Transcription
Nelson, J. Post-COVID OpsoclonusJodi Nelson D.O.aGregory Blume M.D.aSaurabh Bansal M.D.cJacqueline Kaufman APNbFlorence Woods, APNbXiaojun Zhang, M.D.aJorge Kattah, M.D.aatedPOST-INFECTIOUS SARS CoV-2 OPSOCLONUS MYOCLONUS ATAXIASYNDROMEAccepDepartment of Neurology, University of Illinois College of Medicine Peoria, IllinoisNeurologic Institute. OSF St. Francis Medical Center, Peoria, IllinoisbDepartment of Neurology, Illinois Neurologic Institute OSF St. Francis Medical Center, Peoria,IllinoiscDepartment of Internal Medicine, University of Illinois College of Medicine Peoria, OSF St.Francis Medical Center, Peoria, IllinoisCorresponding Author:Jorge C Kattah, M.D.Department of Neurology, University of Illinois College of Medicine Peoria, St. Francis MedicalCenter. 530 NE Glen Oak Ave, Peoria, IL, USA 61637Telephone: 309-655-2702, FAX 309-655-2040Email: kattahj@uic.eduAcknowledgement: The authors thank Professor Davis S Zee, M.D., who provided updatedreferences on the pathogenic mechanisms of opsoclonus.None of the authors has a Conflict of Interest.There was no funding support for this study1
Nelson, J. Post-COVID OpsoclonusAbstracttedBackground: The opsoclonus-myoclonus-ataxia syndrome (OMAS) represents both apathophysiology and a diagnostic challenge. Even though the diverse etiologies likely share acommon mechanism to generate the ocular, trunk and limb movements, the underlying causemay be a paraneoplastic syndrome, as the first sign of cancer, or may be a post-infectiouscomplication and thus, outcome depends on identifying the trigger mechanism. A recenthypothesis suggests increased GABAA receptor sensitivity in the olivary-ocular motor vermis(OMV)-fastigial nucleus (FN) - premotor saccade burst neuron circuit in the brainstem. Themanagement therefore, will focus on immunosuppression and modulation of GABA Ahypersensitivity with benzodiazepines.Methods: We serially video recorded the eye movements at the bedside of one patient withSARS-Cov-2 IgG serum antibodies, but twice-negative nasopharyngeal reverse transcriptasepolymerase chain reaction (RT-PCR). We tested cerebrospinal fluid (CSF), serum, andnasopharyngeal samples. In addition to an MRI brain and CT chest-abdomen pelvis. We treatedour patient with clonazepam and high-dose solumedrol, followed by a rituximab infusion afterher formal eye movement analysis 10 days later.AccepResults: The recordings throughout her acute illness demonstrated different eye movementabnormalities. While on high-dose steroids and clonazepam, she had initially macrosaccadicoscillations (MSO), followed the next day by brief ocular flutter during convergence; ten dayslater she had bursts of opsoclonus during scotopic conditions with fixation block with otherwisenormal eye movements. Concern for a suboptimal response to high-dose Solumedrol motivatedan infusion of Rituximab, which induced remission. An investigation for a paraneoplasticetiology was negative. CSF testing showed elevated neuron specific enolase. Serum IgG toSARS-CoV2 was elevated with negative reverse transcriptase polymerase change reaction (RTPCR) nasopharyngeal testing.Conclusion: A recent simulation model of macro-saccadic oscillations, and OMAS, proposescombined brainstem/cerebellar pathology due to increased GABA A receptor sensitivity. Here, wereport one patient with elevated CSF NSE, macro-saccadic oscillations, ocular flutter and OMASas a SARS-CoV2 post-infectious complication. Opsoclonus emerged predominantly withfixation block and suppressed with fixation, providing support to modern theories on themechanism responsible for these ocular oscillations involving cerebellar-brainstem pathogenesis.2
Nelson, J. Post-COVID OpsoclonusIntroduction:tedThe opsoclonus-myoclonus-ataxia syndrome (OMAS) is the result of diverse etiologies with acommon mechanism responsible for the ocular, trunk and limb movements. The underlyingcause may be a paraneoplastic syndrome, as the first sign of cancer, or may be a postinfectious complication [1-4]. A recent hypothesis suggests increased GABA A receptor sensitivityin the olivary-ocular motor vermis (OMV)-fastigial nucleus (FN) - premotor saccade burst neuroncircuit in the brainstem[5]. The management therefore, will focus on immunosuppression,search for a possible underlying malignancy or infectious etiology and modulation of GABAAhypersensitivity with benzodiazepines.AccepCaseA 57-year old female without significant past medical history presented with a day of speechchanges and persistent jerking movements in late February 2021. Of note, her son and husbandhad SARS CoV-2 pneumonia with positive SARS CoV-2 nasopharyngeal RT-PCR test obtainedat the local city public testing facility and performed at our Institution in January 2021, after afamily trip to Georgia. On 2/1, she had a negative SARS CoV-2 nasopharyngeal RT-PCR test.No family history of ataxia or abnormal movements. Review of systems was negative for nightsweats, unintentional weight loss, fevers, rashes, respiratory complaints, or change in olfaction ortaste. Her recent mammogram was normal.On examination, she had a non-rhythmic truncal titubation (Video 1), hyperekplexia, pronouncedlimb and truncal ataxia, intention tremor and dysdiadochokinesis. Cranial nerves, strength,sensation to pinprick, vibration, and proprioception were intact with symmetric deep tendonreflexes without pathologic reflexes. On hospital day 4, before steroids were started, her MOCAscore was 25/30 (-3 delayed recall, -1 for copying, -1 floor of the hospital). Her eye examshowed unsteady visual fixation with macrosaccadic oscillations (Video 2 Section 1), recordedthe day after her first dose of 1 G of intravenous Methylprednisolone (i.v. MP) andconvergence-induced brief ocular flutter (Video 3) recorded the following day, after two days of1 G, i.v. MP.CSF testing: Clear, colorless fluid with 1 nucleated cell and 1 red blood cell, normal protein(35.5 mg/dL) and glucose (57 ng/dL). Her CSF NSE was elevated at 34 ng/dL (normal 15ng/dL). Gram stain was negative for organisms. Cytology was negative for malignancy. Flowcytometry was negative for abnormal lymphoid population. AMPA-A, Amphyphysin, Anti-glialnuclear, anti-neuronal nuclear type 1-3, CASPR 2 IgG, CRMP-5, DPPX, GABA-B-R, GAD65,GFAP, glycine R, IgLON5, LGI1 IgG, mGlur1, NIF, NMDAR, and Purkinje cell cytoplasmicantibodies were negative (Mayo Clinic Laboratory). Oligoclonal bands were absent.On admission, she had a second negative SARS CoV-2 nasopharyngeal RT-PCR test, but shehad positive serum testing: IgG to SARS CoV-2 virus 6.9 S/C (normal 1/4 S/C),, the lactic acid3
Nelson, J. Post-COVID Opsoclonus3.8, CRP 0.75 (normal 0.5 mg/dL). Normal serum testing: GQ1B antibodies, Mayo ClinicPAVAL panel, CBC, CMP, ANA, ENA, and ESR. Negative nasopharyngeal testing: SARSCoV-2 RT-PCR (tested twice), influenza, parainfluenza, RSV, mycoplasma, bordetella pertussis,bordetella parapertussis, chlamydia pneumoniae, rhino/enterovirus, metapneumovirus, andadenovirus. A chest x-ray on admission showed patchy opacities, but no ground glass opacities,in the right lung representing pneumonia.AcceptedMRI of the brain w/wo contrast on hospital day 2 showed modest caudate nuclei hyperintensitiesin T2 Fluid attenuated inversion recovery (FLAIR) sequence and DWI but without restricteddiffusion. A 30-minute EEG on hospital day 2 and an overnight EEG from days 3-4 werenegative for seizures or epileptiform discharges. Neuropsychological evaluation on hospital day3 (prior to starting Solumedrol) showed symmetrically impaired fine motor dexterity speedbimanually. Her encephalopathy manifested as slower mental processing speed, particularly inperforming visual-construction tasks with a heavier executive demand, mental flexibility, visualmemory, or non-contextual verbal encoding. We treated her with 1000mg IV Solumedrol for 5days and clonazepam 0.25mg BID and 0.5mg at night. She improved after her second dose ofSolumedrol. She was able to ambulate more steadily, and her ocular flutter was only present withconvergence whereas before it was also present with vertical and horizontal saccadic eyemovements. We discharged her on day 5 with an oral steroid taper.Ten days after discharge, she had residual, albeit improved, limb and trunk ataxia, and the familynoted that occasional eye movements present behind closed eyelids, which were presentpreviously, has resolved. We recorded the eye movements using the Otometrics Chartr- 200goggles with the head fixed (Trustup, Denmark). She had normal eye movements and steadyfixation in response to visual targets; however, she had intermittent bursts of multidirectional,fast, large amplitude saccades without an intersaccadic interval, characteristic for opsoclonus,exclusively with fixation block (Figure 1, Video 2 section 2). These oscillations persistedthroughout the five-minute recording. We did not see these movements with eyelid closure at aquick glance. This was concerning for suboptimal response to steroids, therefore, we initiatedfurther workup and administered a 750mg Rituximab infusion. CT chest abdomen pelvis wasnegative for cancerous lesions but showed pulmonary ground-glass opacities in the right lowerlung that appeared improved from her CXR showing a larger opacity limited to the right lowerlung 19 days earlier. Serum ANA, ENA, CA-125, CEA were negative. She showed significantimprovement two weeks after the Rituximab infusion. The examination and video recording fourweeks after symptom onset and hospitalization were normal; the patient returned to work.Discussion:The striking myoclonus and hyperekplexia represent a dramatic, but potentially curable,neurologic syndrome. In our patient, the initial eye abnormalities were more severe prior to the4
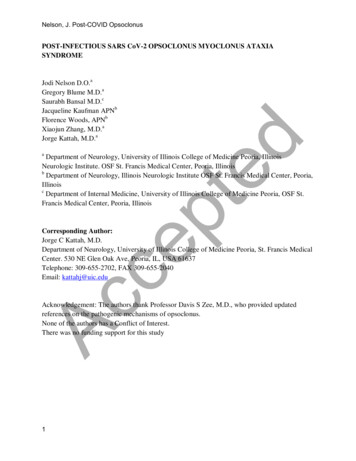
Nelson, J. Post-COVID Opsoclonusfirst bedside eye movement video n (recorded after the first high-dose of steroids on hospital day4). Macro-saccadic oscillations (MSO) were present primarily during vertical saccade refixations(Video 2, first section).tedWhereas the etiology of OMAS in children and older adults is paraneoplastic, in younger adultsit is often post-infectious. Regardless of age, brain imaging may be normal. Also, opsoclonusdoes not occur in natural or experimental lesions in primates[1]. Additionally, neuropathologicalexamination in paraneoplastic opsoclonus typically lacks definitive macro- or microscopicabnormalities [1, 2]. In particular, the pause cells, initially proposed as the principal OMAS cell –group target, showed no microscopic abnormalities[3]. However, one patient with paraneoplasticopsoclonus had sparse gliosis and mild lymphocytic infiltrates in the fastigial nucleus (FN) andinspired the first OMAS computer model.[2].AccepThe current theoretical mechanisms to explain the ocular oscillations in these patients involvesimultaneous neuron dysfunction in the brainstem and cerebellum [1, 4, 5]. The brainstem circuitrytheoretically involves omnipause neuron (OPN) inability to regulate post-inhibitory rebound(PIR) from oscillating excitatory (EBN) and inhibitory burst neuron (IBN) circuits in the pons [68]Disruption of this mechanism causes back-to-back saccades without intersaccadic intervals(Figure 1). Although not documented with Video-nystagmography (VNG) in this case,convergence/divergence refixations (known to suppress OPN), [7, 9] caused transient ocularoscillations in our patient. They likely represent ocular flutter, and thus support a brainstem roleas well (Video 3), recorded on day 5 of admission, and the second day of high-dose steroids) [7].In addition to altered membrane excitability in the EBN/IBN circuit and PIR, disinhibition of theFN causes increased, non-rhythmic eye oscillations. In humans, lesions of the fastigial nucleuscause saccade hypermetria [1, 7, 10]; our patient had similar saccades (Video 2, Section 1). In astudy, serum from three out of seven patients with opsoclonus had anti-Purkinje cell antibodieswith punctate staining in the cerebellar molecular layer, presumably directed against the parallelfiber-Purkinje cell synapse [11]. Moreover, PET scan hyperactivation of cerebellar nuclei supportsthe potential role of deep cerebellar nuclei[12].A recent simulation model[5] based on opsoclonus related to anabolic steroids, which modulateGABAA receptors, implies mistimed neuronal activity in the brainstem and cerebellum in thepathogenesis of opsoclonus. This may explain the findings in our patient [5, 13]. In theirmathematical model, the steroids increased sensitivity of the GABAA receptor leading toincreased GABA inhibition of neurons in the FN, and OPN. FN inhibition did not allow saccadesto stop on target. Delayed OPN reactivation caused a return movement with no saccadic interval,driven by PIR. The varying degree of FN, OPN inhibition leads to a continuum of movementsincluding MSO, ocular flutter, and opsoclonus; our patient had these same eye movements. Thissuggests a simultaneous brainstem-cerebellar mechanism. [2,[5] 11, 12].5
Nelson, J. Post-COVID OpsoclonustedAs a potential example, using abnormal eye movements in OMAS, one could draw an analogousexplanation for the head and truncal tremor in our patient have a similar etiology. Irregularoscillations of motoneurons innervating the trunk and neck may originate in the cerebellum,particularly regions of the FN that control movement of axial musculature [5, 14] (Video 1). In ourcase, elevation of NSE (a neuronal lesion marker) and the absence of white matter MRI changes[15]suggests Purkinje cell, cerebellar deep-nuclei and pontine neurons rather than cerebellaroutflow tracts as the cause of the abnormal eye movement and the symmetric limb and truncalataxia. Of note, elevated NSE did not preclude full recovery of function after treatment. Ingeneral, alteration of function in OMAS responds well to management and this may be predictedby the fact that PET CT has shown cerebellar deep nuclei hyperactivity, and not hypoactivity asone would expect with irreversible injuryAccepThe waveform of the oscillations in these patients includes large amplitude back-to-backsaccades and, as seen in this case, MSO and flutter [16]. The oscillations remained with eyelidclosure, as noted by the patient’s family. In a previous instance, they occurred during REM sleep[17]. In some cases, they developed in lateral gaze [18] and in some instances triggered by positonchanges[19] . Interestingly, we recorded overt opsoclonus with fixation-block ten days aftersymptom onset (Figure 1); this suggests that PIR may be fixation-suppressed and equivalent toprevious studies that showed persistent opsoclonus with eye closure [1, 3]. Therefore, vision maybe important in restoring or hasting the proper timing of neuronal activation in theEBN/IBN/omnipause neuron circuit.Treatment typically includes combinations of steroids, IVIG, and plasma exchange. However,others used azathioprine, rituximab and mycophenolate mofetil with success [20, 21] . We choseRituximab in our case since it has a longer half-life than IVIG. Rituximab improved opsoclonusmyoclonus syndrome in children with or without neuroblastoma [22]. The mechanism may bethrough CD20- B cell population normalization; however, an exact explanation is unclear. Whilethere is minimal data on adults, we could apply the pediatric experience to adults. Our patient’sVOG two weeks later showed steady fixation in all testing conditions, possibly reflecting thebeneficial effect of Rituximab on the presumed post-viral OMAS antibody. The paraneoplasticsyndrome often precedes diagnosis of cancer and improves at slower pace after tumor resectionor cancer specific treatment [3]. Idiopathic/non-paraneoplastic etiologies appear to be monophasicwith hastened recovery following immunotherapy, as in our case [23].Our case highlights a SARS CoV-2 para/post-infectious OMAS in the setting of subclinicalpneumonia. Recent reports suggest that OMAS may be an infrequent post –SARS-CoV-2neurologic syndrome [24-27]. The bilateral caudate hyperintensities on MRI, high NSE andencephalopathy suggest additional CNS targets [28, 29]. CSF may be normal in patients withOMAS, [22, 25, 29] however; to our knowledge, NSE was not tested. We add to previous post6
Nelson, J. Post-COVID OpsoclonusAcceptedSARS-CoV2 OMAS reports with serial clinical, ocular motor and immunologic findings beforeand after Rituximab-associated remission. Serum immunologic testing is valuable whenconfronting unexplained neurologic abnormalities in patients exposed to SARS CoV-2 andnegative nasopharyngeal RT-PCR testing.7
Nelson, J. Post-COVID OpsoclonusREFERENCES2.3.4.5.6.7.8.9.Accep10.Leigh, R.S., Zee,D.S., The Neurology of Eye Movements. 2915, Oxford, New York:Oxford University Press.Wong, A.M., et al., Opsoclonus in three dimensions: oculographic, neuropathologic andmodelling correlates. J Neurol Sci, 2001. 189(1-2): p. 71-81.Ridley, A., et al., Omnipause neurons in two cases of opsoclonus associated with oatcell carcinoma of the lung. Brain, 1987. 110 ( Pt 6): p. 1699-709.Oh, S.Y., J.S. Kim, and M. Dieterich, Update on opsoclonus-myoclonus syndrome inadults. J Neurol, 2019. 266(6): p. 1541-1548.Optican, L.M. and E. Pretegiani, A GABAergic Dysfunction in the Olivary-CerebellarBrainstem Network May Cause Eye Oscillations and Body Tremor. II. Model Simulationsof Saccadic Eye Oscillations. Front Neurol, 2017. 8: p. 372.Optican, L.M. and E. Pretegiani, What stops a saccade? Philos Trans R Soc Lond B BiolSci, 2017. 372(1718).Ramat, S., et al., Ocular oscillations generated by coupling of brainstem excitatory andinhibitory saccadic burst neurons. Exp Brain Res, 2005. 160(1): p. 89-106.Shaikh, A.G., et al., Saccadic burst cell membrane dysfunction is responsible forsaccadic oscillations. J Neuroophthalmol, 2008. 28(4): p. 329-36.Busettini, C. and L.E. Mays, Pontine omnipause activity during conjugate anddisconjugate eye movements in macaques. J Neurophysiol, 2003. 90(6): p. 3838-53.Buttner, U., A. Straube, and A. Spuler, Saccadic dysmetria and "intact" smooth pursuiteye movements after bilateral deep cerebellar nuclei lesions. J Neurol NeurosurgPsychiatry, 1994. 57(7): p. 832-4.Jen, J.C., I. Lopez, and R.W. Baloh, Opsoclonus: clinical and immunological features. JNeurol Sci, 2012. 320(1-2): p. 61-5.Mustafa, M., et al., Postinfectious Opsoclonus-Myoclonus Syndrome in a 41-Year-OldPatient-Visualizing Hyperactivation in Deep Cerebellar Nuclei by Cerebral [(18) F]-FDGPET. J Neuroimaging, 2015. 25(4): p. 683-5.Pretegiani, E., et al., GABAAergic dysfunction in the olivary-cerebellar-brainstemnetwork may cause eye oscillations and body tremor. Clin Neurophysiol, 2017. 128(3): p.408-410.Zhang, X.Y., J.J. Wang, and J.N. Zhu, Cerebellar fastigial nucleus: from anatomicconstruction to physiological functions. Cerebellum Ataxias, 2016. 3: p. 9.Royds, J.A., W.R. Timperley, and C.B. Taylor, Levels of enolase and other enzymes inthe cerebrospinal fluid as indices of pathological change. J Neurol Neurosurg Psychiatry,1981. 44(12): p. 1129-35.Zee, D.S. and D.A. Robinson, A hypothetical explanation of saccadic oscillations. AnnNeurol, 1979. 5(5): p. 405-14.Ellenberger, C., Jr., J.L. Keltner, and M.H. Stroud, Ocular dyskinesia in cerebellardisease. Evidence for the similarity of opsoclonus, ocular dysmetria and flutter-likeoscillations. Brain, 1972. 95(4): p. 685-92.Rizzo, J.R., et al., Eye position-dependent opsoclonus in mild traumatic brain injury.Prog Brain Res, 2019. 249: p. 65-78.Lemos, J. and E. Eggenberger, Saccadic intrusions: review and update. Curr OpinNeurol, 2013. 26(1): p. 59-66.Zutt, R., et al., A novel diagnostic approach to patients with myoclonus. Nat Rev Neurol,2015. 11(12): p. 687-97.ted1.11.12.13.14.15.16.17.18.19.20.8
Nelson, J. Post-COVID Opsoclonus22.23.24.25.26.27.28.Accep29.Klaas, J.P., et al., Adult-onset opsoclonus-myoclonus syndrome. Arch Neurol, 2012.69(12): p. 1598-607.Pranzatelli, M.R., et al., Rituximab (anti-CD20) adjunctive therapy for opsoclonusmyoclonus syndrome. J Pediatr Hematol Oncol, 2006. 28(9): p. 585-93.Bataller, L., et al., Clinical outcome in adult onset idiopathic or paraneoplasticopsoclonus-myoclonus. Brain, 2001. 124(Pt 2): p. 437-43.Emamikhah, M., et al., Opsoclonus-myoclonus syndrome, a post-infectious neurologiccomplication of COVID-19: case series and review of literature. J Neurovirol, 2021.27(1): p. 26-34.Shah, P.B. and S.D. Desai, Opsoclonus Myoclonus Ataxia Syndrome in the Setting ofCOVID-19 Infection. Neurology, 2021. 96(1): p. 33.Sanguinetti, S.Y. and R.A. Ramdhani, Opsoclonus-Myoclonus-Ataxia Syndrome Relatedto the Novel Coronavirus (COVID-19). J Neuroophthalmol, 2021.Ishaq, H., et al., Post-COVID Opsoclonus Myoclonus Syndrome: A Case Report FromPakistan. Front Neurol, 2021. 12: p. 672524.Sountharalingam, S., et al., Opsoclonus myoclonus syndrome in a patient with Japaneseencephalitis: a case report. J Med Case Rep, 2017. 11(1): p. 294.Armangue, T., et al., Clinical and Immunological Features of Opsoclonus-MyoclonusSyndrome in the Era of Neuronal Cell Surface Antibodies. JAMA Neurol, 2016. 73(4): p.417-24.ted21.9
Nelson, J. Post-COVID OpsoclonusFigure and Video Legends:AcceptedFigure 1. Video-Oculography Recording of primary eye position with fixation block. Note aburst of conjugate, non-rhythmic, 40- deg amplitude saccades without intersaccadic interval (A),with a frequency of 7 Hz, and a vertical component. There are also oscillations withintersaccadic interval and one square wave jerk.10
Nelson, J. Post-COVID OpsoclonusVideo 1. Note truncal oscillations and Finger to nose dysmetria with open and closed eyesVideo 2. Section 1 the patient has vertical saccadic oscillations during saccade refixations; theVideo recorded one dose of high-dose steroids. Section 2 recording with fixation block, ten dayslater shows irregular saccade bursts, they are primarily horizontal conjugate, fast saccades, with asmall vertical component. (We obtained Figure 1 during this video recording).AcceptedVideo 3. Obtained 24 hours after Video 1; it shows brief ocular flutter during convergence11
Nelson, J. Post-COVID OpsoclonusStatement of Authorshipted1. Category 1:a) Conception and designJodi Nelson, D.O.Jorge C Kattah, M.D.b) Acquisition of dataJodi Nelson, D.O.Gregory Blume, M.D.Saurabh Bansal, M.D.Jacqueline Kaufman, APNFlorence Woods, APNXiaojun Zhang, M.D.Jorge Kattah, M.D.c) Analysis and interpretation of dataJodi L Nelson, D.O.Jorge C Kattah, M.D.Accep2. Category 2:a) Drafting the manuscriptJodi L Nelson, D.O.Jorge C Kattah, M.D.b) Revising it for intellectual contentJodi Nelson, D.O.Gregory Blume, M.D.Saurabh Bansal, M.D.Jacqueline Kaufman, APNFlorence Woods, APNXiaojun Zhang, M.D.Jorge Kattah, M.D.3. Category 3:a) Final approval of the completed manuscriptJodi Nelson, D.O.Gregory Blume, M.D.Saurabh Bansal, M.D.Jacqueline Kaufman, APNFlorence Woods, APNXiaojun Zhang, M.D.Jorge Kattah, M.D.12
convergence whereas before it was also present with vertical and horizontal saccadic eye movements. We discharged her on day 5 with an oral steroid taper. Ten days after discharge, she had residual, albeit improved, limb and trunk ataxia, and the family noted that occasional eye movements present behind closed eyelids, which were present