Transcription
Psychiatric Hospital AccreditationOverview, Resources, and Compliance StrategiesPresented by:Chad Larson, MBA, Executive Director, Hospital Accreditation ProgramGayle Jensen-Savoie, LPC-S, LMFT-S, LCDC, Field Director, InpatientBehavioral Health Services
Our PresentersChad Larson holds an MBA, with an emphasis in Healthcare ServicesAdministration. He is the Executive Director for Hospital Accreditationprogram at The Joint Commission. In this role, he is responsible for buildingnew client relationships with hospitals who are new to the accreditationprocess. A 15-year Joint Commission employee, Chad also leads customerservice and retention efforts, and develops and carries out annualstrategic initiatives in response to the changing healthcare environmentallandscape.Gayle Jensen-Savoie holds a Doctorate degree in Psychology. She is aLPC-S, LMFT-S and a LCDC. She currently serves as a Field Director at TheJoint Commission, responsible for oversight and education of the surveyorcadre. Prior to her Field Director role, Dr. Jensen-Savoie surveyed for 7years to the standards in the Comprehensive Accreditation Manual forBehavioral Health Care. Dr. Jensen-Savoie has over 20 years’ experiencemanaging inpatient and outpatient psychiatric and addiction facilities. Herfield of expertise is ADHD, addiction and young adults.2 2019 The Joint Commission. All Rights Reserved.
Webinar Objectives Provide an overview of how The JointCommission goes beyond accreditation Understand how The Joint Commission workswith psychiatric hospitals and inspires them todeliver high quality, safe patient care Review emerging risk points and compliancestrategies for psychiatric hospitals3 2019 The Joint Commission. All Rights Reserved.
The Joint Commission Disclaimer These slides are current as of December 8, 2020. The JointCommission and the original presenters reserve the right to changeor update the content of the information, as appropriate. The Joint Commission reserves the right to review and retire contentfrom this presentation that is not current, has been made redundantor has technical issues. These slides are meant to be cue points, to be expounded uponverbally by the original presenters. These cue points are not meant tobe comprehensive statements of standards, their interpretation orrepresent all content of the presentation. Thus, care should beexercised in interpreting Joint Commission requirements basedsolely on the content of these slides. These slides are copyrighted and may not be further used, shared ordistributed without permission of the original presenters and theDivision of Accreditation and Certification Operations.4 2019 The Joint Commission. All Rights Reserved.
About The Joint Commission A global improvement company A focus beyond accreditation: Creating and deliveringeffective solutions to address persistent quality andsafety improvement efforts in healthcare Setting and maintaining modern, relevant, evidencebased standards Exceeding customer expectations Evaluating and improving everything we do usingLean Six Sigma methodologies Founded in 1951 under guidance of AHA, AMA, ACP,ACS to act as independent accrediting body forhospitals: Nation’s oldest and largest standards-setting andaccrediting body in health care: 68% of all U.S. hospitals are Joint Commissionaccredited 85% of all U.S. psychiatric hospitals areJoint Commission accredited5 2019 The Joint Commission. All Rights Reserved.
Benefits of Psychiatric Hospital Accreditation Helps identify risks and ways your psychiatric hospital canreduce potential adverse events More than 40 surveyors with specific behavioral health caresetting experience who provide best practices specific topsychiatric hospitals Cost is minimal when compared to the savings of risk that maycause harm to patients, staff, and visitors of your organization Numerous resources and tools to advance patient safety andquality in your organization The Joint Commission’s Gold Seal of Approval is anachievement that symbolizes an organization’s commitment toquality and safety6 2019 The Joint Commission. All Rights Reserved.
A Patient-Centric SurveyProcess7 2019 The Joint Commission. All Rights Reserved.
Surveyors Specializing in Psychiatric Settings Customizing our surveyor skills and selection in order to meetour customer needs: Employed surveyors working actively in the fields to whichthey survey Survey team selection based upon organizational setting Survey tracers focus on highest risks (e.g., suicide riskreduction, medication management) Annual survey option customized to organization’s priorities Collaborative approach that is data-driven, organizationspecific, and patient-centric Engaging staff throughout the survey; enabled by technology Actively engaging organizational leadership to inspire them ontheir own high reliability and zero harm journey8 2019 The Joint Commission. All Rights Reserved.
The On-Site Survey: Providing Best-in-ClassExpertise Through a Collaborative ExperienceThe survey process isdata-driven, patientcentered, and focused onproviding actual careprocesses, using ourtracer methodology as arisk reduction strategyOffer, share and observe leadingpractices gleaned from accreditedcommunityConduct educationally focusedsurveysLead a collaborative engagement thathelps to increase staff awarenessand educationInspire staff and support efforts toimprove performance and quality ofpatient care9 2019 The Joint Commission. All Rights Reserved.
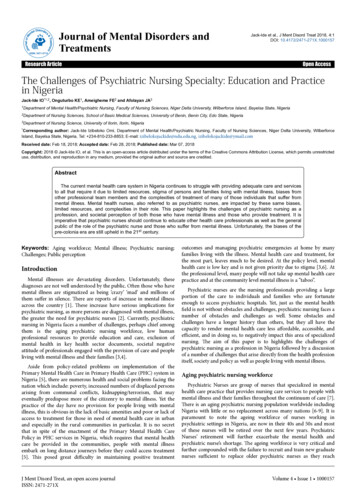
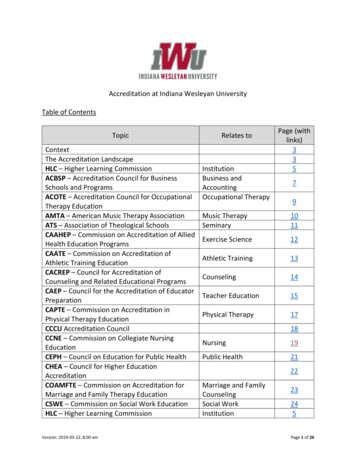
Focus On Identifying Areas of Risk Data-driven approachinforms organizations onareas of risk within yourpsychiatric hospital Prioritize improvementefforts and ensuresefficient utilization ofresources Compare/benchmarkacross health system Identifies negativetrends that have a stronglikelihood to developover timeLIKELIHOOD TO HARM Communicates mostsusceptible risk points insimplified visual:Immediate Threat to Health or SafetyHIGHHarm mayhappen at anytimeMM.03.01.01, EP8MODERATEHarm mayhappenoccasionallyMS.01.01.01, EP5PC.01.02.03, EP6PC.01.03.01, EP1LOWHarm mayhappen but rareMS.08.01.01. EP1MS.08.01.03, EP3IC.02.02.01, EP4PATTERNMultipleoccurrences, mayimpact more thana limited numberPatientsWIDESPREADPervasive,systemicfailure, mayimpactmost/all patientsRC.02.03.07, EP4LIMITEDUniqueoccurrence,limited impact topatientsSCOPE10 2019 The Joint Commission. All Rights Reserved.
Survey Agenda11 2019 The Joint Commission. All Rights Reserved.
Survey Activities12 2019 The Joint Commission. All Rights Reserved.
Resources to Advance Qualityand Safety for PsychiatricHospitals13 2019 The Joint Commission. All Rights Reserved.
Complimentary Educational Resources14 2019 The Joint Commission. All Rights Reserved.
Resources on Suicide Prevention15 2019 The Joint Commission. All Rights Reserved.
Resources to Address Workplace Violence16 2019 The Joint Commission. All Rights Reserved.
Dashboards and Continuous Compliance ToolsSAFER Dashboard Analytics tool usingsurvey findings andpresenting them inaggregate dashboard Empowers timely,data-driven decisionsto drive delivery ofsafe, high-quality care Use as an internalcomparison toolacross health system17 2019 The Joint Commission. All Rights Reserved.
Dashboards and Continuous Compliance ToolsAccelerate PI Dashboard Compare organizational performance to national, state andJoint Commission-accredited averages on specific performancemeasures Incorporated in the on-site survey process to help facilitatediscussion about ongoing quality improvement work Resources and webinars provided from peer community tolearn best practices and address underperformance18 2019 The Joint Commission. All Rights Reserved.
Dashboards and Continuous Compliance ToolsHeads Up Report Identifies topics orthemes surveyors havecited on recent surveys Provides ways touncover similar issuesand contributing factorsin your organization Intended to help identifyand resolve potentialproblems that mayimpact safe and effectivedelivery of care19 2019 The Joint Commission. All Rights Reserved.
Resources to Meet Standards Compliance Standards compliance assistance: Technical experts available to answer questions Standards FAQ’s published by chapter and keyword search 40 published FAQ’s to address suicide prevention20 2019 The Joint Commission. All Rights Reserved.
Continuous Compliance Tools21 2019 The Joint Commission. All Rights Reserved.
Continuous Compliance Tools22 2019 The Joint Commission. All Rights Reserved.
High Reliability Assessment Tool Online, self-guided, organizationalassessment Identifies an organization's readinessand advancement towards highreliability Uses a series of questions across 14areas of performance Four stages of maturity leveladvancement - beginning,developing, advancing,approaching Resource Library provideseducational resources and changemanagement strategies to assist onthe journey23 2019 The Joint Commission. All Rights Reserved.
Frequently Cited Standards inPsychiatric HospitalsCompliance Strategies forPsychiatric Hospitals24 2019 The Joint Commission. All Rights Reserved.
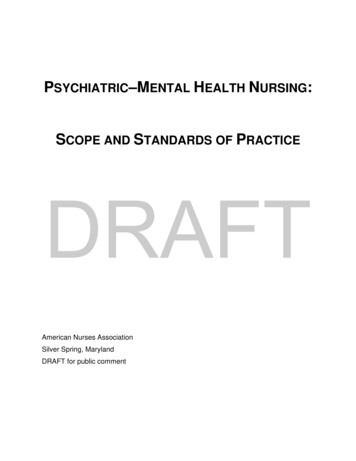
Aggregate SAFER Matrix DataPsychiatric HospitalsJanuary 1, 2019 - November 1, 2020Likelihood to Harm aPatient/Staff/VisitorImmediate Threat to Health or Safety0.1 IDESPREADScope25 2019 The Joint Commission. All Rights Reserved.
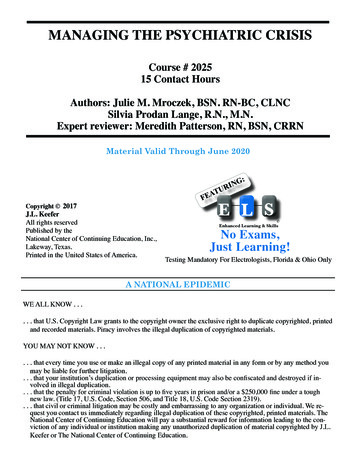
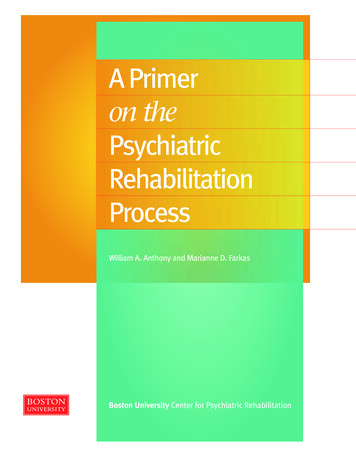
Top 10 Frequently Cited StandardsJanuary 2019-November 1, 2020Psychiatric EvaluationPC.01.02.13 EP 2Treatment PlansPC.01.03.01 EP 6Suicide Risk AssessmentNPSG.15.01.01 EP 1Discharge SummaryRC.02.04.01 EP 3Safe EnvironmentEC.02.06.01 EP 1Extinguishing FireLS.02.01.35 EP 4Utility System LabelingEC.02.05.01 EP 9Utility Systems; Inspect, Test & MaintainEC.02.05.05 EP 6Treatment PlansPC.01.03.01 EP 1Fire ProtectionLS.02.01.10 EP 14020406080100120Number of Requirements for Improvements (RFIs)14016020018026 2019 The Joint Commission. All Rights Reserved.
Top 10 Clinical FindingsJanuary 1, 2019 – November 1, 2020PC.01.02.13 EP 2Psychiatric EvaluationTreatment PlansPC.01.03.01 EP 6Suicide Risk AssessmentNPSG.15.01.01 EP 1Discharge SummaryRC.02.04.01 EP 3PC.01.03.01 EP 1Treatment PlansPC.01.03.01 EP 5Treatment PlansFood/Nutrition StoragePC.02.02.03 EP 11Neurological ExamPC.01.02.13 EP 6Treatment ActivitiesPC.01.03.01 EP 43IC.02.01.01 EP 1Infection Control0020204040606080100120140160180200Number of Requirements for Improvements (RFIs)27 2019 The Joint Commission. All Rights Reserved.
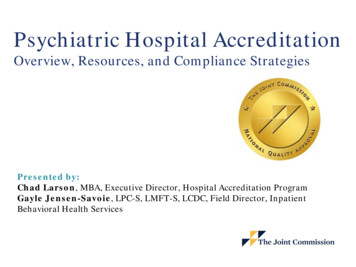
Top 10 Environment of Care/Life Safety Code FindingsJanuary 1, 2019 – November 1, 2020EC.02.06.01 EP 1Safe EnvironmentLS.02.01.35 EP 4Sprinkler System as SupportEC.02.05.01 EP 9Utility System LabelingUtility Systems; Inspect, Test & MaintainEC.02.05.05 EP 6LS.02.01.10 EP 14Fire ProtectionExtinguishing FireLS.02.01.35 EP 14Fire DoorsLS.02.01.10 EP 11Hazardous WasteEC.02.02.01 EP 5LS.02.01.35 EP 5EC.02.03.05 EP 28Sprinklers002040 of Alarm60 Testing80Documentation4020 Number1001201406014080 for Improvements120 (RFIs)100of Requirements16018016018028Number of Requirements for Improvements (RFIs) 2019 The Joint Commission. All Rights Reserved.
Compliance Strategies forFrequently Cited Standards29 2019 The Joint Commission. All Rights Reserved.
Psychiatric Evaluation (PC.01.02.13, EP 2)Deficiency Examples No documented estimate of intellectual functioning,memory functioning, and orientation withdocumentation of supporting information in admissionassessment Mental Status Exam as part of the AdmissionPsychiatric Evaluation did not document the patient’sbehaviors used to conclude judgement and insight Patient strengths and weaknesses in the psychiatricassessment were described in overly generalizedterms that were not sufficiently descriptive fortreatment plan use No supporting evidence for the documented degree ofcognitive impairment30 2019 The Joint Commission. All Rights Reserved.
Psychiatric Evaluation (PC.01.02.13, EP 2)Compliance Strategies Document reason for admission as stated by patientand/or family Do not be vague! Record “who” “what” “where”“when” “why” Psychiatric Evaluation Include mental status exam that describesappearance and behavior, emotional response,verbalization, thought content, and cognition Document onset of illness & reason forhospitalization Describe attitudes and behaviors Include intellectual functioning, memoryfunctioning and orientation. Include supportingevidence as to how this was determined Describe patient’s assets31 2019 The Joint Commission. All Rights Reserved.
Treatment Plans (PC.01.03.01, EP 6)Deficiency Examples The treatment plan did not includeinterventions for active medical problems The patient plan of care did not include thespecific, individualized treatment modalities. Treatment plan did not include asubstantiated diagnosis32 2019 The Joint Commission. All Rights Reserved.
Treatment Plan (PC.01.03.01, EP 6)Compliance Strategies The Treatment Plan should be the blueprint for all treatmentdelivered to patient Substantiated Diagnosis documented in treatment plan Serves as basis for treatment interventions Developed by synthesizing data from various disciplines Rule-out diagnosis is NOT substantiated diagnosis Specific Treatment Modalities documented in treatment plan Simply “stating” modality approach (i.e. “set limits” or “encouragesocialization”) is NOT acceptable Simply “naming” modalities (i.e. “individual therapy” “grouptherapy” “medication education”) is NOT acceptable Treatment methods and interventions from all disciplines need tobe included in treatment plan Interventions must be specifically described to assure consistency Include specific focus of treatment for each patient for groupactivity interventions33 2019 The Joint Commission. All Rights Reserved.
Suicide Risk Assessment (NPSG.15.01.01, EP1)Deficiency Examples No comprehensive suicide risk assessment(SRA) Still highest score on SAFER Matrix (highpattern and high and widespread) Incomplete SRA SRA inaccurate/inconsistent with clinicalinformation in medical record SRA not completed per policy No synthesis of individual factors on SRA todetermine level of risk and interventionsbased on that level of risk34 2019 The Joint Commission. All Rights Reserved.
Suicide Risk Assessment (NPSG.15.01.01, EP1)Compliance Strategies Policy creation and/or revision: Suicide risk assessment (SRA) tool How often? By whom? Interventions based upon level of risk Define monitoring procedures Staff Training Demonstrated competency assessment for use of SRAtool Knowledge of policy/procedures Leadership Oversight Ensure policy/procedure adherence Rounding Audits of Medical Records35 2019 The Joint Commission. All Rights Reserved.
Discharge Summary (RC.02.04.01, EP3)Deficiency Examples The discharge summary did not include asummary of the circumstances and rationale foradmission Patient’s condition at time of discharge wasnot included in the discharge summary The discharge summary did not recap thepatient’s hospitalization to include theevaluation of treatment plan goals.36 2019 The Joint Commission. All Rights Reserved.
Discharge Summary (RC.02.04.01, EP3)Compliance Strategies Discharge Summary must include: Extent to which treatment plan goals were met Summary of patient’s hospitalization Reason for admission Treatment provided Baseline of psychiatric, physical, and social functioning attime of discharge Response to treatment Follow-up services (specific appointments & providernames if applicable) Psychiatric, medical/physical treatment and medicationregimen Summary of psychiatric, medical, and functional conditionat time of dischargeRC.02.04.01 EP3Usetreatmentplan as aguide37 2019 The Joint Commission. All Rights Reserved.
Safe Environment (EC.02.06.01, EP 1)Deficiency Examples Ligature Risk on Inpatient Units (still highest on SAFERMatrix) Doors and door hardware Drop Ceilings Beds with ligature risks Light Fixtures HVAC Vents Non-Tamper Proof Screws Sprinkler Heads Bathroom Fixtures (plumbing, toilet paperdispensers, paper towel dispensers, etc.) Grab Rails Window Treatments38 2019 The Joint Commission. All Rights Reserved.
Safe Environment (EC.02.06.01, EP 1)Compliance Strategies Consider the following for scoring CLD: Not all ligature risks were identified Plan of correction not developedand/or does not have an establishedtimeline to remove ligature risks Lack of development and/orcompliance with clinical mitigation toreduce the risk Policy/Procedure for suicide riskassessments Identify high risk patients Implement 1:1 monitoring of highrisk patients39 2019 The Joint Commission. All Rights Reserved.
Extinguishing Fire (LS.02.01.35, EP 4)Deficiency Examples Cabling wrapped around the sprinkler pipe Conduit, tubing, wiring supported by thesprinkler system40 2019 The Joint Commission. All Rights Reserved.
Extinguishing Fire (LS.02.01.35, EP 4)Compliance Strategy Ensure that the sprinkler pipingcannot be used to support anything.This includes items that aretouching the piping.41 2019 The Joint Commission. All Rights Reserved.
Utility System Labeling (EC.02.05.01, EP 9)Deficiency Examples The water source valve to the building was notlabeled The electrical panel did not have an accuratelegend depicting what the circuit breakersserve The fire alarm circuit disconnect/electricalbreaker was not identified42 2019 The Joint Commission. All Rights Reserved.
Utility System Labeling (EC.02.05.01, EP 9)Compliance Strategies At a minimum, the main valves/controlsfor the utility systems need to be labeled Electrical panel must have legend and beaccurately identified If the circuit breakers are installed theymust be identified on the legend whetherspares or in service.43 2019 The Joint Commission. All Rights Reserved.
Frequently Asked Questions1. What types of fees are associated withaccreditation?2. How may I obtain a copy of theaccreditation standards for psychiatrichospitals?3. What does the on-site survey look like?4. How does The Joint Commission ensureconsistency in how standards areinterpreted and ensuring surveyors take asimilar approach?Contact us at clarson@jointcommission.org44 2019 The Joint Commission. All Rights Reserved.
Benefits of Psychiatric Hospital Accreditation Helps identify risks and ways your psychiatric hospital can reduce potential adverse events More than 40 surveyors with specific behavioral health care setting experience who provide best practices specific to psychiatric hospitals Cost is minimal when compared to the savings of risk that may