Transcription
The Pediatrics Subspecialty Milestone ProjectAdolescent MedicineChild AbuseDevelopmental-Behavioral PediatricsNeonatal-PerinatalPediatric CardiologyPediatric Critical CarePediatric EndocrinologyPediatric GastroenterologyPediatric Hematology OncologyPediatric Hospital MedicineJoint Initiative ofPediatric Infectious DiseasesPediatric NephrologyPediatric PulmonologyPediatric RheumatologyPediatric Transplant HepatologyThe Accreditation Council for Graduate Medical EducationandThe American Board of PediatricsJuly 2015
The Pediatrics Subspecialty Milestone ProjectThe Milestones are designed only for use in assessment of fellow in the context of their participation in ACGME-accreditedresidency or fellowship programs. The Milestones, in the context of the entrustable professional activities (EPAs) identifiedfor a given subspecialty practice, provide a framework for the assessment of the development of fellows in key dimensions ofthe elements of physician competency in a subspecialty. They neither represent the entirety of the dimensions of the sixdomains of physician competency, nor are they designed to be relevant in any other context.i
Pediatrics Milestones Working GroupPediatrics Milestones Advisory GroupChair: Carol Carraccio, MD, MACarol Aschenbrener, MDBradley Benson, MDRichard Behrman, MDAnn Burke, MDTimothy Brigham, MDiv, PhDRobert Englander, MD, MPHStephen Clyman, MDSusan Guralnick, MDEric Holmboe, MDPatricia Hicks, MD, MHPEM. Douglas Jones Jr., MDStephen Ludwig, MDGail McGuinness, MDDaniel Schumacher, MDVictoria Norwood, MDJerry Vasilias, PhDRobert Perelman, MDWilliam Raszka, MDTheodore Sectish, MDSusan Swing, PhDPediatrics Subspecialty Milestones Advisory GroupCarol Carraccio, MDJoseph Gilhooly, MDRichard Mink, MDii
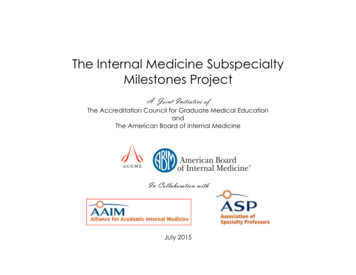
Milestone ReportingThis document presents milestones designed for programs to use in semi-annual review of fellow performance and reporting to the ACGME.Milestones are knowledge, skills, attitudes, and other attributes for each of the ACGME competencies organized in a developmental frameworkfrom less to more advanced. The Pediatrics Subspecialty Milestones are designed to describe changes in observable attributes of the learneracross the continuum of medical education from residency through fellowship into practice. In the initial years of implementation, the ReviewCommittee will examine Milestone performance data for each program’s fellows as one element in the Next Accreditation System (NAS) todetermine whether fellows overall are progressing.For each reporting period, review and reporting will involve selecting the level of milestones that best describes each fellow’s currentperformance level in relation to those milestones. Milestones are arranged into levels (see the figure on page iv). Progressing from Level 1 toLevel 5 is synonymous with moving from novice to expert in the subspecialty. Selection of a level implies that the fellow substantiallydemonstrates the milestones in that level, as well as those in lower levels.Additional NotesLevel 4 is designed as the graduation target but does not represent a graduation requirement. Making decisions about readiness for graduationis the purview of the residency program director (See the Milestones FAQ for further discussion of this issue: “Can a resident/fellow graduate ifhe or she does not reach every milestone?”). Study of Milestone performance data will be required before the ACGME and its partners will beable to determine whether Level 4 milestones and milestones in lower levels are in the appropriate level within the developmental framework,and whether Milestone data are of sufficient quality to be used for high stakes decisions.Answers to Frequently Asked Questions about Milestones are available on the Milestones web tonesFAQ.pdf.A full report on the Pediatrics Milestone Project, including background information on each set of Milestones, is located estones/320 PedsMilestonesProject.pdfiii
The figure below presents an example set of milestones for one sub-competency in the same format as the Milestone Report Worksheet. Foreach reporting period, a fellow’s performance on the milestones for each sub-competency will be indicated by: selecting the level of milestones that best describes that fellow’s performance in relation to those milestonesor selecting the “Not yet Assessable” response option. This option should be used only when a fellow has not yet had a learning experiencein the sub-competency.Selecting a response box in the middle of alevel implies that milestones in that level andin lower levels have been substantiallydemonstrated.Selecting a response box on the line in between levelsindicates that milestones in lower levels have beensubstantially demonstrated as well as some milestonesin the higher level(s).iv
Version 1/2014PEDIATRICS SUBSPECIALTY MILESTONESACGME Report WorksheetPC1. Provide transfer of care that ensures seamless transitionsNot yetAssessableLevel 1Level 2Demonstrates variability intransfer of information(content, accuracy, efficiency,and synthesis) from one patientto the next; makes frequenterrors of both omission andcommission in the hand-offUses a standard templatefor the informationprovided during the handoff; is unable to deviatefrom that template toadapt to more complexsituations; may have errorsof omission or commission,particularly when clinicalinformation is notsynthesized; neitheranticipates nor attends tothe needs of the receiverof informationLevel 3Adapts and applies astandardized template,relevant to individualcontexts, reliably andreproducibly, with minimalerrors of omission orcommission; allows ampleopportunity forclarification and questions;is beginning to anticipatepotential issues for thetransfereeLevel 4Adapts and applies astandard template toincreasingly complexsituations in a broadvariety of settings anddisciplines; ensures opencommunication, whetherin the receiver- or theprovider-of-informationrole, through deliberativeinquiry, including readbacks, repeat-backs(provider), and clarifyingquestions (receivers)Level 5Adapts and applies thetemplate without errorand regardless of setting orcomplexity; internalizesthe professionalresponsibility aspect ofhand-off communication,as evidenced by formal andexplicit sharing of theconditions of transfer (e.g.,time and place) andcommunication of thoseconditions to patients,families, and othermembers of the healthcare teamComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.1
Version 1/2014PC2. Make informed diagnostic and therapeutic decisions that result in optimal clinical judgmentNot yetAssessableLevel 1Level 2Level 3Level 4Recalls and presents clinicalfacts in the history and physicalin the order they were elicitedwithout filtering,reorganization, or synthesis;demonstrates analyticreasoning through basicpathophysiology results in a listof all diagnoses consideredrather than the development ofworking diagnosticconsiderations, making itdifficult to develop atherapeutic planFocuses on features of theclinical presentation,making a unifying diagnosiselusive and leading to acontinual search for newdiagnostic possibilities;largely uses analyticreasoning through basicpathophysiology indiagnostic and therapeuticreasoning; oftenreorganizes clinical facts inthe history and physicalexamination to help decideon clarifying tests to orderrather than to develop andprioritize a differentialdiagnosis, often resultingin a myriad of tests andtherapies and unclearmanagement plans, sincethere is no unifyingdiagnosisAbstracts and reorganizeselicited clinical findings inmemory, using semanticqualifiers (such as pairedopposites that are used todescribe clinicalinformation [e.g., acuteand chronic]) to compareand contrast the diagnosesbeing considered whenpresenting or discussing acase; shows theemergence of patternrecognition in diagnosticand therapeutic reasoningthat often results in a wellsynthesized and organizedassessment of the focuseddifferential diagnosis andmanagement planReorganizes and storesclinical information (illnessand instance scripts) thatlead to early directeddiagnostic hypothesistesting with subsequenthistory, physicalexamination, and testsused to confirm this initialschema; demonstrateswell-established patternrecognition that leads tothe ability to identifydiscriminating featuresbetween similar patientsand to avoid prematureclosure; Selects therapiesthat are focused and basedon a unifying diagnosis,resulting in an effectiveand efficient diagnosticwork-up and managementplan tailored to addressthe individual patientLevel 5Current literature doesnot distinguish betweenbehaviors of proficientand expert practitioners.Expertise is not anexpectation of GMEtraining, as it requiresdeliberate practice overtimeComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.2
Version 1/2014PC3. Develop and carry out management plansNot yetAssessableLevel 1Develops and carries outmanagement plans based ondirectives from others, eitherfrom the health careorganization or the supervisingphysician; is unable to adjustplans based on individualpatient differences orpreferences; communicationabout the plan is unidirectionalfrom the practitioner to thepatient and familyLevel 2Develops and carries outmanagement plans basedon one’s theoreticalknowledge and/ordirectives from others; canadapt plans to theindividual patient, but onlywithin the framework ofone’s own theoreticalknowledge; is unable tofocus on key information,so conclusions are oftenfrom arbitrary, poorlyprioritized, and timelimited informationgathering; developsmanagement plans basedon the framework of one’sown assumptions andvaluesLevel 3Develops and carries outmanagement plans basedon both theoreticalknowledge and someexperience, especially inmanaging commonproblems; follows healthcare institution directivesas a matter of habit andgood practice rather thanas an externally imposedsanction; is able to moreeffectively and efficientlyfocus on key information,but still may be limited bytime and convenience;begins to incorporatepatients’ assumptions andvalues into plans throughmore bidirectionalcommunicationLevel 4Level 5Develops and carries outmanagement plans basedmost often on experience;effectively and efficientlyfocuses on key informationto arrive at a plan;incorporates patients’assumptions and valuesthrough bidirectionalcommunication with littleinterference from personalbiasesDevelops and carries outmanagement plans, evenfor complicated or raresituations, based primarilyon experience that putstheoretical knowledge intocontext; rapidly focuses onkey information to arriveat the plan and augmentsthat with availableinformation or seeks newinformation as needed; hasinsight into one’s ownassumptions and valuesthat allow one to filterthem out and focus on thepatient/family values in abidirectional conversationabout the managementplanComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.3
Version 1/2014PC4. Provide appropriate role modelingNot yetAssessableLevel 1Level 2Level 3Level 4Level 5Performs routine duties andbehaviors of profession withoutawareness of the impact onthose around him or her; mayor may not reflect on actions asthey occur (reflection in action)and does not share reflectionswith othersInconsistently aware of theimpact of one’s behaviorsand attitudes on others;sometimes teaches byexample; occasionally willreflect openly on events asthey occur (reflection inaction) and privately onevents that have alreadytaken place (reflection onaction)Conscious of being a rolemodel during manyinteractions; frequentlyteaches by example andoften reflects in actionopenly in the presence oflearners; behavior changeimplies frequentprivate reflection on actionConscious of being a rolemodel during mostinteractions; routinelyteaches by example;regularly reflects in actionand frequently reflects onaction, sharing this analysisof practice with learnersRole modeling is a habit;recognizes that he or she isa role model in all actionsand behaviors at alltimes; characteristicallyteaches by example;routinely reflects both inaction and on action;examines, analyzes, andexplains actions/behaviorsin the presence of learnersand colleaguesComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.4
Version 1/2014MK1. Locate, appraise, and assimilate evidence from scientific studies related to their patients’ health problemsNot yetAssessableLevel 1Level 2Level 3Level 4Level 5Explains basic principles ofEvidence-based Medicine(EBM), but relevance is limitedby lack of clinical exposureRecognizes the importanceof using currentinformation to care forpatients and responds toexternal prompts to do so;is able to formulatequestions with somedifficulty, but is not yetefficient with onlinesearching; is starting tolearn critical appraisal skillsAble to identify knowledgegaps as learningopportunities; makes aneffort to ask answerablequestions on a regularbasis and is becomingincreasingly able to do so;understands varying levelsof evidence and can utilizeadvanced search methods;is able to critically appraisea topic by analyzing themajor outcomes, however,may need guidance inunderstanding thesubtleties of the evidence;begins to seek and applyevidence when needed,not just when assigned todo soIs increasingly selfmotivated to learn more,as exhibited by regularlyformulating answerablequestions; incorporatesuse of clinical evidence inrounds and teaches fellowlearners; is quite capablewith advanced searching;is able to critically appraisetopics and does soregularly; shares findingswith others to try toimprove their abilities;practices EBM because ofthe benefit to the patientand the desire to learnmore rather than inresponse to externalpromptsTeaches critical appraisalof topics to others; strivesfor change at theorganizational level asdictated by best currentinformation; is able toeasily formulateanswerable clinicalquestions and does so withmajority of patients as ahabit; is able to effectivelyand efficiently search andaccess the literature; isseen by others as a rolemodel for practicing EBMExample:The senior fellow asks eachmember of the inpatient teamto answer a clinical questionthat he raised during roundsand to be prepared to discuss itthe next morning. The learnergoes to a more senior colleaguefor help, since he cannot workthrough a case or article usingthe critical appraisal approach,Example:In response to a clinicalquestion raised duringrounds and the seniorfellow’s request thateveryone answer thequestion, the learner isable, with some difficulty,to frame the question in In response to the clinicalquestion raised duringrounds, the learnerdevelops an answerableclinical question in PICOformat and efficientlysearches for best evidence.He volunteers to presenton rounds the next day anddemonstrates effectiveExample:In response to the clinicalquestion raised duringrounds, presents a secondquestion that he hasalready researched in aPICO format as well as acritique of the evidenceand its applicability to thecurrent patient. He wasmotivated to be proactiveExample:Is an EBM practitioner, asobserved by conversationsduring rounds, whomothers try to emulate. Heenjoys teaching colleagueshow to become EBMpractitioners by rolemodeling. He helps teammembers develop andrefine their skills using hisCopyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.5
Version 1/2014mainly due to lack of clinicalcontext from which to work.(PICO) format. He hassearching capability, butthe search and the steps ofanalyzing and applying theevidence are timeintensive, so he is notprepared to discuss hisfindings on rounds the nextmorning.analytic skills and theability to apply his findingsto the current patient. Hehas a bit of difficultyinterpreting and applyingsome of the secondaryoutcomes and, in thecontext of this discussion,another question is raised,which he volunteers tosearch and answer.by his interest in learning,as well as the needs of hispatient. He shares histactics with team membersby teaching them the stepshe engaged in to learn andapply this information.expertise to make adifficult task practical anddoable.Comments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.6
Version 1/2014SBP1. Work effectively in various health care delivery settings and systems relevant to their clinical specialtyNot yetAssessableLevel 1Level 2With limited knowledge ofsystems, focuses on the“pieces” of a process ratherthan the whole; frequentlyfrustrated by the system’ssuboptimal processes, but lacksthe ability to identify the rootcause and thus to effect changeHas developed knowledgeof systems and thereforeunderstands when othersdescribe how the piecesrelate to the whole; notyet able to articulate thatrelationshipindependently, andtherefore develops workarounds when faced with asystems challengeLevel 3Competent in working invarious systems andsettings; therefore, able toapply knowledge, skills,and attitudes in systemsthinking to systems’problems within a givencontext; recognizes theneed to change systemsrather than develop workarounds, and can activatethe system to do so;however, does not applylearning from one settingor context to anotherLevel 4Capable in systemsthinking; therefore, hascompetence in systemsthinking and can adaptlearning from one systemor setting to another; inthis way, can effect orstimulate improvements ina system and does so whenthe need arisesLevel 5Capable, as defined inLevel 4, and viewsimproving systems of careas an integral componentof professional identity;leads systems changes aspart of the routine caredelivery processComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.7
Version 1/2014SBP2. Coordinate patient care within the health care system relevant to their clinical specialtyNot yetAssessableLevel 1Performs the role of medicaldecision-maker, developingcare plans and setting goals ofcare independently; informspatient/family of the plan, butno written care plan isprovided; makes referrals, andrequests consultations andtesting with little or nocommunication with teammembers or consultants; is notinvolved in the transition ofcare between settings (e.g.,outpatient and inpatient,pediatric and adult); showslittle or no recognition ofsocial/educational/culturalissues affecting thepatient/familyLevel 2Level 3Level 4Begins to involve thepatient/family in settingcare goals and some of thedecisions involved in thecare plan; a written careplan is occasionally madeavailable to thepatient/family; care plandoes not address keyissues; has variablecommunication with teammembers and consultantsregarding referrals,consultations, and testing;answers patient/familyquestions regarding resultsand recommendations;may inconsistently beinvolved in the transitionof care between settings(e.g., outpatient andinpatient, pediatric andadult); makes someassessment ofsocial/educational/culturalissues affecting thepatient/family and appliesthis in interactionsRecognizes theresponsibility to assistfamilies in navigation ofthe complex health caresystem; frequently involvespatient/family in decisionsat all levels of care, settinggoals, and defining careplans; frequently makes awritten care plan availableto the patient/family andto appropriatelyauthorized members of thecare team; care plan omitsfew key issues; has goodcommunication with teammembers and consultants;consistently discussesresults andrecommendations withpatient/family; is routinelyinvolved in the transitionof care between settings(e.g., outpatient andinpatient, pediatric andadult); considers social,educational and culturalissues in most careinteractionsActively assists families innavigating the complexhealth care system; hasopen communication,facilitating trust in thepatient-physicianinteraction; develops goalsand makes decisions jointlywith the patient/family(shared-decision-making);routinely makes a writtencare plan available to thepatient/family and toappropriately authorizedmembers of the care team;makes a thorough careplan, addressing all keyissues; facilitates carethrough consultation,referral, testing,monitoring, and follow-up,helping the family tointerpret and act onresults/recommendations;coordinates seamlesstransitions of carebetween settings (e.g.,outpatient and inpatient,pediatric and adult; mentaland dental health;education; housing; foodsecurity; family-to-familysupport); buildspartnerships that fosterLevel 5Current literature does notdistinguish betweenbehaviors of proficient andexpert practitioners.Expertise is not anexpectation of GMEtraining, as it requiresdeliberate practice overtimeCopyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.8
Version 1/2014family-centered, culturallyeffective care, ensuringcommunication andcollaboration along thecontinuum of careComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.9
Version 1/2014SBP3. Incorporate considerations of cost awareness and risk-benefit analysis in patient and/or population-based care as appropriateNot yetAssessableLevel 1Level 2Level 3Unaware of costs issues inevaluation and management ofpatients; has difficultyprocessing cost and risk-benefitinformation in a way thatresults in cost-containmentactions or appropriate riskbenefit analysis; frustrated bycost containment efforts thatare viewed as primarilyexternally mandatedUses externally providedinformation (e.g.,prescribing information,test ordering patterns, orresearch around atreatment) to inform costcontaining action and/orpreliminary risk-benefitanalysis; demonstratesinadequate skills in criticalappraisal that may result ininappropriate costcontainment activitiesand/or risk-benefitcounselingCritically appraisesinformation available onan evaluation test ortreatment to allowoptimization of cost issuesand risk-benefit for anindividual patient; adoptsstrategies that decreasecost and risk and optimizebenefits for individuals,with less attention to thoseoutcomes for populationsLevel 4Critically appraisesinformation in the contextof not only the individualpatient, but also thebroaderpopulation/system;ascribes value to cost andrisk-benefit decisionsbased on this broadunderstanding of theinformationLevel 5Consistently integratescost analysis into one’spractice while minimizingrisk and optimizingbenefits for whole systemsor populationsComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.10
Version 1/2014SBP4. Work in inter-professional teams to enhance patient safety and improve patient care qualityNot yetAssessableLevel 1Seeks answers and responds toauthority from only intraprofessional colleagues; doesnot recognize other membersof the interdisciplinary team asbeing important or makingsignificant contributions to theteam; tends to dismiss inputfrom other professionals asidefrom other physiciansLevel 2Level 3Is beginning to have anunderstanding of the otherprofessionals on the team,especially their uniqueknowledge base, and isopen to their input,however, still acquiesces tophysician authorities toresolve conflict andprovide answers in theface of ambiguity; is notdismissive of other healthcare professionals, but isunlikely to seek out thoseindividuals whenconfronted withambiguous situationsAware of the uniquecontributions (knowledge,skills, and attitudes) ofother health careprofessionals, and seekstheir input for appropriateissues, and as a result, is anexcellent team playerLevel 4Same as Level 3, but anindividual at this stageunderstands the broaderconnectivity of theprofessions and theircomplementary nature;recognizes that qualitypatient care only occurs inthe context of the interprofessional team; servesas a role model for othersin interdisciplinary workand is an excellent teamleaderLevel 5Current literature does notdistinguish betweenbehaviors of proficient andexpert practitioners.Expertise is not anexpectation of GMEtraining, as it requiresdeliberate practice overtimeComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.11
Version 1/2014SBP5. Participate in identifying system errors and implementing potential systems solutionsNot yetAssessableLevel 1Defensive or blaming whenencountering medical error; noperception of personalresponsibility for individual orsystems error correction; notopen to discussion of error oridentification of the type oferror; approaches errorprevention from an individualcase perspective onlyLevel 2Level 3Level 4Occasionally open todiscussion of error withouta defensive or blamingapproach; some awarenessof personal responsibilityfor individual or systemserror correction; identifiesmedical error events, butcannot identify the type(active versus latent) oferror; begins to perceivethat error may be morethan the mistake of anindividualUsually open to adiscussion of error; activelyidentifies medical errorevents and seeks todetermine the type oferror; occasionallyidentifies the element ofpersonal responsibility forindividual or systems errorcorrection; seesexamination and analysisof error as an importantpart of the preventiveprocessUsually encourages openand safe discussion oferror; actively identifiesmedical error events;accepts personalresponsibility for individualor systems errorcorrection, regularlydetermining the type oferror and beginning toseek system causes oferrorLevel 5Consistently encouragesopen and safe discussionof error; characteristicallyidentifies and analyzeserror events, habituallyapproaching medical errorwith a system solutionmethodology; actively androutinely engaged withteams and processesthrough which systems aremodified to preventmedical errorComments:Copyright (c) Pending. The Accreditation Council for Graduate Medical Education and the American Board of Pediatrics. All rights reserved. The copyrightowners grant third parties the right to use the Pediatrics Subspecialty Milestones on a non-exclusive basis for educational purposes.12
Version 1/2014PBLI1. Identify strengths, deficiencies, and limits in one’s knowledge and expertiseNot yetAssessableLevel 1Level 2Level 3Level 4Level 5The learner acknowledgesexternal assessments, butunderstanding of hisperformance is superficial andlimited to the overall grade orbottom line; has littleunderstanding of how theperformance measure relatesin a meaningful way to hisspecific level of Knowledge,Skills and Attitudes (KSA)Assessment ofperformance is seen asbeing able to do or not dothe task at hand withoutappreciation for how wellit is done and whetherthere is a need to improvethe outcomePrompts for understandingspecifics of level ofperformance are internaland may be identified inresponse to uncertainty,discomfort, or tension incompleting clinical duties;evidence of this stage isdemonstrated by activequestioning andapplication of knowledgein developing a rationalefor care plans or inteaching activitiesPrompted by anticipationor contemplation ofpotential clinical problems,the learner self-identifiesgaps in KSA throughreflection that assessescurrent KSA versusunderstanding ofunderlying basic science orpathophysiologic principlesto generate new questionsabout limitations ormastery of KSA; evidenceof this stage can bedetermined by theadvanced nature and levelof questioning or resourceseekingPrompted by a selfdirected goal of improvingthe professional self, thepractitioner anticipateshypothetical clinicalscenarios that build oncurrent experience andsystematically addressesidentified g
Neonatal-Perinatal Pediatric Hematology Oncology Pediatric Rheumatology . Pediatric Cardiology Pediatric Hospital Medicine Pediatric Transplant Hepatology . Joint Initiative of . The Accreditation Council for Gradua te Medical Education . and . The American Board of Pediatrics