Transcription
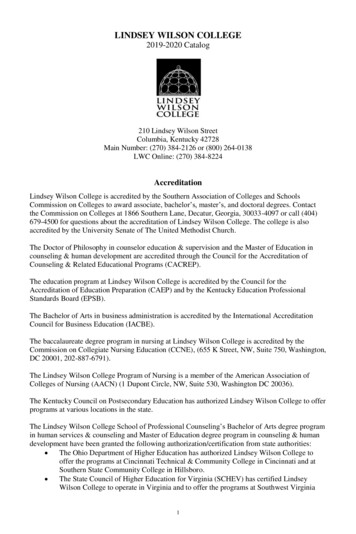
GROUP HEALTH PLANS - EMPLOYEE APPLICATION/WAIVERFARMERSNATIONALBANKLINDSEY WILSONCOLLEGEPPOPLANHDHPENROLLMENT NEW ENROLLMENT CHANGEPLANNEW ENROLLMENTCHANGE ENROLLMENTA. EMPLOYEE INFORMATIONLAST NAMEFIRST NAMEPARTICIPANT SSN:--MIPARTICIPANT DOB:ADDRESS//CITYZIP CODE COREPLAN TYPE:GENDER:MALEFEMALESTATE BUY-UPMARITAL STATUS:MARRIEDSINGLEEffective Date:HIRE DATE://Termination Date:B. COVERAGE YOU ARE REQUESTINGEMPLOYEE ONLYEMPLOYEE & FAMILYEMPLOYEE & FAMILYIF ENROLLMENT CHANGE PROVIDE QUALIFYING EVENT:C. FAMILY INFORMATION - ENROLLMENTSPOUSE: LAST NAMEFIRST NAMESPOUSE SSN:GENDER:MALE------CHILD DOB:MI//FIRST NAMECHILD SSN:MALE/FEMALECHILD: LAST NAMEGENDER:/FIRST NAMECHILD SSN:MALECHILD DOB:MIFEMALECHILD: LAST NAMEGENDER:/FIRST NAMECHILD SSN:MALE/FEMALECHILD: LAST NAMEGENDER:SPOUSE DOB:MIFEMALE-CHILD DOB:MI//
Are you or any ofyour Dependentscovered byMedicare?YesNoIf yes, complete theinformation on therightNameReasonOver 65DisabledEnd Stage Renal DiseaseNameReasonOver 65DisabledEnd Stage Renal DiseaseCovered by:Part APart BPart CPart DCovered by:Part APart BPart CPart DDates became effectiveMedicare NumbersA.B.C.D.A.B.C.D.////////Dates became effectiveMedicare NumbersA.B.C.D.A.B.C.D.////////Premium Payment: I authorize my employer to deduct the requested premium contribution from m y earnings.Authorization to Release Information: I hereby authorize any physician or medical practitioner, hospital, or other organization, institution or person that has any medical recordsor knowledge of me or my family as to diagnosis, treatment and prognosis regarding any physical, mental, drug or alcohol condition or any and all such information to be given toARC Administrators or its authorized Administrator or legal representative (including medical review specialists). Any information obtained will not be released by the insurancecompany except to persons or organizations performing business or legal services in connection with my application or claim, including but not limited to pre-certification of hospitaladmissions, Continued Stay Review, On-Site Concurrent Review or as may be otherwise lawfully required or as I further authorize. A photocopy of this authorization shall be validas the original and is valid for thirty (30) months from the date shown below.U.S. Resident: I understand that the coverage under this plan is available for United States Residents and benefits are not payable for medical expenses outside of the UnitedStates except while traveling.M y Answers Are True and Correct: I have personally reviewed all of my answers to the questions on this application and represent that all of the information I have provided istrue and complete. I understand that it is my responsibility to provide truthful, complete and accurate information and I represent I have fully understood all the questions asked.W ith the exception of health related factors, I understand that my intentional material misstatements or failure to report information may be used as the basis of rescission ortermination of coverage for me or my dependents, if any. I understand that under no circumstances is any agent allowed to (a) waive, alter or modify any questions; (b) permit me toinaccurately answer any questions; or (c) instruct me not to disclose any particular medical condition on the application. I understand that no agent is authorized or has authority toalter the terms of the Group Master Policy. W AIVER OF COVERAGE. This is to certify that I have been given an opportunity to insure myself and/or my eligible dependents and I have DECLINED s uchcoverage. I understand that if I am declining enrollment for myself or my dependents (including my spouse) because of other health insurance coverage, I may in thefuture be able to enroll myself and my dependents in this plan, provided that I request enrollment within thirty-one (31) days of my other coverage ending. In addition, ifI have a new dependent as a result of marriage, birth, adoption, party in a suit in which the adoption of child by me is sought or placement for adoption, I may be able toenroll myself and my dependents, provided that I request enrollment within thirty-one (31) days after the marriage, birth, adoption, party in a suit in which the adoption ofchild by me is sought or placement for adoption. If I choose to enroll myself or my dependents, at a later date, for a reason other than the special reasons stated herein, Iunderstand that I and/or my dependents may not enroll until my employer’s next enrollment period. I understand that I and/or my dependents will be subject to atwelve (12) month pre-existing conditions limitations period which may be proportionately reduced by my furnishing certification or creditable coverage for myself and/ordependents.Any person who, with intent to defraud or knowing that he/she is facilitating a fraud against an insurer, submits an application or files a claim containing a falseor deceptive statement is subject to civil and criminal penalties.D. SIGNATURESignature of Employee and Parent if Applicant is under the age eighteen (18) yearsSignatureEmployee and Parent if Applicant is under the age eighteen (18) yearsEmailofAddressDateDatePhone Number
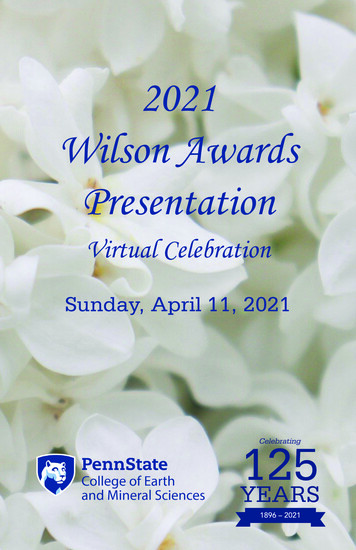
LINDSEY WILSON COLLEGEANTHEM HEALTH INSURANCE ELECTION FORMFOR PLAN YEAR 2018I hereby elect the following plan for the 2018 plan year.Single Core Plan - 45.91Single Buy-up Plan - 105.61Family Core Plan - 780.53Family Buy-Up Plan - 935.76Dual Employee Family Core Plan - 367.30Dual Employee Family Buy-Up Plan - 522.53I waive participation in the 2018 health insurance plan year.Print NameSignatureDate
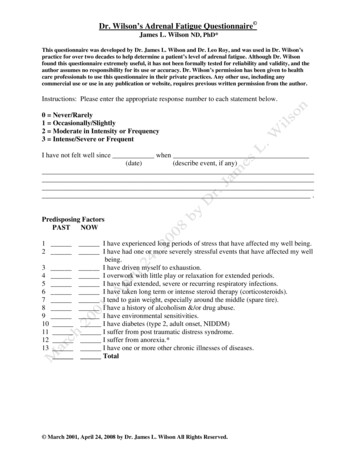
COORDINATION OF BENEFITS QUESTIONNAIREName:Address:City, State, Zip:Member ID:ARC Administrators coordinates benefits with other payers when a member is covered by two or more group benefit plans.THIS FORM IS REQUIRED TO BE COMPLETED ANNUALLY. In order to coordinate benefits accurately we request the followinginformation be completed and returned to us within 10 days upon receipt of this letter. If you prefer to provide the information over thephone, you may call us at 800- 250-5735.In addition to this medical coverage, are you or any of your covered dependents covered by another health plan? NO- Please skip the rest of the questions, sign, date on the back and return.YES- Please complete the entire form, sign, date on the back and return.Other Carrier NameOther Carrier AddressPolicy Holder NamePolicy Holder Date ofBirthGroup NumberSubscriber IDType of Coverage Single FamilyRelation to YouPolicy Holder EmployerEffective DateTermination DateIs this a retiree policy?YesNoIs this a COBRA policy?YesNoIs this a Medicaid policy?YesOther Carrier Phone NumberType of Plan:MedicalDentalVisionRXNoPlease list all dependents on this policyName (first and last)Relationship to YouName (first and last)Relationship to You1.3.2.4.Is this additional coverage court orderedNoYes (If yes, attach a copy of the Divorce Decree)Name and relationship of the person who has primary custodyIf this additional coverage is Medicare, please indicate why you have MedicareAgeDisabilityESRDPlease attach a copy of your cardMedicare Question EmployeeEffective Part AEffective Part BEffective Part DPolicy Holder NameAre you Retired?YesNoDate ofRetirementMedicare ID(HICN)If your Medicare benefits terminated, what part, and termination dateIf you have Medicare due to ESRD, please answer the following questionsDate Dialysis beganWhere did you receive treatmentHomeOutpatient / Dialysis CenterIf at home when did training begin?Date of TransplantWas the Transplant successfulYesNoWas second Transplant successfulYesNoIf No, was a second Transplant doneTURN OVER AND FINISH COMPLETINGYesNo
Did you resume dialysis after your transplant, and if so when?Medicare Question DependentPolicy Holder NameAre you Retired?Effective Part AYesNoDate ofRetirementEffective Part BEffective Part DMedicare ID(HICN)If your Medicare benefits terminated, what part, and termination dateIf you have Medicare due to ESRD, please answer the following questionsDate Dialysis beganWhere did you receive treatmentHomeOutpatient / Dialysis CenterIf at home when did training begin?Date of TransplantWas the Transplant successfulYesNoWas second Transplant successfulYesNoIf No, was a second Transplant doneYesNoDid you resume dialysis after your transplant, and if so when?Medicare Advantage QuestionIt is very important that you disclose if you, your spouse or any dependents are covered by a Medicare Advantage Plan becauseenrollment in this health plan can cause you to be dis-enrolled from the Medicare Advantage Plan (often provided by thespouses’ employer as part of their retirement benefits).A Medicare Advantage Plan is a health insurance program that serves as a substitute for “Original Medicare” Parts A and B MedicareBenefits. These traditional Medicare benefits are provided by a commercial insurance company (like Humana, Anthem, Cigna, andothers) but include benefits for prescription drugs, and often include office copay and other benefits common to an insurance plan –benefits that are not typically provided by Medicare Parts A & B. Medicare Advantage plan can include prescription drug coverage aspart of the plan and is subsidized by CMS (Center for Medicare Services).Is anyone covered under your police covered by a Medicare Advantage Plan?NoYes (complete the section below)Policy Holder NameEffective DateMedicare Advantage ID # as displayed on ID CardPolicy Holder NameEffective DateMedicare Advantage ID # as displayed on ID CardEmployee Signature:Date:Return completed form to: ARC Administrators, P.O Box 12290, Lexington, KY 40582Fax: 859-243-0381
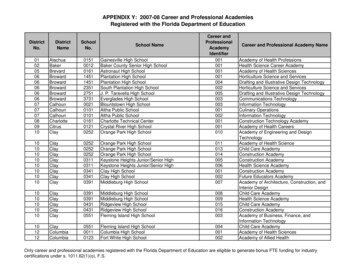
Life InsuranceBeneficiary Designation FormTHE EMPLOYER MUST KEEP THIS FORM ON FILE.Name of employer/group (if applicable)Policy/certification no.Name of insuredSocial security no.Name of policyowner (if different)Social security no.If you reside in a state with Marital or Community Property Laws, spousal consent is required if your spouse is not listed as a Primary Beneficiary for at least 50%.PRIMARY BENEFICIARY(IES): Person or persons who will receive the life insurance proceeds upon your death.NameDate of birthAddressNameRelationship to insuredDate of birthAddressNameSocial security no.Social security no.Relationship to insuredDate of birthAddress% to be paid to beneficiary% to be paid to beneficiarySocial security no.Relationship to insured% to be paid to beneficiaryTotal percentages should add up to 100%. If no percentages are indicated, the proceeds will be divided equally. If no Primary beneficiary survives,proceeds will be paid to the Contingent beneficiary(ies) listed below. Space is provided at the bottom of the page if you wish to name additionalPrimary or Contingent beneficiaries.CONTINGENT BENEFICIARY(IES): Person or persons who will receive the life insurance proceeds if there is no surviving primary beneficiary.NameDate of birthAddressNameRelationship to insuredDate of birthAddressNameAddressSocial security no.% to be paid to beneficiarySocial security no.Relationship to insuredDate of birth% to be paid to beneficiarySocial security no.Relationship to insuredSignature of insured or policyowner (2 officers’ signatures, with title, are required if corporate owned)% to be paid to beneficiaryDate signed (MM/DD/YYYY)XSignature of spouse (if not designated as primary beneficiary and residence is in community property state)Date signed (MM/DD/YYYY)XSi usted necesita ayuda en Español para entender este documento, puede solicitarlo sin ningun costo adicional llamandoal número de servicio al cliente que se encuentra en este documento.14469ANEENLBS 6/10Life and Disability products underwritten by Anthem Life Insurance Company, an independent licensee of the Blue Cross and Blue Shield Association. ANTHEM is a registered trademark of Anthem Insurance Companies, Inc. The Blue Cross and Blue Shield names and symbols are registered marks of the Blue Cross and Blue Shield Association.Page 1 of 2
Life InsuranceBeneficiary Designation Form - continuedTHE EMPLOYER MUST KEEP THIS FORM ON FILE.BENEFICIARY DESIGNATIONSDEFINITIONS:The purpose of designating beneficiaries for this policy is to instruct Anthem Life Insurance Company (Anthem Life) exactly how you wish the proceeds of yourpolicy/certificate to be paid upon your death. Therefore, please take a moment to read the examples below:PRIMARY BENEFICIARY:Person or persons to receive the Life Insurance proceeds upon the death of the Insured. If multiple Primary Beneficiaries are listed, death benefits are dividedequally among all the living Primary Beneficiaries, unless otherwise stated.CONTINGENT BENEFICIARY:Person or persons to receive the Life Insurance proceeds when the Primary Beneficiary(ies) dies before the Insured. If multiple Contingent Beneficiaries arelisted, death benefits are divided equally among all the living Contingent Beneficiaries, unless otherwise stated.EXAMPLES OF CORRECT BENEFICIARY DESIGNATIONS:Joe and Jane Smith — Father and MotherWilliam E. Brown — SpouseGeorge Jones — FriendDonald C. White, Jane E. Smith, and Richard E. Beck — ChildrenIf you choose the estate or a trust as beneficiary, see the following example beneficiary designation:Insured’s Estate: John Q. Smith –- trustee under the Mary R. Smith Trust dated 01/02/2006.Full given names of each beneficiary must be clearly stated.NOTE: INSUREDS OF GROUP INSURANCE MAY NOT DESIGNATE THEIR EMPLOYER AS BENEFICIARY. Employees should make a copy to keep for their personal record.Employers need to keep original on file. For All Voluntary benefits, a legible copy must be sent to Anthem Life.ADDITIONAL BENEFICIARY(IES)PRIMARYNameDate of birthAddressNameRelationship to insuredDate of birthAddressNameSocial security no.Social security no.Relationship to insuredDate of birthAddress% to be paid to beneficiary% to be paid to beneficiarySocial security no.Relationship to insured% to be paid to beneficiaryCONTINGENTNameDate of birthAddressNameAddressSocial security no.Relationship to insuredDate of birth% to be paid to beneficiarySocial security no.Relationship to insured% to be paid to beneficiaryPage 2 of 2
AUTHORIZATION FOR DISCLOSURE OFPROTECTED HEALTH INFORMATION (PHI)I hereby authorize ARC Administrators, it agents, subsidiaries, and affiliates, to disclose my medical, claim orbenefit records, including my Protected Health Information (PHI) as indicated below to the persons or entitiesspecified on this form.All sections must be completed for this authorization to be valid.1. VerificationIdentification of Member: (This is the member whose information will be released.)Name of Member whose information will be disclosed:Date of Birth:Member Address:Phone number where this member can be reached if we need to contact you:2. Description of Information to be ReleasedUnless specifically indicated differently on the line provided below, I hereby authorize the full release of allClaims, Eligibility and Benefit Information, Medical Records, and Care Coordination Information. Iacknowledge this information may be viewed through the online claim system as well as discussed over thephone. I understand that these records may contain information created by other persons or entities, includinghealth care providers. I further understand these records may contain information diagnosis and or treatmentinformation for Alcoholism, Drug abuse or dependency, Mental Illness, HIV and or Aids. In addition, Genetictesting information maybe contained within. If you want to specifically limit or restrict the information, dates,or manner in which the information this authorization covers may be disclosed please indicate the limitations onthe following line.Limitations on authorization:3. Person or Entity Authorized to Receive InformationName of the person or entity you are giving permission for ARC Administrators to release your ProtectedHealth Information (PHI) to.Name:4. Expiration of AuthorizationI understand that I may revoke this authorization at any time by notifying ARC Administrators in writing:Page 1 of 2
ARC AdministratorsPO Box 12290Lexington, KY40582This authorization expires when I am no longer a plan participant, unless otherwise specified on the line below.This authorization expires: .Please note: Information disclosed based on this authorization may be subject to redisclosure by the recipient andmay no longer be protected by federal privacy regulations. If the information on this form is not complete, ARC Administrators will return the form to you, and thisrequest will not be considered until ARC Administrators receives complete information. Coverage, treatment, payment, enrollment, and eligibility under the plan(s) for benefits does not dependon whether you sign this authorization, any authorization is completely voluntary.5. Signature of Member Authorizing the release of his/her InformationI have read and understand the information contained on this form and by signature am hereby expresslyauthorizing ARC Administrators to release my information as described above.Signature:Date:Please return this completed form to:Mail to:ARC AdministratorsP.O. Box 12290Lexington, KY 40582Fax to:(859) 243-0381Page 2 of 2
LINDSEY WILSON COLLEGE HEALTH BENEFIT PLAN210 Lindsey Wilson Street, Columbia, KY 42728270-384-7313Employment Verification form for Spouse**Any Spouse who is eligible for coverage through his/her own employeris not eligible for coverage from Lindsey Wilson College’s health benefit plan.**SECTION 1: This section to be completed by the participant (employee)Participant (employee) name:Participant Social Security number: XXX-XX-SECTION 2: This section to be completed and signed by the spouseSpouse name:Spouse signature: I am not employed at this time and if I become employed, I will complete a new “Employment verification form” toterminate coverage for myself as of the date that coverage is available to me through my employer. I am employed at this time and authorize my employer to complete the information on this form.SECTION 3: This section to be completed by the spouse’s employerDear Employer:Effective January 1, 2014, the Lindsey Wilson College Health Benefit Plan requires spouses to verify whether or not a spouse iseligible for coverage from the plan. For verification purposes, the employer must complete this “Employment Verification form”and return the completed form to the Lindsey Wilson College HR Office.Please verify the following information: We do not offer medical insurance. We offer medical insurance but this employee is not eligible to enroll because: .We offer medical insurance, and this employee is eligible to enroll / / in: Medical(date) Dental VisionWe offer medical insurance, and this employee is enrolled effective / / in: Medical(date) Dental VisionWe offer medical insurance however, this employee has chosen not to enroll effective / / in: Medical(date) Dental Vision Company Name:Company Benefits Representative:NameSignatureTelephoneDatePlease return this form to:Lindsey Wilson College HR Office210 Lindsey Wilson StreetColumbia, KY 42728Or fax: 270-384-7373Or Email: HR@LINDSEY.EDU
LINDSEY WILSON COLLEGE EMPLOYEE HEALTH PLANAUTHORIZATION TO VIEW DEPENDENT CLAIMS ONLINEAs a convenience to our participants ARC Administrators has established an online websitewhere participants of the Lindsey Wilson College Employee Benefit Plan will be able to log inand view their individual health claims. In addition to the individual participant’s health claims,upon written consent of the participant’s dependents, the participant will be able to view theirdependents health claims as well. This authorization only has to be completed and returned toARC Administrators if the participant wants to be able to view their dependents claims in theonline system.Section 1: This section to be completed by the participant (employee))Participant (employee) Name:Participant Member ID #:Participant Signature:Section 2: This section to be completed and signed by the spouseBy signing this authorization form I hereby give my spouse permission to view my health claimsin the online system.Spouse Name:Spouse Signature:Section 3: This section to be completed and signed by any other covered dependent over the ageof 18By signing this authorization form I hereby give participant permission to view my health claimsin the online system.Dependent Name:Dependent Signature:Dependent Name:Dependent Signature:Dependent Name:Dependent Signature:Completed Authorizations can be returned to ARC Administrators by the following methods:Mail to: ARC AdministratorsP.O. Box 12290Lexington, KY 40582Fax to:859-243-0381 Attn: Eligibility DepartmentEmail to:eligibility@arcsvs.comAccess to view participant’s dependents health claims will not be granted without this completedauthorization. If you have questions please contact us at 1-877-309-2955.
LINDSEY WILSON COLLEGE . ANTHEM HEALTH INSURANCE ELECTION FORM . FOR PLAN YEAR 2018. I hereby elect the following plan for the 2018 plan year. Single Core Plan - 45.91 Single Buy-up Plan - 105.61 Family Core Plan - 780.53 Family Buy-Up Plan - 935.76 Dual Employee Family Core Plan - 367.30 Dual Employee Family Buy-Up Plan - 522.53 I waive participation in the 2018 health insurance plan year.