Transcription
This step-by step guide will help you apply for certification as an Agency, NonAgency or Assisted Living provider.PLEASE NOTE: You must serve two consumers for a three month period prior toapplying for certification. If you have not served two consumers for a threemonth period, you are not eligible to apply until this condition is met.You begin the process by applying through Ohio Department of Jobs and Family Services (ODJS) websiteusing the Medicaid Information Technology System (MITS). Click on this id/43/Default.aspx. Select “Provider EnrollmentApplication” from the options listed on the right side of the screen.
PLEASE NOTE: the checklist and FAQ provided on this screen is for applicants applying to an ODJFSwaiver program. It will not provide you with a checklist or FAQ to apply to the Ohio Department ofAging (ODA).Select “New Application”.
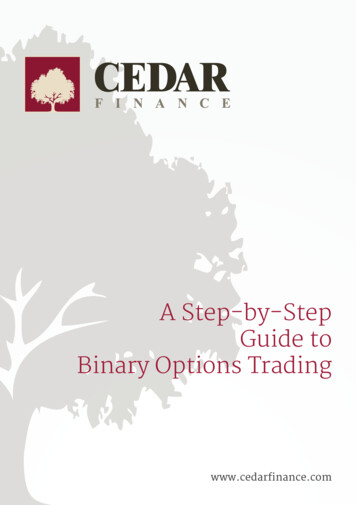
Enrollment Type: Select “Organization”.Action Request: will always be “Initial Enrollment”.Provider Type: “45 – Waivered Services OrganizationOR“74 – Home and Community Based ODA Assisted Living”Click “Next” to continue.
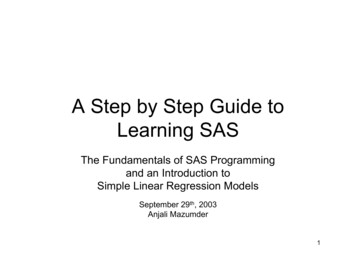
Enter all required fields where an asterisk (*) is located.Organization Legal Name: type the legal name of your business.Ownership Type: Select from the drop down box the option the best represents your business.Type: Select “FEIN” from the drop down box.SSN/FEIN: Type your Federal Tax ID number.OPTIONAL:If you are “doing business as” (DBA), please type your DBA in the field provided.No other information is required. Please leave all other fields blank.Click “Next” to continue.
IRS Tax Type: Select “FEIN”.IRS Tax ID: Type your Federal Tax ID number in the space.PLEASE NOTE: The system may not require you to answer the remaining fields. This would happen ifyou are reentering a second application or if you are currently a Medicaid Waiver Provider throughanother waiver program (e.g., ODJFS, DODD, etc).Complete your name, address, city and zip.Select date you are completing the MITS application as the IRS Effective Date.W-9 Form: Select “Yes”.All other fields remain blank.Click “Next” to continue.
Address Type: “Practice Location” is the default option. This is the address where you conduct yourbusiness.Enter all required fields where an asterisk (*) is located.Address Type Options:Please complete the required information for the following options by selecting “Add”.Home/Corporate OfficeMail To/CorrespondencePay ToAlt Practice LocationClick “Next” to continue.
Specialty: Select “480-ODA Waiver” from the drop down box for PASSPORT Waiver.Select “740-Home and Community Based Assisted Living” for the Assisted Living Waiver.Primary Specialty: Click the boxAll other fields remain blank.Click “Next” to continue.
You are not required to complete this screen.Click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
Type of Entity or Practice: Select the type of business (example: sole proprietor, corporation, etc).If other, specify the type of business in the field provided (example: LLC, etc).Click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
If your agency currently has a Medicaid Provider Number and are providing services through anotherstate agency (ODJFS, DODD, etc.), please select “Yes” and provide your Medicaid Provider Number in thefield.If you have more than one Medicaid Provider Number, select add and complete the step listed above.If no, click “Next” to continue.
If your agency is a corporation or LLC, select “Yes” and completed the required fields. If you have morethan one owner/director, select “Add” and repeat the process.If no, click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
Read the question and select the appropriate answer (yes or no). If yes, please complete the fields asrequested the click “Next” to continue.If no, click “Next” to continue.
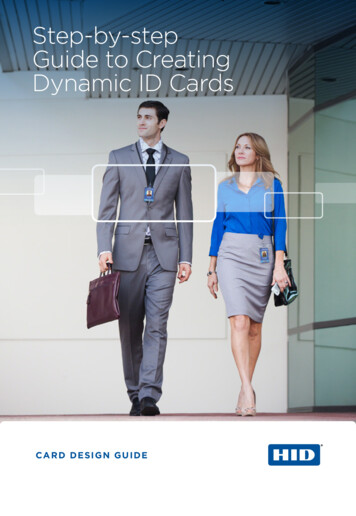
Enter all required fields wherean asterisk (*) is located.EMAIL ADDRESS: THIS FIELDMUST BE COMPLETED.Read thestatementand scrolldown prior toselecting “Iaccept theterms andconditions.Click “Next” to continue.PLEASE NOTE: You mustaccept all the terms andconditions on this page beforeyou can complete theapplication. If you do notagree to the terms andconditions, you will not beeligible to be certified as aMedicaid Waiver Provider.
Document Submission Type: Select “Mail” from the drop down box.No additional information is required. The space can be left blank.Click “Submit” to finalize you application in the MITS system.
These documents will beemailed to you by ODA.You have successfully completed your application in the MITS program.Your tracking number is displayed above. Be sure to write the ATN number down. You will be asked forthe ATN number if you call to check the status of your application.Signed Agreement & W-9 Form: ODA will email a copy of these documents when you are notifiedthrough email by our office. Both documents will need to be completed and signed. These documentswill be included when you return the required ODA application material. ODA will upload all requireddocumentation in MITS.You may print a copy of the application for your records by selecting “Print Application”.Click “Exit” to end the application process.
What to Expect:Within 10-15 business days, an email will be sent from ODA to the email address you provided on theapplication. Included in the email will be: Checklist indicating the additional documentation that is need for certification.Ohio Department of Aging Application for Certification as an Agency, Non-Agency or AssistedLiving Provider.Instruction for applicants seeking certification.A copy of the MITS Application.Blank W-9 form.All documentation must be completed and returned to ODA within thirty (30) business days.If you have any questions, please feel free to contact our office at 614-644-1737.Thank you for your interest in becoming a certified provider with the Ohio Department of Aging.
Select “Provider Enrollment Application” from the options listed on the right side of the screen. PLEASE NOTE: the checklist and FAQ provided on this screen is for applicants applying to an ODJFS waiver program. It will not provide you with a checkli