Transcription
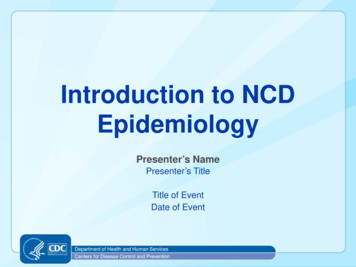
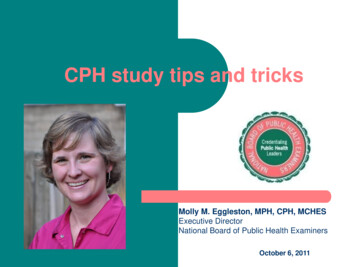
Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8–18www.elsevier.com / locate / jphotobiolThe epidemiology of UV induced skin cancer,abBruce K. Armstrong* , Anne KrickeraCancer Research and Registers Division, New South Wales Cancer Council, PO Box 572, Kings Cross 2011, AustraliabNational Breast Cancer Centre, Sydney, AustraliaReceived 8 August 2001; accepted 13 August 2001AbstractThere is persuasive evidence that each of the three main types of skin cancer, basal cell carcinoma (BCC), squamous cell carcinoma(SCC) and melanoma, is caused by sun exposure. The incidence rate of each is higher in fairer skinned, sun-sensitive rather than darkerskinned, less sun-sensitive people; risk increases with increasing ambient solar radiation; the highest densities are on the most sun exposedparts of the body and the lowest on the least exposed; and they are associated in individuals with total (mainly SCC), occupational (mainlySCC) and non-occupational or recreational sun exposure (mainly melanoma and BCC) and a history of sunburn and presence of benignsun damage in the skin. That UV radiation specifically causes these skin cancers depends on indirect inferences from the action spectrumof solar radiation for skin cancer from studies in animals and the action spectrum for dipyrimidine dimers and evidence that presumedcausative mutations for skin cancer arise most commonly at dipyrimidine sites. Sun protection is essential if skin cancer incidence is to bereduced. The epidemiological data suggest that in implementing sun protection an increase in intermittency of exposure should beavoided, that sun protection will have the greatest impact if achieved as early as possible in life and that it will probably have an impactlater in life, especially in those who had high childhood exposure to solar radiation. 2001 Elsevier Science B.V. All rights reserved.Keywords: Basal cell carcinoma; Squamous cell carcinoma; Cutaneous malignant melanoma; UVA; UVB1. IntroductionBy skin cancer we mean the three commonest types,basal cell (BCC) and squamous cell (SCC) carcinomas ofthe skin (also referred to, collectively, as nonmelanocyticskin cancer) and cutaneous malignant melanoma(melanoma).That UV radiation per se causes these cancers is mainlyan indirect inference from evidence that exposure to solarradiation, the main source of exposure to UV radiation, istheir main cause and the fact that only UV radiation candamage DNA directly. That solar radiation causes theseskin cancers is based on a substantial body of indirect anddirect epidemiological studies. These studies are stronglysupported by experimental evidence of the capacity of UVradiation to cause SCC and melanoma in animal models.There are no such models for BCC, although the presenceof UV ‘‘signature mutations’’ in the TP53 gene in a highproportion of BCCs [1] provides biological evidence tosupport the epidemiological observations.This paper summarises, the epidemiological evidence, as*Corresponding author. Tel.: 161-9-9334-1837; fax: 161-9-334-1778.E-mail address: brucea@nswcc.org.au (B.K. Armstrong).it now stands, that sun exposure causes skin cancer andthen briefly describes the basis on which a causal role forUV radiation can be inferred from a combination ofexperimental and epidemiological data. Finally, it describes the key implications of these data for prevention ofskin cancer by control of sun exposure.2. Epidemiological evidence that sun exposure causesskin cancer2.1. Relationship to ambient solar radiation2.1.1. Incidence by latitude or estimated ambient solarUVThe relationships between incidence rates of BCC andSCC in 1977–1978 and ambient solar UV across a latitudegradient are illustrated in Fig. 1 based on the data of Scottoet al. [2]. Rates increased with increasing estimatedambient solar UV (from Robertson-Berger meter observations of erythemal UV expressed as annual number ofmeter counts by 10 24 ) in ten US metropolitan populationsfrom 47.58 N (Seattle) to 30.08 N (New Orleans). Thevalues of R 2 for the exponential relationships plotted in1011-1344 / 01 / – see front matter 2001 Elsevier Science B.V. All rights reserved.PII: S1011-1344( 01 )00198-1
B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 189Fig. 1. Relationship of age-standardised incidence rates of BCC, SCC and melanoma (CMM) to estimated ambient erythemal UV radiation in ten USpopulations (Seattle, Minneapolis-St Paul, Detroit, Utah, San Francisco-Oakland, Atlanta, New Orleans, Albuquerque (New Mexico for melanoma)) in1977–1978 (BCC and SCC) and 1978–1982 (melanoma) [2,3].Fig. 1 are 0.81 for BCC in males, 0.80 for BCC in females,0.82 for SCC in males and 0.78 for SCC in females (R isthe coefficient of correlation between incidence and estimated ambient solar UV and takes values from 21 to 11,where 21 indicates a perfect negative correlation, 11indicates a perfect positive correlation and 0 indicates anabsence of any correlation, and R 2 is an estimate, in thiscase, of the proportion of variation in each incidence ratethat is explained by its association with ambient UV).While the incidence rates in the two sexes were quitedifferent, the slopes of the trends in incidence with ambientsolar UV were similar.By comparison, melanoma incidence rates showed amuch shallower trend with ambient solar UV, when rates in1978–1982 were added to Fig. 1 from Cancer Incidence inFive Continents (Vol. 5) [3] for nine of the ten populations.The R 2 -values were also very low: 0.02 in males and 0.07in females. However, a much more persuasive relationshipwas shown in data relating melanoma mortality in 1950–1967 to estimates of annual erythemal solar UV doseacross the ten provinces of Canada and the 48 continentalstates of the USA [4]. The R 2 -values were 0.44 for malesand 0.31 for females. In addition, Moan et al. [5] haveshown that the slope of the relationship across 30 populations of European origin in ten countries was much steeperif a measure of ambient solar UVA instead of erythemalUV (mainly UVB) was related to melanoma incidence.Inconsistencies have been observed in these patternsdepending on the populations studied, particularly formelanoma. They could be seen as arguing against arelationship of melanoma and solar UV at the geographicallevel. Alternatively, they may be explained by geographicgradients in ethnic mix of the population or the balance ofrecreational to occupational sun exposure [6].2.1.2. Personal residence history and effect of migrationThe effect of length of residence in an area of highambient solar radiation on risks of BCC, SCC andmelanoma is shown in Table 1. Here, length of residence isindicated by age at the beginning of residence in Australia,a high ambient solar radiation area. The three studies onwhich this and several other tables are based were chosenbecause they were all conducted in the same general area(Western Australia), used similar methods and recordedsimilar measurements. Risk of each type of skin cancerwas less in people who migrated to Australia after birththan in those who were born there, though risk was little ifat all less in those who migrated there in the first 10 yearsof life than in those born in Australia, while it was somethree-fold less in those who migrated after the first 10years of life. These results could suggest, simply, that riskof skin cancer increases with increasing length of residencein an environment with high ambient solar radiation, butthey have also been taken to suggest that exposure to solar
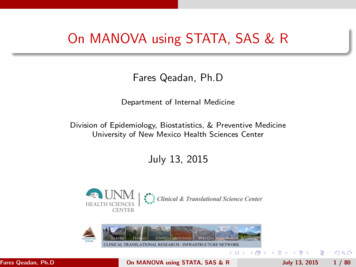
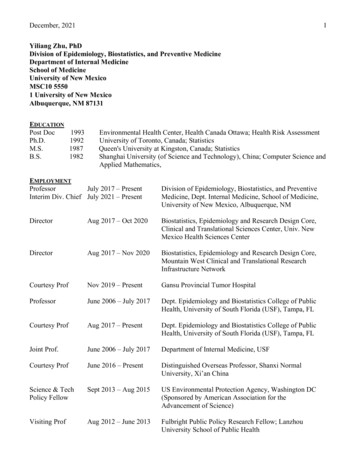
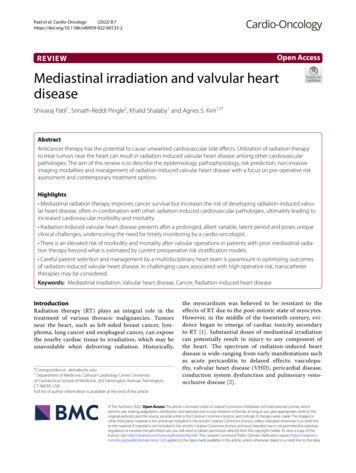
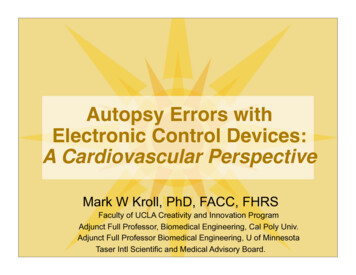
B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 1810Table 1Relationship of age at arrival in Australia, an area of higher ambient solarradiation than most of the areas from which the migrants came, with risksof BCC, SCC and melanoma [11,12,41]Age at arrivalin Australia(years)BCC aSCC 13)aThe relative risks of BCC and SCC are for migrants other than thoseof Southern European origin.bRelative risk estimates with 95% confidence intervals in brackets.radiation early in life may be particularly important inincreasing the risk of skin cancer [7].Risk also increased with increasing average annualhours of bright sunlight at all places of residence regardless of migration, but the gradients were generally not assteep as those seen with migration (Table 2). The gradientfor SCC appeared to be steeper than that for either BCC ormelanoma, which is consistent with the way rates varyacross geographic regions in relation to ambient solarradiation (Fig. 1). The rather weaker gradient for BCC,though, is not consistent, but nor is it precise. Lack of astrong correlation between bright sunlight hours andambient UV radiation could be a cause of inconsistency inthese patterns. However, the use of global solar radiationinstead of bright sunlight hours in studies of BCC and SCCdid not appear to produce any greater consistency [8,9].2.2. Relationship to cutaneous sun sensitivity2.2.1. Ethnic originThe best current comparisons of risk of skin cancer byethnic origin comes from population-based cancer incidence estimation or registration in multi-ethnic populationsin single environments. Rates of BCC, SCC and melanomaare compared between hispanic and non-hispanic whites inNew Mexico in Fig. 2. For each cancer in each sex, ratesin non-hispanic whites were 5–10 times higher than thosein the darker skinned hispanic whites. More detail is givenfor melanoma in Los Angeles County in Fig. 3. Again thedifferential in rates is 5–10-fold between non-hispanic andhispanic whites, and the rates in hispanic whites are twiceor more those in blacks and in people originating in China,The Philippines and Japan. The very low rates in theChinese population are notable and consistent with similarly low rates reported from China itself (0.3–0.4 in malesand 0.3 in females) and are not greatly less than those inthe Chinese in Singapore (0.6 in both males and females),who live on the equator. Chinese people generally havesubstantially lighter skin than do US blacks, thus, itappears that their very low incidence of melanoma is notsolely related to density of skin pigmentation.2.2.2. Color of unexposed skinRecent and comparable estimates of the associationbetween skin colour and risk of BCC, SCC and melanomaare shown in Table 3. The weakest evidence for anincrease in risk with increasing fairness of the skin is seenfor BCC and the strongest for melanoma. The apparentstrength of such associations, however, is influenced by theaccuracy of measurement of the ‘‘exposure’’ characteristic,in this case the colour of unexposed skin. Taking thedifference between light absorption at 420 and 400 nm isnow thought to be preferable to reflectance at 650 nm as anobjective measure [10]. Thus measurement error may havecontributed to the weaker association of skin colour withBCC.2.2.3. Propensity to sunburn and ability to tanTable 3 shows representative and comparable estimatesof trends in skin cancer risk with increasing sun sensitivity,as measured by decreasing ability to tan following repeatedexposure to the sun in summer. There was a substantialgradient to increasing risk with increasing sensitivity foreach of BCC, SCC and melanoma. The steepest gradientwas for SCC with a relative risk of 6.9 in people in themost sensitive group. All of these gradients were steeperthan the corresponding gradients in risk with decreasingskin colour.Confounding with sun sensitivity, or whatever thecomplex of inherited characteristics is that mediates it, isTable 2Relationships of average annual daily hours of bright sunlight averaged or accumulated over all places of residence in people born in Australia with risks ofBCC, SCC and melanoma [41,8,9]Hours of bright sunlight aBCCSCCMelanoma bFirst quarterSecond quarterThird quarterFourth 7–12)1.001.34(0.96–1.86)c1.92(1.16–3.18)aFor melanoma, the measure was average annual hours of bright sunlight at all places of residence, for BCC and SCC it was accumulated hours ofbright sunlight at all places of residence.bAccumulated hours of bright sunlight was categorised into thirds for the analysis of melanoma.cRelative risk estimates with 95% confidence intervals in brackets.
B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 1811Fig. 2. Relationship of age-standardised incidence rates of BCC, SCC and melanoma (CMM) to ethnic origin in New Mexico, USA, in 1977–1978 (BCCand SCC) and 1978–1982 (melanoma) [2,3].Fig. 3. Relationship of age-standardised incidence rates of melanoma to ethnic origin in Los Angeles County, USA, in 1988–1992 [38]. (The SanFrancisco Bay Area rates were used for the Chinese population because the Chinese population of that area was appreciably larger and gave non-zerorates).
12B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 18Table 3Relationships of colour of unexposed skin and ability to tan with risks of BCC, SCC and melanoma [13,11,12]Colour of unexposed skinDarkest quarterSecond quarterThird quarterLightest quarterBCC aSCC 1–1.9)2.3(1.6–3.3)3.5(1.8–6.8)bAbility to tanDeep tanModerate tanLight tanNo tanaEstimate for BCC adjusted for age, sex, age at arrival in Australia and Southern European ethnicity, estimate for SCC based on subjects not of SouthernEuropean origin and adjusted for age, sex and year at interview.bRelative risk estimates with 95% confidence intervals in brackets.cSkin colour of melanoma cases and controls was measured by comparison with a grey scale viewed through monochromatic filters; for BCC and SCCit was measured by reflectometry at 650 nm.usually regarded as explaining the relationship of pigmentary variables with skin cancers. When sun sensitivity andskin colour were analysed in a single logistic regressionmodel with hair colour and eye colour, only the ability totan remained a significant predictor of risk for BCC [11],and ability to tan and tendency to sunburn for SCC [12].Skin reaction to sun exposure was a strong independentpredictor of risk for melanoma in Western Australia [13]and appeared to explain the effect of skin colour and eyecolour but not hair colour.2.3. Distribution on the bodyRecent data on the relative density of incident BCC,SCC and melanoma in Queensland, Australia, are shownseparately for males and females in Fig. 4. Broadlyspeaking, relative body density of all three cancers washigh on the face and neck, which are more-or-less continually exposed when outdoors, and very low on the scalp inwomen and the buttocks in both sexes, which are rarelyexposed. It was also low on the chest, abdomen and thighs,which are generally little exposed. Outside this broadgeneralisation, there are some interesting differences in thepatterns. SCC stands out with a substantially higherdensity on the backs of the hands than either BCC ormelanoma. These two, however, had similar and quite highdensities on the shoulders and back, whereas SCC had alow density on these sites.Comparing males and females there are also somenotable differences. Density of all three cancers wasgreater on the scalp in men than women, which mightreasonably be attributed to loss of hair in men giving riseto increased exposure of the scalp to solar radiation. Thesame is true when the density on the ears is estimatedseparately from that on the face (data not shown). Densityof SCC and, to a lesser extent, melanoma was higher onthe arms and lower legs in women than it was in men,which may reflect a higher exposure of these sites to thesun in women than men.These data are then consistent with an effect of sunexposure on risk of all three cancers given the highdensities on the usually exposed face and ears and the lowdensities on the rarely exposed sites. That this effect is notthe same for all three cancers, however, is suggested by thedifferences in density on the frequently but intermittentlyexposed shoulders and back where the density of SCC islow and the densities of BCC and melanoma are moderateand similar. As noted above, the site distribution ofmelanoma has been taken to suggest an effect of pattern ofsun exposure on its incidence, and the somewhat similardistribution of BCC may indicate a similar effect. Equally,however, it may be a simple dose effect for BCC given itsextreme density on the face. The near absence of BCC andmelanoma from the backs of the hands has generally beenassumed to be due to the nature of the skin rather than tocomplex effects of sun exposure.2.4. Relationship to personal exposure to the sunBecause of the evidence that melanoma and possiblyalso BCC are related to pattern as well as amount of sunexposure, personal sun exposure is now usually represented in three ways: total exposure, occupational exposure(the archetypal example of a more continuous pattern ofexposure) and non-occupational or recreational exposure(‘‘intermittent’’ exposure). In addition, history of sunburnis usually recorded in studies of skin cancer; sunburn isgenerally thought to be an indicator of high levels ofintermittent sun exposure. Each of these may be estimatedover the whole or a part of life. When sun exposure occursin life may also be important [7], but only estimates oflifetime exposure will be considered here.Our present, best understanding of the relationshipbetween the different types of personal sun exposure and
B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 1813Fig. 4. Relative density (the density on a particular site relative to the density on the body as a whole) of BCC, SCC and melanoma (CMM) on differentbody sites in Queensland, Australia (prepared from data of Green et al. [39] and Buettner and Raasch [40]).risk of BCC, SCC and melanoma is summarised in Table4. This table is based on an overview (metanalysis) ofpublished studies of melanoma prepared by Elwood andJopson [14] and a similar overview, which we haveprepared, of published studies of BCC and SCC. In eachcase, the result used in the overview analysis was thepublished relative risk (odds ratio) for the highest categoryof exposure documented compared to the reference groupchosen by the authors, which was the lowest exposurecategory in all cases. Where there was a choice of variable
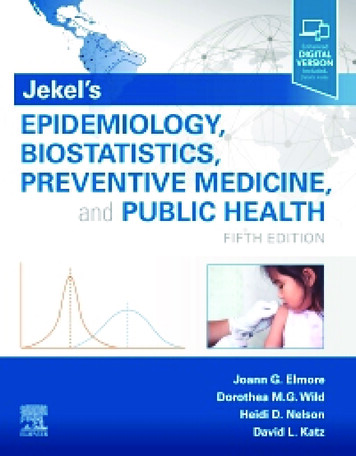
B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 1814Table 4Relationships of personal sun exposure with risks of BCC, SCC and melanoma [14]Type of exposureTotalOccupationalNon–occupational or ‘‘intermittent’’Sunburn at any ageabBCC 4)1.40(1.29–1.51)bSCC s for BCC and SCC are from an unpublished overview of published studies (see text).Relative risk estimates with 95% confidence intervals in brackets.for any exposure type, priority for selection was given tovariables that represented the nearest to lifetime exposureof that type. For non-occupational or intermittent exposure,the variable likely to represent the most clearly intermittenttype of exposure was also sought. Only results that wereadjusted for age and sex were used (a number of the earlystudies of BCC and SCC did not make this adjustment)and results that were also adjusted for some measure ofsun sensitivity were chosen where there was a choice.While none of the associations illustrated in Table 4 arevery strong, possibly because of the difficulty people havein recalling past sun exposure accurately and a lack ofspecificity of measurements for the site of the skin cancerin most studies, they do show a coherent pattern that isconsistent with present thinking on differences in the waysin which BCC, SCC and melanoma are related to sunexposure.First, only SCC is at all strongly related to estimatedtotal sun exposure (RR51.53, 95%; CI50.02–2.27). Thelimited data indicate a weak relationship of total sunexposure with melanoma. While there is little evidence forsuch a relationship with BCC, the wide confidence intervalindicates that it could be at least as strong as that withmelanoma.Second, only SCC shows a strong relationship withoccupational sun exposure (RR51.64, 95%; CI51.26–2.13). There is a weak, but significant association of BCCwith occupational exposure (RR51.19) but, if anything,the association of melanoma with it is inverse (RR50.86,95%; CI50.77–0.96). While the latter observation mightbe taken to suggest that risk of melanoma is reduced byoccupational sun exposure, to do so would be wrong giventhe data on which it is based. The reference, low-occupational exposure groups with which the high exposuregroups have been compared have probably contained, inmost if not all cases, some people with higher levels ofrecreational sun exposure. Thus, the lower than baselinerisk of melanoma in people with high occupational exposure probably reflects simply the association of melanomawith high levels of recreational or intermittent exposure.Third, both BCC (RR51.38) and melanoma (RR51.71)show significant associations with non-occupational (intermittent) sun exposure, while SCC shows no such association (RR50.91). There is, however, no overlap betweenthe 95% confidence intervals about the relative risks forBCC and melanoma, thus, suggesting that melanoma ismore strongly related to intermittent exposure than is BCC.A similar pattern is seen for sunburn except that SCCshows a weak positive, but not statistically significant,association with sunburn. The patterns for BCC andmelanoma can reasonably be taken to support previousinferences that a history of sunburn generally reflects anintermittent pattern of sun exposure. A weak association,such as that seen for SCC, could be due to residualconfounding between sun sensitivity and sunburn.2.5. Association with benign sun-related conditionsAssociations of benign sun-related conditions with BCC,SCC and melanoma are compared in Table 5.Cutaneous microtopography was used in the WesternAustralian studies as a semi-objective measure of sundamage to the skin of the backs of the hands. In principle,it is a reasonably accurate measure of total sun exposure tothese body sites, but it is not highly correlated withhistopathological assessment of grade of solar elastosis[15]. Risk of each type of skin cancer was higher inhigher-graded categories of microtopography. While SCCappeared less strongly related to microtopography gradethan BCC and melanoma, the baseline category used forthis assessment was grades 1–4 instead of 1–3 as used forTable 5Relationships of benign sun-related conditions with risks of BCC, SCCand melanoma aBCCGrade of cutaneous �6.4)63.1(1.5–6.4)SCC1.00 �2. 8)1.8(1.0–3.2)2.7(1.4–5.0)Freckling as a childYes cf. no1.8(1.2–1.5)1.6(1.0–2.4)1.5(1.2–1.9)Solar keratosesSome cf. lanocytic naeviSome cf. rces of results: cutaneous microtopography [41]; freckling[16,17]; solar keratoses [11,18]; melanocytic naevi [11].bFirst category for SCC is grades 1–4, no, mild or moderate damage.cRelative risk estimates with 95% confidence intervals in brackets.
B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 18BCC and melanoma; thus, the evidence for a difference isweak.BCC, SCC and melanoma were equally strongly associated with a history of freckling on the face as a child,based on the results of studies conducted by use ofcommon methods and near simultaneously in WesternCanada [16,17]. Freckling is almost certainly determinedby genetic factors as well as sun exposure and these resultscould indicate that either or both of these factors arerelated to all three types of skin cancer.Presence of solar keratoses, as assessed by dermatologists, on most of the body [11] or just on the left forearmand the face [18], were also associated with all three typesof cancer; thus, suggesting that all are related to totalaccumulated sun exposure. SCC was much more stronglyassociated with solar keratoses than were BCC andmelanoma. In addition to sun exposure being a cause ofboth solar keratoses and SCC, this may be because a solarkeratosis directly precedes some 60% of SCCs [19]. Theweaker association of melanoma with solar keratoses thanBCC should not be over-interpreted because of the difference between the body sites on which the solar keratoseswere measured in the two studies compared; 45% ofsubjects were in the reference ‘‘none’’ category in thestudy of BCC and 64% in the study of melanoma.A similar pattern is seen for the associations withmelanocytic naevi (moles) as for solar keratoses exceptthat the strong association was with melanoma, for whichmelanocytic naevi are precursors, and there was no evidence of an association of melanocytic naevi with BCC orSCC. While there is substantial evidence that melanocyticnaevi are caused by sun exposure [20], as well as beingstrongly genetically determined [21], they probably onlyreflect sun exposure in childhood. This, together with theirstrong genetic determination, may make their presenceinsufficiently predictive of the sun exposure needed toproduce BCC and SCC to be a surrogate measure of it.2.6. Effect of reduction in sun exposure2.6.1. Population sun exposureThere are no data available on long-term trends in sunexposure in any population. It is difficult, therefore, todraw any certain conclusions about effects of changes insun exposure from analysis of trends in incidence of skincancer. There are, however, a few suggestions that recentbut poorly documented down trends in sun exposure mayhave reduced risk of melanoma and BCC, but not SCC.We have observed down trends in melanoma incidencein New South Wales, Australia, in women 15–49 years ofage and men 15–34 years of age over the period 1983–1996, which are consistent with a falling incidence inpeople born since about 1950, particularly women [22].Similar trends have been reported from some other populations, mainly in North America and New Zealand. Therehas been substantial public education in Australia over the15past 20 years regarding the need to reduce sun exposure toprotect against skin cancer, and a number of surveyssuggest that falls in exposure have followed this education.The falls in incidence of melanoma in younger people inNew South Wales are consistent with greater benefit orearlier effects from exposure reduction earlier than later inlife and the greater fall in women than men is consistentwith greater efficacy of sun protection education inwomen.A near identical pattern of trends in incidence of BCC inAustralia as a whole has been observed between surveysdone in 1985 and 1995 [23] with a fall in rate of BCC inpeople under 50 years of age, which was greater in theyounger than the older age groups in this range andappears to have been greater in women than in men. Therewas no similar trend in incidence of SCC, which could bea consequence of the differences in the relationship of sunexposure to SCC and BCC and melanoma summarised inTable 5.2.6.2. Personal sun protectionA number of case-control studies have examined therelationship between sun protection measures, includinguse of hats, clothing and sunscreen, and risk of BCC, SCCand melanoma. There results, however, are unreliablebecause of the great difficulty of controlling negativeconfounding between sun protection and sun sensitivityand sun exposure.One observational study only, of BCC, might be takenas indicative of a probable effect of sun protectionmeasures in reducing risk. Robinson and Rademaker [24]randomised 61 patients with a past history of two or morebiopsy proven BCCs to receive either 10 mg a day ofisotretinoin or placebo. All patients were also given writtenrecommendations on sun protection. They had follow-upskin examinations at 6, 12, 18 and 36 months and allclinically suspicious lesions were surgically removed. Atthe end of the study, all patients completed a questionnaireregarding their sun exposure. Thirty-five patients wereclassified into a high exposure group and 26 into a lowexposure group — people who had changed theirsunscreen use since developing a cancer tended to use anSPF 151 sunscreen and limited their outdoor activities.Those with low sun exposure had, on average, one lessBCC before entry to the study than those with high sunexposure (2.5 cf. 3.5). In the first 18 months of the studythey had an average of 0.2 BCCs compared with 3.0 in thehigh exposure group and 1.4 compared with 5.5 in thesecond 18 months. The level of sun exposure significantlypredicted the number of new BCCs (P50.02) independently of number of previous BCCs. While these resultssuggest a short-latency effect of sun exposure reduction onrisk of BCC, a randomised controlled trial of dailysunscreen use in a general population sample in Queensland, Australia, showed no effect on risk of BCC over 4–5years of intervention and follow-up [25] (see below).
16B.K. Armstrong, A. Kricker / Journal of Photochemistry and Photobiology B: Biology 63 (2001) 8 – 18There are two lines of evidence suggesting that reduction in sun exposure by daily use of a sunscreen mayreduce risk of SCC. First, two randomised controlled trialshave shown that daily use over 6 months (one summer) to2 years (SPF 17 and 29, respectively) can reduce the rateo
an indirect inference from evidence that exposure to solar 2. Epidemiological evidence that sun exposure causes radiation, the main source of exposure to UV radiation, is skin cancer their main cause and the fact that only UV radiation can damage DNA directly. That solar radiation causes these 2.1. Relationship to ambient solar radiation