Transcription
Fluid Managementand DehydrationNational Pediatric Nighttime CurriculumWritten by Dr. Mitzi Scotten, Dr. Nidal El-Wiher,Dr. Gunjeet KalaUniversity of Kansas Medical Center
Learning Objectives Calculatemaintenance fluidrequirements based on anunderstanding of body watercomposition and electrolyte physiology Identify symptoms of dehydration andcalculate degree of deficit Identify electrolyte composition ofdifferent body fluids andcorresponding replacement fluid type
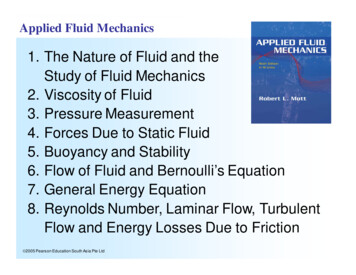
Total Body Water Composition Regulated by Antidiuretic hormone (ADH)and aldosteroneAre secreted in reactionchanges in bloodvolumeDisturbances in eitherADH or aldosterone willcause large effects onwater homeostasis
Electrolyte Composition of Intraand Extracellular Fluids Sodium is thepredominant cation in theextracellular spaceAlterations in sodiumconcentrations can havesignificant effects onwater homeostasisPotassium is thepredominant intracellularcationMedical conditions anddrugs can causemovement in potassiumfrom the intracellular toextracellular space
Intravenous Fluid ½ NormalSaline(0.45%)77meq77meq1/4 09meqKCaLactate4meq3meq28meq
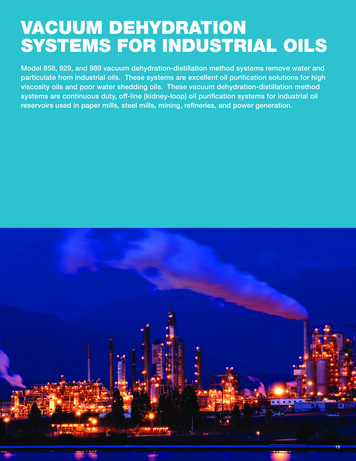
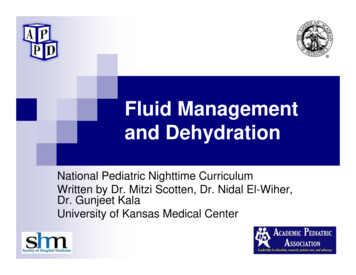
OsmolalityOsmolality 2 [Na] [glucose]/18 [BUN]/2.8 Measure of solute particlesper weight of solventNormal ranges are 280-295mOsm/kilogramWater shifts from a low tohigh osmolality in the bodyRapid shifts adversely effectthe central nervous systemmore than the rest of the bodyas seen to the right withcentral pontine myelinosis -
Goals of Maintenance FluidsFluid Goals Prevent DehydrationPrevent ElectrolyteDisordersPrevent Ketoacidosis** Guidelines assume thatthere is no diseaseprocess present that wouldrequire an adjustment ineither the volume or theelectrolyte composition ofthe maintenance fluids Infants and childrenrequire more fluids per unitof body weight due to highmetabolic ratesMaintenance fluids shouldbe initiated for infants whoare required to go over 4hours without fluid intakeas occurs prior to surgeryand proceduresMaintenance fluids replacethe daily loss of: urine stool insensible losses
Maintenance IV Fluids:Holliday Segar Method of CalculationWhat to run? 10kg: D5 ¼ NS 10meqKCl/L 10kg:D5 ½ NS 20meq KCl/LHow much ml/day?1st 10 kg: 100ml/kg2nd 10 kg: 50ml/kgkg 20kg: 20ml/kgHow fast ml/hr?1st 10 kg: 4ml/kg2nd 10 kg: 2ml/kgkg 20 kg: 1ml/kg
Maintenance IVF Practice:Write hourly rates foreach patient weight8 kg 10kg 15kg 80kg 8 x 4 32cc per hour- D5 1/410 x 4 40cc per hour- either ½ or1/410x 4 5 x 2 (40 10) 50cc/hr- D5 ½10x 4 10x 2 60x 1 (40 20 60) 120ccNote- 120cc is maximal rate for normalmaintenanceIn oncology patients meters squared is used inlieu of kilograms
Clinical Picture of DehydrationSigns &SymptonsMild 3-5%Moderate 6-9%Severe 10%GeneralThirsty, restless, DrowsyalertDrowsy, limp,cold, mottledPeripheralpulsesNormalRapid and weakRapid, threadyBreathingNormalDeep, rapidDeep, rapidFontanelleNormalSunkenVery sunkenCapillary Refill 2 SecondsProlonged 3-4secVery prolonged 4 secMucousmembraneMoistDryVery dryBlood PressureNormalNormalHypotension
Fluid Resuscitation/Treatment ofDehydration For dehydration,shock,blood loss-isotonicNormal Saline or Lactated RingersGive 20ml/kg as bolus .then repeat your examRepeat bolus if symptoms of dehydration are still presentAfter patient shows improvement you can change toglucose containing IV fluidsCalculate fluid need based on degree of dehydration andcover for 24 hoursConsider Colloid for large blood loss or greater than 3boluses of 20cc/kg
Electrolyte Composition of BodyFluidsFluidReplacement of ongoing Replacement ratefluid lossGastric fluidNa 60 meq/LK 10 meq/LCl 90 meq/LNormal Saline 10meq KCL/Literml/ml every 1-6 hoursDiarrheaNa 55meq/LK 25meq/LHCO3 meq15/LD5 ¼ NS NaHCO3 20 meq/L KCL 20 meq/Lml/ml every 1-6 hours
Intern CaseHistoryYou are receiving an admissionfrom the same day sick clinic. Itis a 2 month old with vomitingand diarrhea for 3 days. Failedoral rehydration therapy due tovomiting. Two days ago thepatient was seen for the samesymptoms- weight at that timewas 5500 grams. Today you aretold the weight is 5000 grams.Questions1. What is the degree ofdehydration?2. What would be the fluid deficit ofthis child in cc?3. What is the maintenance IV rate?4. What would be your initial fluidorder?5. What vital signs would youexpect initially?6. Write admission orders for thischild
Senior Level CaseYou are covering the oncologyservice overnight. A nurse callsto report that a 2 year old withrecently diagnosed ALL has noturinated for 8 hours. He hasbeen on no IV fluids and hasoral lesions due to recentchemotherapy.This child has Down’s Syndromeand a “large” VSD and is onlasix and digoxin. You have norecent laboratory work available.What potential electrolyteabnormalities do you expecton a chemistry?What underlying pathology inthis child could causepotential complications influid resuscitation?What would be your initial fluidorder to the nurse and why?What physical exam findingswould be helpful in yourdecision?What ominous physical signswould you look for afterinitial treatment?
Take Home Points! Maintenance fluid calculations are based onthe composition of maintenance water anduse the Holiday Segar, or 4:2:1 methodDehydration can be a medical emergency.Identification of the degree of deficit is basedon patient history and physical signs onexam. Fluid resuscitation should be withisotonic fluid.Correction of ongoing fluid losses is basedon the body fluid lost and should be addedto maintenance fluid requirements
Bibliography 1. Perkin R., Swift J., Newton D., Anas N. Pediatric Hospital Medicine:Textbook of Inpatient Management Second Edition. WoltersKluwer;20082. Zaoutis L., Chiang V. Comprehensive Pediatric Hospital Medicine.Mosby;20073. Pediatric Hospital Medicine Core Competencies
Maintenance fluid calculations are based on the composition of maintenance water and use the Holiday Segar, or 4:2:1 method Dehydration can be a medical emergency. Identification of the degree of deficit is based on patient history and physical signs on exam. Fluid resuscitation should be with isotonic fluid.