Transcription
The Clinical Presentation of Psychotic DisordersBob Boland MDSlide 1Psychotic DisordersSlide 2Archetype SchizophreniaSlide 3Phenomenology The mental status udgment and InsightAs with all the disorders, it is preferable to pickone “archetypal” disorder for the category ofdisorder, understand it well, and then know theothers as they compare. For the psychoticdisorders, the diagnosis we will concentrate onwill be Schizophrenia.A good way to organize discussions ofphenomenology is by using the same structureas the mental status examination.
Clinical Presentation of Psychotic Disorders.Slide 4Appearance– Motor disturbances Catatonia Stereotypy Mannerisms– Behavioral problems Hygiene Social functioning– “Soft signs”Slide 5Appearance Behavioral Problems Social functioning Other– Ex. Neuro soft signsSlide 6Mood and Affect– Affective flattening– Anhedonia– Inappropriate AffectMotor disturbances include disorders ofmobility, activity and volition. Catatonicstupor is a state in which patients areimmobile, mute, yet conscious. They exhibitwaxy flexibility, or assumption of bizarrepostures as most dramatic example. Catatonicexcitement is uncontrolled and aimless motoractivity. It is important to differentiate fromsubstance-induced movement disorders, suchas extrapyramidal symptoms and tardivedyskinesia.Disorders of behavior may involvedeterioration of social functioning-- socialwithdrawal, self neglect, neglect ofenvironment (deterioration of housing, etc.), orsocially inappropriate behaviors (talking tothemselves in public, obscene language,exposing self). Substance abuse is anotherdisorder of behavior. Patients may abusecigarettes, alcohol or other substances;substance abuse is associated with poortreatment compliance, and may be a form of"self-medication" for negative symptoms ormedication effects.Disorders of mood and affect includeaffective flattening, which is a reducedintensity of emotional expression and responsethat leaves patients indifferent and apathetic.Typically, one sees unchanging facialexpression, decreased spontaneous movements,poverty of expressive gestures, poor eyecontact, lack of vocal inflections, and slowedspeech. Anhedonia, or the inability toexperience pleasure, is also common, as isemotional emptiness. Patients may also exhibitinappropriate affect. Depression may occur inas many as 60% of schizophrenics. It isdifficult to diagnose, as it overlaps with(negative) symptoms of schizophrenia andmedication side effects.Page 2 of 17
Clinical Presentation of Psychotic Disorders.Slide 7Thought– Thought Process– ContentSlide 8Thought Process– Associative disorders– CircumstantialThinking– Tangential thinkingThought disorders can be divided into differenttypes. Most commonly they are divided intodisorders of "process" or of "content".Disorders of thought process involve adisturbance in the way one formulates thought:the process by which we come up with ourthoughts. Thought disorders are inferred fromspeech, and often referred to as "disorganizedspeech." Historically, thought disordersincluded associative loosening, illogicalthinking, over inclusive thinking, and loss ofability to engage in abstract thinking.Associative loosening includes circumstantialthought and tangential thought.Page 3 of 17
Clinical Presentation of Psychotic Disorders.Slide 9Other associative problems smsThought ContentOther types of formal thought disorder havebeen identified, including perseveration,distractibility, clanging, neologisms, echolalia,and blocking. With the possible exception ofclanging in mania, none appears to be specificto a particular disorder.Disorders of Thought Content includehallucinations and delusions. Hallucinations DelusionsSlide11Hallucinations Definition Typical typesHallucinations are perceptions withoutexternal stimuli. They are most commonlyauditory, but may be any type. Auditoryhallucinations are commonly voices, mumbledor distinct. Visual hallucinations can be simpleor complex, in or outside field of vision (ex. "inhead") and are usually normal color. Olfactoryand gustatory are usually together--unpleasanttaste and smell. Tactile or haptic hallucinationsinclude any sensation--electrical, or the feelingof bugs on skin (formication). These arecommon across all cultures and backgrounds;however, culture may influence contentPage 4 of 17
Clinical Presentation of Psychotic Disorders.Slide12DelusionsDelusions are fixed, false beliefs, notamendable by logic or experience. There are avariety of types. Delusions are mostcommonly persecutory, but may be somatic,grandiose, religious or nihilistic. They areinfluenced by culture, and none is specific toany one disorder (such as schizophrenia).(The cartoon is an example of a delusion ofreference: that something that is independentof you is in fact intended for you. WE oftenget at these by asking patients whether thetelevision or radio seems to be sending themmessages.)Slide13Comparing types of ThoughDisorders:Slide14Cognitions Subtle impairments– Frontal lobe function Associative thinking2 video examples demonstrating first a disorderof thought process, and then one of content.Among other disorders of cognition is lack ofinsight. Truly psychotic persons have abreakdown in this ability to rationally critiquetheir own thoughts. This may best distinguishpsychotic disorders (like Schizophrenia) from"normal" hallucinations and delusions.Other cognitive symptoms are usually normal(for example, orientation and memory).However, IQ usually is less than normalpopulation for their age; it does not tend todecline over time. And there appear to besubtle cognitive deficits in persons withpsychotic disorders. For example for yearsinvestigators have noticed deficits frontal tasks(see Dr. Malloy’s lecture on frontal lobes) suchas difficulties with pattern recognition.Page 5 of 17
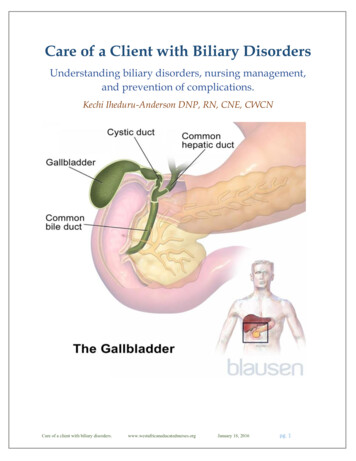
Clinical Presentation of Psychotic Disorders.Slide15For example, Sorkin and colleagues created avirtual maze. The maze consists of a series ofrooms, each of which included three doors.Each door was characterized by three features(color, shape, and sound), and a singlecombination of features-the door-opening rulewas correct. Subjects had to learn the rule anduse it. In that sense, its like a virtual Wisconsincard sort.They studies the maze with 39 schizophrenicpatients and 21 healthy comparison subjects.They found that by taking into account variouserror scores, response times, navigation abilityand overall strategy they could correctlypredict 85% of the schizophrenic patients andall of the comparison subjects.Sorkin A, et al, American Journal ofPsychiatry. 163(3):512-520, 2006.Page 6 of 17
Clinical Presentation of Psychotic Disorders.Slide16Positive versus Negative Sxs Positive– Hallucinations– DelusionsSlide17Negative Symptoms AlogiaAffective flatteningAnhedoniaAvolition/apathyIt is important to differentiate positivesymptoms of schizophrenia from negativesymptoms. Positive symptoms are disordersof commission, including things patients do orthink. Examples are hallucinations, delusions,marked positive formal thought disorder(manifested by marked incoherence,derailment, tangentiality, or illogicality), andbizarre or disorganized behavior.Negative symptoms are disorders of omission:things patients don't do. Negative symptomsinclude alogia (i.e., marked poverty of speech,or poverty of content of speech), affectiveflattening, anhedonia or asociality (i.e.,inability to experience pleasure, few socialcontacts), avolition or apathy (i.e., anergia, lackof persistence at work or school), andattentional impairment. The relevance of thesesymptoms is unclear. Perhaps they representindependent subtypes of schizophrenia?Probably not. Different stages of disease?Maybe--positive symptoms tend to occur earlyon, negative symptoms later. Most patientshave a mix of symptoms.Page 7 of 17
Clinical Presentation of Psychotic Disorders.Slide18Epidemiology 1% prevalence Genders SocioeconomicThere is an overall 0.7% incidence of "NonaffectivePsychosis" in the National Comorbidity Study. Thisstudy included schizophrenia, schizophreniformdisorder, schizoaffective disorder, delusional disorderand atypical psychosis.Schizophrenia has about 1% lifetime prevalence inECA studies. There is a lower incidence (chronicdisorder): 1/10,000/year. Incidence is equal acrossgender, but men may get it earlier. It most commonlystarts in late adolescence/early adulthood. It rarelyoccurs in children. Women are more likely to get lateonset. Generally, this version tends to have betterpsychosocial functioning. Schizophrenia occursthroughout the world, regardless of site or culture.Schizophreniform Disorder has a lifetime prevalenceof 0.2%, with 1-year prevalence of 0.1%. Otherwise, itis similar in epidemiology to Schizophrenia.Schizoaffective Disorder is probably less commonthan Schizophrenia. There is little data about thecommunity prevalence of Delusional Disorders.However, lifetime prevalence appears to be 0.03%.Clinical studies show delusional disorder to be 1-2% ofinpatient psychiatric admissions.Brief Psychotic Disorder and Shared PsychoticDisorder also have little information and are probablyrare. Shared Psychotic Disorder may go unrecognized inclinical settings; it is also probably more common inwomen.Psychotic Disorder Due to a General MedicalCondition, and Substance-Induced PsychoticDisorder are both probably common, particularly inclinical settings.Page 8 of 17
Clinical Presentation of Psychotic Disorders.Slide19DiagnosisSlide20Diagnosis Schizophrenia: DSM-IV “A” Criteria– Psychosis Duration– 6 months Global CriteriaPatients have to have been psychotic at sometime. This is referred to as the “A” Criteria ofSchizophrenia, as they are listed under the “A”outline heading in DSM-IV. The next slidewill cover these, but it basically serves as a listof possible psychotic symptoms.There is also a time criteria. The acutesymptoms must persist for 1 month (less iftreated). And the overall duration of thedisorder must be at least 6 months: that, is thepatient must show some signs of disturbance(psychotic episode prodromal or residualsymptoms) for at least 6 months.The Global Criteria. This is my term, not anofficial one. It simply reflects almost everydisorder in DSM-IV includes a criteria sayingthat the disorder has to impair the individuallyin some way. Psychiatrists don’t just treatpeople because they seem “weird” orunusual—they must have some sort of social oroccupational dysfunction as a result of thedisease.Page 9 of 17
Clinical Presentation of Psychotic Disorders.Slide21Diagnosis “A Criteria”– Two or more: DelusionsHallucinationsDisorganized speechDisorganized behaviorNegative symptomsThe "A" Criteria of Schizophrenia basicallysays that, to have schizophrenia, you have tohave been psychotic at some point. Theydefine psychosis as having one of the followingsymptoms:delusions, hallucinations, disorganizedspeech, disorganized behavior/catatonia, andnegative symptomsYou have to have had at least 2 of thesesymptoms to meet the criteria. Or, if you havereally bad hallucinations or delusions, that’sgood enough.Slide22Schizophrenia Subtypes Catatonic– Movement Disorganized– ProcessThere are certain subtypes of the disorder aswell. The purpose of subtyping is to improveprediction of likely effective treatment and/orcourse of illness.The types are listed as follows: Paranoid– Content Undifferentiated ResidualParanoid subtype: a preoccupation withone or more delusions or frequent auditoryhallucinations; disorganized speech/behavior,catatonic behavior, and flat or inappropriateaffect are not prominent.Disorganized subtype: characterized bydisorganized speech and behavior, and flat orinappropriate affect; it does not meet thecriteria for catatonic schizophrenia.Catatonic subtype: dominated by at least twoof the following: motoric immobility asevidenced by catalepsy or stupor, excessivemotor activity, extreme negativism or mutism,peculiarities of voluntary movement (e.g.,stereotypies, mannerisms, grimacing) andecholalia or echopraxia.Undifferentiated subtype: which is aresidual category for patients meeting criteriafor schizophrenia but not meeting criteria forthe paranoid, disorganized, or catatonicsubtypes.The residual subtype: as described in DSMIV is used for patients who no longer haveprominent psychotic symptoms but who oncePage 10 of 17
Clinical Presentation of Psychotic Disorders.met criteria for schizophrenia and havecontinuing evidence of illness.Slide23Other Diagnosis SchizophreniformSchizoaffectiveBrief PsychoticDelusional DisordersShared PsychosesPsychosis due to something’ elseSchizophrenia is the most common psychotic disorder. (that may notbe exactly true: “secondary psychotic disorders”, that is, psychoticdisorders caused by drugs or medical disorders are probably morecommon, but they are rarely studied, so we know less about them).However, there are other psychotic disorders, and these should bedifferentiated from schizophrenia:Schizophreniform disorder is like Schizophrenia except the duration isbetween 1 and 6 months (prodrome episode residual). If theduration is less than 1 month it is Brief Psychotic Disorder. Impairedpsychosocial functioning is not required for the diagnosis; probablyabout 2/3 go on to become Schizophrenics.Schizoaffective Disorder has symptoms of both Schizophrenia and of aMood Episode:. It fulfills symptoms of "Criterion A" ofSchizophrenia. For diagnosis, at some point, psychotic symptoms haveto be independent of mood (for at least 2 weeks). Symptoms of aMood Episode may include either manic, depressed or mixedsymptoms. These have to occur for a "substantial" amount of time;otherwise patient might be a depressed schizophrenic.Delusional Disorder is a disorder in which patients present withpersistent delusions. Delusions are nonbizarre, thus differentiat
Schizophrenia, as they are listed under the “A” outline heading in DSM-IV. The next slide will cover these, but it basically serves as a list of possible psychotic symptoms. There is also a time criteria. The acute symptoms must persist for 1 month (less if treated). And the overall duration of the disorder must be at least 6 months: that, is the patient must show some signs of disturbance .