will continue current medications. M CHF is well-controlled. E Lasix and ACE inhibitors required. A No additional testing necessary. T Continue current medications.
M.E.A.T. ExamplesHypertension remains stable; will continue with Losartan 100 mg daily M Hypertension remains stable. E Continue Losartan 100 mg daily. A No additional testing necessary. T Continue current medication.
National Stats on Risk ScoresAverage national HCC error rate is approximately33% according to CMSRural providers serve Medicare beneficiaries withlower average CMS-HCC risk scores than urbanproviders—1.43 compared to 1.75, respectively.Sources:(1) Average Beneficiary CMS Hierarchical Condition Category (HCC) Risk Scores for Rural and Urban Providers Abby F. Hoffman;Kristin L. Reiter, PhD; Randy K. Randolph, MPP(2) ure 16613&lat 37.52715361723378&long 81.507568359375&z 6&unit county&n 5&colors YlGnBu&overlay sharedsavings&hidemeasures 1
Resources
Thank YouAmy Holm Kotch, MHA Prin. Business Consultant Mobile: 914.275.6531 E-Mail: akotch@salient.comMaria Nikol, MJ Sr. Business Consultant Mobile: 410.812.7156 E-Mail: mnikol@salient.comRyan Mackman, MBA, MHA Business Consultant Mobile: 954.270.0692 E-mail: ase/salient-healthcare/
Hierarchical Condition Category (HCC) Coding aims to predict costs for Medicare beneficiari