Transcription
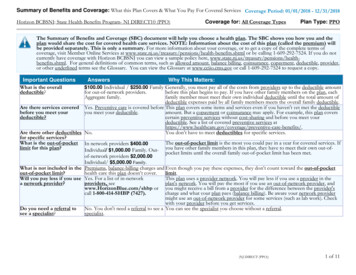
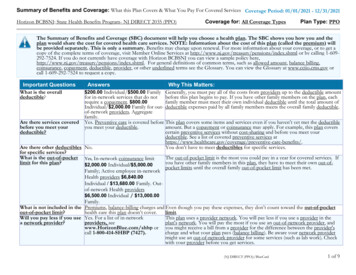
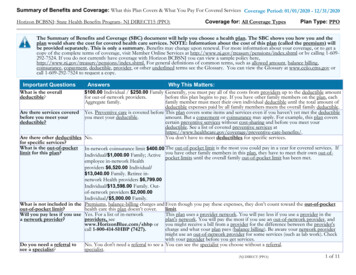
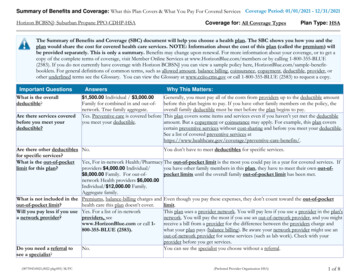
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2021 - 12/31/2021Horizon BCBSNJ: State Health Benefits Program- HORIZON HMOCoverage for: All Coverage TypesPlan Type: HMOThe Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and theplan would share the cost for covered health care services. NOTE: Information about the cost of this plan (called the premium) willbe provided separately. This is only a summary. Benefits may change upon renewal. For more information about your coverage, or to get acopy of the complete terms of coverage, visit Member Online Services at http://www.nj.gov/treasury/pensions/index.shtml or by calling 1-609292-7524. If you do not currently have coverage with Horizon BCBSNJ you can view a sample policy ml. For general definitions of common terms, such as allowed amount, balance billing,coinsurance, copayment, deductible, provider, or other underlined terms see the Glossary. You can view the Glossary at www.cciio.cms.gov orcall 1-609-292-7524 to request a copy.Important QuestionsWhat is the overalldeductible?Are there services coveredbefore you meet yourdeductible?Answers 0Why This Matters:See the Common Medical Events chart for your costs for services this plan covers.Yes. Preventive care is covered before This plan covers some items and services even if you haven’t yet met the deductibleyou meet your deductible.amount. But a copayment or coinsurance may apply. For example, this plan coverscertain preventive services without cost-sharing and before you meet yourdeductible. See a list of covered preventive services are-benefits/.Are there other deductibles Yes. 100.00 for medical appliances You must pay all of the costs for these services up to the specific deductiblefor specific services?and durable medical equipment.amount before this plan begins to pay for these services.What is the out-of-pocketlimit for this plan?The out-of-pocket limit is the most you could pay in a year for covered services. IfFor Active employee in-networkyou have other family members in this plan, they have to meet their own out-ofHealth providers 6,840.00pocket limits until the overall family out-of-pocket limit has been met.Individual / 13,680.00 Family.Retiree in-network Health providers 7,199.00 Individual/ 14,398.00Family.What is not included in the Premiums, balance-billing charges and Even though you pay these expenses, they don’t count toward the out-of-pocketout-of-pocket limit?health care this plan doesn’t cover.limit.Will you pay less if you use Yes. For a list of in-networkThis plan uses a provider network. You will pay less if you use a provider in thea network provider?providers, seeplan's network. You will pay the most if you use an out-of-network provider, andwww.HorizonBlue.com/shbp or you might receive a bill from a provider for the difference between the provider'scall 1-800-414-SHBP (7427).charge and what your plan pays (balance billing). Be aware your network providermight use an out-of-network provider for some services (such as lab work). Checkwith your provider before you get services.Do you need a referral toYes.This plan will pay some or all of the costs to see a specialist for covered services butsee a specialist?only if you have a referral before you see the specialist.(Health Maintenance Organization)1 of 8
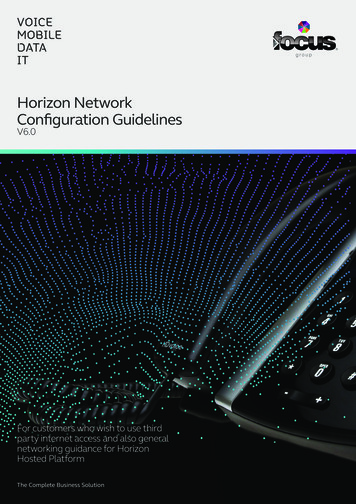
CommonMedical EventServices You May NeedIf you visit a health Primary care visit to treat ancare provider’s office injury or illnessor clinicSpecialist visitIf you have a testIf you need drugs totreat your illness orconditionWhat You Will PayLimitations, Exceptions, & OtherNetwork ProviderOut-of-NetworkImportant Information(You will pay theProvider(You will payleast)the most) 10.00 Copayment perActive State employees have 15.00Not Covered.visit.Copayment per visit. 10.00 Copayment pervisit.Not Covered.Preventivecare/screening/immunizationNo Charge.Not Covered.One per calendar year. You may haveto pay for services that aren'tpreventive. Ask your provider if theservices needed are preventive. Thencheck what your plan will pay for.Diagnostic test (x-ray, bloodwork)No Charge.Not Covered.Imaging (CT/PET scans, MRIs) No Charge.Not Covered.Requires pre-approval.Generic drugsnonenonePreferred brand drugsMore information about Non-preferred brand drugsprescription drugcoverage is availablethrough your employer. Specialty drugsSee separate Prescription Drug Plan SBCIf you haveoutpatient surgeryFacility fee (e.g., ambulatorysurgery center)No Charge.Not Covered.nonePhysician/surgeon feesNo Charge.Not Covered.noneEmergency room care 85.00 Copayment per visit 85.00 Copayment per visit 35 Copayment/visit for physicianfor Outpatient Hospital. for Outpatient Hospital. referrals or pediatric (under age 19) ERvisits; and if admitted within 24 hours,the Copayment is waived. Payment atthe in-network level applies only to trueMedical Emergencies & AccidentalInjuries. Active State employees have a 100 Copayment/visit; 50 Copayment/visit for dependent children under 19and Members who obtain a referral.If you needimmediate medicalattention* For more information about limitations and exceptions, see the plan or policy document athttp://www.nj.gov/treasury/pensions/index.shtml2 of 8
CommonMedical EventServices You May NeedEmergency medicaltransportationUrgent careIf you have ahospital stayIf you need mentalhealth, behavioralhealth, or substanceabuse servicesIf you are pregnantWhat You Will PayLimitations, Exceptions, & OtherNetwork ProviderOut-of-NetworkImportant Information(You will pay theProvider(You will payleast)the most)No Charge.Not Covered.Limited to local emergency transport tothe nearest facility equipped to treat theemergency condition. 10.00 Copayment pervisit.Not Covered.Active State employees have 15.00Copayment per visit.Facility fee (e.g., hospital room) No Charge.Not Covered.Requires pre-approval.Physician/surgeon feesNo Charge.Not Covered.Requires pre-approval.Outpatient servicesNo Charge for Outpatient Not Covered.Hospital. 10.00 Copayment perOffice visit for MentalHealth and BehavioralHealth. No Charge forSubstance abuse Officevisit.Some specialty outpatient servicesrequire pre-approval. Active Stateemployees have 15.00 Copayment peroffice visit for Mental Health andBehavioral Health. No Charge forSubstance Abuse office visit.Inpatient servicesNo Charge.Requires pre-approval.Office visits 10.00 Copayment per visit Not Covered.for Office.Childbirth/delivery professional No Charge.servicesNot Covered.Not Covered.* For more information about limitations and exceptions, see the plan or policy document ost sharing does not apply forpreventive services. Maternity care mayinclude tests and services describedelsewhere in the SBC (i.e. Ultrasound.).Active State employees have 15.00Copayment per visit.none3 of 8
CommonMedical EventServices You May NeedChildbirth/delivery facilityservicesIf you need helprecovering or haveother special healthneedsHome health careNo Charge.Rehabilitation servicesRequires pre-approval. Active Stateemployees have a 15.00 Copaymentper visit for Office.Skilled nursing careNo Charge for Inpatient Not Covered.and Outpatient Facility. 10.00 Copayment per visitfor Office.No Charge for Inpatient Not Covered.and Outpatient Facility. 10.00 Copayment per visitfor Office.No Charge.Not Covered.Durable medical equipmentNo Charge.Not Covered.Hospice servicesNo Charge.Not Covered.Requires pre-approval for all rentalsand some purchases. Subject to a 100medical appliance and durable medicalequipment deductible.Requires pre-approval.Children’s eye exam 10.00 Copayment pervisit.Not Covered.Coverage is limited to 1 visit. ActiveState employees have 15.00Copayment per visit.Children’s glassesNot Covered.Not Covered.noneChildren’s dental check-upNot Covered.Not Covered.noneHabilitation servicesIf your child needsdental or eye careWhat You Will PayLimitations, Exceptions, & OtherNetwork ProviderOut-of-NetworkImportant Information(You will pay theProvider(You will payleast)the most)No Charge.Requires pre-approval.Not Covered.Not Covered.* For more information about limitations and exceptions, see the plan or policy document equires pre-approval.Requires pre-approval. Limited to 120days per calendar year.4 of 8
Excluded Services & Other Covered Services:Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excludedservices.) Acupuncture Long Term Care Private-duty nursing (inpatient) Cosmetic Surgery Most coverage provided outside the UnitedStates. Routine foot care Dental care (Adult)Non-emergency care when traveling outsidethe U.S. Weight Loss Programs Other Covered Services (Limitations may apply to these services. This isn’t a complete list. Please see your plan document.) Bariatric surgery (requires pre-approval) Chiropractic care (limited to 20 visits/year) Hearing Aids (Only covered for members age15 or younger)* For more information about limitations and exceptions, see the plan or policy document athttp://www.nj.gov/treasury/pensions/index.shtml Infertility treatment (requires pre-approval) Routine eye care (Adult)5 of 8
Your Rights to Continue Coverage:There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agencies is: the plan at 1-800-4147427 (SHBP), the Department of Health and Human Services, Center for Consumer Information and Insurance Oversight, at 1-877-267-2323 x61565 orwww.cciio.cms.gov, or the U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa. Othercoverage options may be available to you, too, including buying individual insurance coverage through the Health Insurance Marketplace. For moreinformation about the Marketplace, visit www.getcovered.nj.gov or call 1-877-962-8448.Your Grievance and Appeals Rights:There are agencies that can help if you have a complaint against your plan for a denial of a claim. This complaint is called a grievance or appeal. For moreinformation about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents also provide completeinformation to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance,contact: Horizon Blue Cross Blue Shield of New Jersey Member Services at 1-800-414-SHBP (7427). You may also contact the Department of Labor’sEmployee Benefits Security Administration at 1-866-444-EBSA (3272) or www.dol.gov/ebda/healthreform.Does this plan provide Minimum Essential Coverage? YesMinimum Essential Coverage generally includes plans, health insurance available through the Marketplace or other individual market policies, Medicare,Medicaid, CHIP, TRICARE, and certain other coverage. If you are eligible for certain types of Minimum Essential Coverage, you may not be eligible for thepremium tax credit.Does this plan meet the Minimum Value Standards? YesIf your plan doesn’t meet the Minimum Value Standards, you may be eligible for a premium tax credit to help you pay for a plan through ------To see examples of how this plan might cover costs for a sample medical situation, see the next ---* For more information about limitations and exceptions, see the plan or policy document athttp://www.nj.gov/treasury/pensions/index.shtml6 of 8
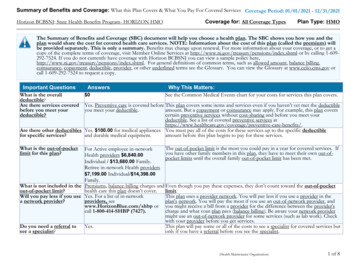
About these Coverage Examples:This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs willbe different depending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the costsharing amounts (deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to comparethe portion of costs you might pay under different health plans. Please note these coverage examples are based on self-only coverage.Peg is Having a Baby(9 months of in-network pre-natal careand a hospital delivery) The plan’s overall deductibleSpecialist CopaymentHospital (facility) CoinsuranceOther Coinsurance 0.00 10.000%0%This EXAMPLE event includes services like:Specialist office visits (prenatal care)Childbirth/Delivery Professional ServicesChildbirth/Delivery Facility ServicesDiagnostic tests (ultrasounds and blood work)Specialist visit (anesthesia)Total Example CostIn this example, Peg would pay:Cost SharingDeductiblesCopaymentsCoinsuranceWhat isn’t coveredLimits or exclusionsThe total Peg would pay is 12,700.00 0.00 10.00 0.00 70.00 80.00Managing Joe’s type 2 Diabetes(a year of routine in-network care of awell-controlled condition) The plan’s overall deductibleSpecialist CopaymentHospital (facility) CoinsuranceOther Coinsurance 0.00 10.000%0%This EXAMPLE event includes services like:Primary care physician office visits (includingdisease education)Diagnostic tests (blood work)Prescription drugsDurable medical equipment (glucose meter)Total Example CostIn this example, Joe would pay:Cost SharingDeductiblesCopaymentsCoinsuranceWhat isn’t coveredLimits or exclusionsThe total Joe would pay is 5,600.00 100.00 100.00 0.00 3,500.00 3,700.00Mia’s Simple Fracture(in-network emergency room visit andfollow up care) The plan’s overall deductibleSpecialist CopaymentHospital (facility) CoinsuranceOther Coinsurance 0.00 10.000%0%This EXAMPLE event includes services like:Emergency room care (including medical supplies)Diagnostic test (x-ray)Durable medical equipment (crutches)Rehabilitation services (physical therapy)Total Example Cost 2,800.00In this example, Mia would pay:Cost SharingDeductiblesCopaymentsCoinsuranceWhat isn’t coveredLimits or exclusionsThe total Mia would pay is 100.00 200.00 0.00 10.00 310.00Please note that some of the Limits or Exclusions listedabove may be covered under the Prescription Plan.This plan has other deductibles for specific services included in this coverage example. See "Are there other deductibles for specific services?" row above.The plan would be responsible for the other costs of these EXAMPLE covered services.* For more information about limitations and exceptions, see the plan or policy document athttp://www.nj.gov/treasury/pensions/index.shtml7 of 8
* For more information about limitations and exceptions, see the plan or policy document athttp://www.nj.gov/treasury/pensions/index.shtml8 of 8
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services Coverage Period: 01/01/2021 - 12/31/2021 Horizon BCBSNJ: State Health Benefits Program- HORIZON HMO Coverage for: All Coverage Types Plan Type: HMO (Health Maintenance Organization) 1 of 8 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan.