Transcription
Slide TemplateAssessing your Meaningful UseStage Compliance as you Preparefor Stage 2West Coast RegionalAnnual ConferenceJune 17, 2011Session Objectives Success strategies for achieving Stage 1 Define the key playersReporting matrixGap analysisMitigation strategiesManaging the project to meet the timelineIdentify the role of Compliance in the MeaningfulUse initiative.How organizations can leverage theirimplementation efforts to satisfy broadercompliance and quality improvementefforts.1
Slide TemplateAudience Question #1What is your role with EMR transitionat your organization?*1 Subject Matter Expert; or Other*2 Assigned to formal project team*3 Strategic Leadership relatedStage 1 – Infancy – Don’t be fooledMeaningfulUse2
Slide TemplateMeaningful Use Stage 11.Use of certified EHR technology in a meaningful manner(e.g. e-Prescribing)2.Electronic exchange of health information to improvequality of care3.Report clinical quality measures using certified EHRtechnology CORE Set – 15 mandatory objectivesMenu Set – Pick 5 of 10 objectives“It’s not so much reporting that’s the challenge, it’s getting the data to report” Erica DrazenManaging Director/Emerging PracticesComputer Sciences CorporationMeasures Requiring Compliance InvolvementStage 1 FinalRuleProposed Stage 2Proposed Stage 3CommentsDrug-drug/drugallergy interactionchecksEmploy drug-druginteraction checkingand drug allergychecking onappropriate evidencebased interactionsReporting of druginteraction checks to bedefined by qualitymeasures workgroupCPOE formedication orders(30%)CPOE (by licensedprofessional) for atleast 1 medication, and1 lab or radiology orderfor 60% of uniquepatients who have atleast 1 such order(order does not have tobe transmittedelectronically)Employ drug-druginteraction checking, drugallergy checking, drug agechecking (medications inthe elderly), drug dosechecking (e.g., pediatricdosing, chemotherapydosing), drug lab checking,and drug conditionchecking (includingpregnancy and lactation)on appropriate evidencebased interactionsCPOE (by licensedprofessional) for at least 1medication, and 1 lab orradiology order on 80% ofpatients who have at least1 such order (order doesnot have to be transmittedelectronically)3
Slide TemplateMeasures Requiring Compliance InvolvementMaintain problemlist (80%)Continue Stage 180% problem lists areup-to-dateExpect to drive list tobe up-to-date bymaking it part ofpatient visit summaryand care plansMaintain activemed list (80%)Continue Stage 180% medication lists areup-to-dateMaintain activemedication allergylist (80%)Continue Stage 180% medication allergylists are up-to-dateExpect to drive list tobe up-to-date viamedicationreconciliationExpect to drive the listto be up-to-date bymaking it part of visitsummaryRecord vital signs(50%)80% of uniquepatients have vitalsigns recorded80% of unique patientshave vital signs recordedRecord smokingstatus (50%)80% of unique90% of unique patientspatients have smoking have smoking statusstatus recordedrecordedMeasures Requiring Compliance InvolvementImplement 1 CDS ruleUse CDS to improveperformance on highpriority health conditions.Establish CDS attributesfor purposes ofcertification: 1.Authenticated (sourcecited); 2. Credible,evidence-based; 3.Patient-context sensitive;4. Invokes relevantknowledge; 5. Timely; 6.Efficient workflow; 7.Use CDS to improveperformance on high-priorityhealth conditions.Establish CDS attributes forpurposes of certification: 1.Authenticated (source cited);2. Credible, evidence-based;3. Patient-context sensitive;4. Invokes relevantknowledge; 5. Timely; 6.Efficient workflow; 7.Implement drugformulary checks*Move current measure tocore80% of medication ordersare checked against relevantformulariesWhat is the availability offormularies for eligibleprofessionals?Record existence ofadvance directives(EH) (50%)*Make core requirement.For EP and EH: 50% ofpatients 65 years oldhave recorded in EHR theresult of an advancedirective discussion andthe directive itself if itexistsFor EP and EH: 90% ofpatients 65 years old haverecorded in EHR the result ofan advance directivediscussion and the directiveitself if it existsPotential issues include:state statutes; challengesin outpatient settings;age; privacy; specialists;needs to be accessibleand certifiable; need todefine a standard4
Slide TemplateMeasures Requiring Compliance InvolvementStage 1 Final RuleProposed Stage 2Proposed Stage 3CommentsProvide electroniccopy of healthinformation, uponrequest (50%)Continue Stage 190% of patients have timelyaccess to copy of healthinformation from electronichealth record, upon requestOnly applies toinformation alreadystored in the EHRProvide electroniccopy of dischargeinstructions (EH) atdischarge (50%)Electronic dischargeinstructions for hospitals(which are given as thepatient is leaving thehospital) are offered to atleast 80% of patients(patients may elect toreceive only a printedcopy of the instructions)Electronic dischargeinstructions for hospitals(which are given as thepatient is leaving the hospital)are offered to at least 90% ofpatients in the commonprimary languages (patientsmay elect to receive only aprinted copy of theinstructions)Electronic dischargeinstructions shouldinclude a statement of thepatient’s condition,discharge medications,activities and diet, followup appointments, pendingtests that require followup, referrals, scheduledtests [we invitecomments on theelements listed above]EHR-enabled patientspecific educationalresources (10%)Continue Stage 120% offered patient-specificeducational resources onlinein the common primarylanguagesMeasures Requiring Compliance InvolvementStage 1 Final RuleProposed Stage 2Incorporate labresults as structureddata (40%)*Move current measure tocore, but only whereresults are available90% of lab resultselectronically ordered by EHRare stored as structured datain the EHR and are reconciledwith structured lab orders,where results and structuredorders availableGenerate patientlists for specificconditions*Make corerequirement.Generate patient listsfor multiple patientspecific parametersMake corerequirement.Patient lists are used tomanage patients forhigh-priority healthconditions20% of active patientswho prefer to receivereminders electronicallyreceive preventive orfollow-up remindersHow should ―activepatientǁ be defined?30% of visits have atleast one electronicEP note90% of visits have atleast one electronic EPnoteCan be scanned,narrative, structured,etc.Send patientreminders (20%)*(NEW)Proposed Stage 3Comments5
Slide TemplateMeasures Requiring Compliance InvolvementStage 1 Final RuleProposed Stage 2Proposed Stage 3(NEW for EH)80% of patients offered theability to view and downloadvia a web-based portal, within36 hours of discharge, relevantinformation contained in therecord about EH inpatientencounters. Data are availablein human-readable andstructured forms (HITSC todefine).80% of patients offered the abilityto view and download via a webbased portal, within 36 hours ofdischarge, relevant informationcontained in the record about EHinpatient encounters. Data areavailable in human readable andstructured forms (HITSC to define).Provide clinicalsummaries for each officevisit (EP) (50%)Patients have the ability toview and download relevantinformation about a clinicalencounter within 24 hours ofthe encounter. Follow-up teststhat are linked to encounterorders but not ready during theencounter should be includedin future summaries of thatencounter, within 4 days ofbecoming available. Data areavailable in human-readableand structured forms (HITSC todefine)Patients have the ability to view anddownload relevant informationabout a clinical encounter within 24hours of the encounter. Follow-uptests that are linked to encounterorders but not ready during theencounter should be included infuture summaries of thatencounter, within 4 days ofbecoming available. Data areavailable in human readable andstructured forms (HITSC to define)CommentsInpatient summaries include:hospitalization admit anddischarge date and location;reason for hospitalization;providers; problem list;medication lists; medicationallergies; procedures;immunizations; vital signs atdischarge; diagnostic test results(when available); dischargeinstructions; care transitionssummary and plan; dischargesummary (when available);gender, race, ethnicity, date ofbirth; preferred language;advance directives; smokingstatus. [we invite comments onthe elements listed above]The following encounter data areincluded (where relevant):encounter date and location;reasons for encounter; provider;problem list; medication list;medication allergies; procedures;immunizations; vital signs;diagnostic test results; clinicalinstructions; orders: futureappointment requests, referrals,scheduled tests; gender, race,ethnicity, date of birth; preferredlanguage; advance directives;smoking status. [we invitecomments on the elements listedabove]Measures Requiring Compliance InvolvementStage 1 Final RuleProposed Stage 2Proposed Stage 3CommentsProvide timely electronicaccess (EP) (10%)Patients have the ability to viewand download (on demand)relevant information containedin the longitudinal record,which has been updated within4 days of the information beingavailable to the practice.Patient should be able to filteror organize information by date,encounter, etc. Data areavailable in human-readableand structured forms (HITSC todefine).Patients have the ability to view anddownload (on demand) relevantinformation contained in thelongitudinal record, which has beenupdated within 4 days of theinformation being available to thepractice. Patient should be able tofilter or organize information bydate, encounter, etc. Data areavailable in human readable andstructured forms (HITSC to define).The following data elementsare included: encounter datesand locations; reasons forencounters; providers; problemlist; medication list; medicationallergies; procedures;immunizations; vital signs;diagnostic test results; clinicalinstructions; orders;longitudinal care plan; gender,race, ethnicity, date of birth;preferred language; advancedirectives; smoking status. [weinvite comments on theelements listed above]This objective sets themeasures for ―Providetimely electronic access(EP)ǁ and for ―Provideclinical summaries for eachoffice visit (EP)ǁEPs: 20% of patients use aweb-based portal to accesstheir information (for anencounter or for thelongitudinal record) at leastonce. Exclusions: patientswithout ability to access theInternetEPs: 30% of patients use a webbased portal to access theirinformation (for an encounter or forthe longitudinal record) at leastonce. Exclusions: patients withoutability to access the Internet(NEW)EPs: online secure patientmessaging is in useEPs: online secure patientmessaging is in use6
Slide TemplateNew Measure: Communication PreferencesStage 1 Final RuleProposed Stage 2Proposed Stage 3Comments(NEW)Patient preferences forcommunication mediumrecorded for 20% of patientsPatient preferences forcommunication medium recordedfor 80% of patientsHow should ―communicationmediumǁ be delineated?Offer electronic self-managementtools to patients with high priorityhealth conditionsWe are seeking comment onwhat steps will be needed instage 2 to achieve thisproposed stage 3 objectiveEHRs have capability to exchangedata with PHRs using standardsbased health data exchangeWe are seeking comment onwhat steps will be needed instage 2 to achieve thisproposed stage 3 objectivePatients offered capability toreport experience of caremeasures onlineWe are seeking comment onwhat steps will be needed instage 2 to achieve thisproposed stage 3 objectiveOffer capability to upload andincorporate patient-generateddata (e.g., electronically collectedpatient survey data, biometrichome monitoring data, patientsuggestions of corrections toerrors in the record) into EHRs andclinician workflowWe are seeking comment onwhat steps will be needed instage 2 to achieve thisproposed stage 3 objectiveMeasures Requiring Compliance InvolvementStage 1 Final RuleProposed Stage 2Proposed Stage 3CommentsPerform test of HIEConnect to at least threeexternal providers in―primary referral networkǁ(but outside delivery systemthat uses the same EHR) orestablish an ongoingbidirectional connection to atleast one health informationexchangeConnect to at least 30% ofexternal providers in ―primaryreferral networkǁ or establish anongoing bidirectional connectionto at least one health informationexchangeSuccessful HIE will requiredevelopment and use ofinfrastructure like entitylevel provider directories(ELPD)Perform medicationreconciliation (50%)*Medication reconciliationconducted at 80% of caretransitions by receivingprovider (transitions fromanother setting of care, orfrom another provider ofcare, or the provider believesit is relevant)Medication reconciliationconducted at 90% of caretransitions by receiving providerProvide summary of carerecord (50%)*Move to CoreSummary care record providedelectronically for 80% oftransitions and referrals7
Slide TemplateMeasures Requiring Compliance InvolvementStage 1 Final RuleProposed Stage 2Proposed Stage 3CommentsSubmit immunizationdata*EH and EP: Mandatory test.Some immunizations aresubmitted on an ongoingbasis to ImmunizationInformation System (IIS), ifacceptedand as required by lawEH and EP: Mandatory test.Immunizations are submitted toIIS, if accepted and as requiredby law. During well child/adultvisits, providers review IISrecords via their EHR.Stage 2 implies at leastsome data is submitted toIIS. EH and EP may choosenot, for example, to senddata through IIS todifferent states in Stage 2.The goal is to eventuallyreview IIS-generatedrecommendationsSubmit reportable labdata*EH: move Stage 1 to coreEP: lab reporting menu. ForEPs, ensure that reportablelab results and conditionsare submitted to publichealth agencies eitherdirectly or through theirperforming labs (if acceptedand as required by law).Mandatory test.EH: submit reportable lab resultsand reportable conditions ifaccepted and as required by law.Include complete contactinformation (e.g., patientaddress, phone and municipality)in 30% (EH) of reports.EP: ensure that reportable labresults and reportable conditionsare submitted to public healthagencies either directly orthrough performing labs (ifaccepted and as required by law)Submit syndromicsurveillance data*Move to core.Mandatory test; submit ifacceptedMeasures Requiring Compliance InvolvementStage 1 Final RuleConduct securityreview analysis &correct deficienciesProposed Stage 2Proposed Stage 3CommentsAdditional privacy andsecurity objectives underconsideration via the HITPolicy Committee’sPrivacy & Security TigerTeam8
Slide TemplateMeaningful Use: New/Emerging RolesVanderbilt University Medical Center -Nashville, TNPhysician EducatorStructured electronic template development to support: ICD-9 & 10 specificity Meaningful Use Medical Necessity Co-morbids and complications Present on Admission Severity of Illness Risk of Mortality “By focusing on ‘meaningful use,’ we recognize that better healthcaredoes not come solely from the adoption of technology itself, butthrough the exchange and use of health information to best informclinical decisions at the point of care.” David Blumenthal, National CoordinatorKey Considerations Problem List Management Accurate and standardization of the problem list can yield the mostprecise information for decision support, clinical care, coding and billingStrive for uniformity/standardization by practiceChallenges with adoption Defining/refining responsibility of maintenanceComplexity of integrated health networks with a shared EMR impactsscope EMR GovernanceTools to assist with problem capture – SNOMED CT – ICD-9 (picklist),complexity increases with ICD-10Solutions Consider PCP accountability for maintenance of accurate problem lists;with ability for Specialists to provide recommended additions Create and implement new policy Identify technology solutions to accomplish accurate capture9
Slide TemplateKey Considerations (cont.) Reporting Assure ample resources Assess use of databases external to the EMR Use of separate, uncertified systems may be used to generatereports so long as the data is captured using certified EHRtechnology Meaningful Use Ownership/Governance Define how to drive MU Clarify roles/responsibilities within the organization As you navigate a hybrid system environment & review TechnologyInfrastructure: Consider how standalone systems, such as ROI, will be used inconjunction with a certified EMR Review hardware, training and security needed to provideelectronic PHI (e.g., discharge instructions) Explore opportunities to release to patient portal or PHRMeaningful Use TimelinesTimelinesStage 1Proposed RuleJan 2010Final RuleStage 1 Reporting forHospitalsJuly 2011July 2010 Oct 2010DevelopmentImplementationStage 1 Reportingfor EPsSome hospitals/EPs will take longer for implementation.Stage 2Proposed RuleFinal RuleStage 2 Reporting for HospitalsJan 2012July 2012 Oct 2012DevelopmentImplementationStage 2 Reporting for Eligible ProfessionalsSome hospitals/EPs will take longer for implementation.310
Slide TemplateMeaningful Use: Stage 2 –Are we having fun yet? Unreasonable timelines impact: EMR system development, testing andrelease Customer implementation timeline Risk to patient safety Quantity of proposed quality measurescould distract from stage 1 core EMRadoption Lack of specificity with proposedstandards enables variance in systemdevelopment and fosters concernswith clinical quality measure reportingMeaningful Use: Stage 3All Grown Up Introduction of IOM demographiccategories Relies on clarification ofdemographics to be captured instage 2 Standards also include vaguelanguage, which can enable nonstandard or non-compliantimplementation Proposed establishment of clinicaldecision support (CDS) attributesexpands beyond current EMRcapabilities and may be too rigid11
Slide TemplateMeaningful Use: Stage 3All Grown Up (Cont.) New proposed measuresPatient-Reported experience ofcare measures – standard lacks specificityIncorporation of patient-generateddata– requires sufficient lead time for developmentPublic Health Button – requires further clarification fordevelopment and reportingPatient Generated Data submittedto Public Health Agencies – debate on validity of inclusion within EHRSo where to begin? Leverage opportunities to learn andunderstand Meaningful Use Criteria Seek participation in a dedicated, multidisciplinary Task Force Not involved yet? Ask to join current efforts! Support completion of a gap analysis andhelp drive timely rollout of resultingactions Complete Privacy & Security riskassessment12
Slide TemplateAbout Rady Children’s Hospital –San Diego Vision We will be a leader, recognized nationally andinternationally, for excellence in patient care,education, research and advocacy.Mission To restore, sustain and enhance the health anddevelopmental potential of children throughexcellence in care, education, research andadvocacy.Where weProvide Services Through Rady Children'snetwork of physicians,kids can receivespecialized clinical andprimary care services atmore than 30 satellitelocations throughout thecounty.13
Slide TemplateUnique among California’s eightchildren’s hospitals Rady Children's is the largest children’shospital in California 442-bed pediatric care facility providing the largest source ofcomprehensive pediatric medical services in San Diego,Southern Riverside and Imperial counties;Team Of nearly 700 physicians; more than 1,000 nurses on staff; nearly 3,500 employees; 450 active volunteers; and more than 1,200 Auxiliary members.Unique among California’s eightchildren’s hospitals Serves as the only dedicated safety net provider forthe region Providing 90% of all government funded pediatricservices. Is a Level 1 pediatric trauma center. Provides all of the non-neonatal CCS specialty careservices in the region. Has the lowest average length of stay of any Californiachildren’s hospital. Is the only pediatric teaching hospital in the region fordoctors, nurses, pharmacists, and all other pediatricspecific clinical disciplines.14
Slide TemplateUS News & World ReportOur Journey to World ClassIn 2010, the RCHSD ranked specialties are: Orthopedics (#4) Urology (#12) Neonatology (#27) Pulmonology (#30) Diabetes and Endocrinology (#30)Clinical Care Partnerships Scripps Memorial NICU: partnership established in 1999 managing14 beds; Scripps Encinitas NICU: partnership established in 2003 managing 6beds; Sharp Grossmont Pediatric Acute Care: three-year partnershipestablished in 2008 managing 11 beds; Palomar Hospital NICU and Pediatric Acute Care Beds: implementedin August 2010 managing 20 beds; and Sanford Children’s Clinic: in Oceanside opening in April 2011.15
Slide TemplateIn 2009, Rady Children’s Specialists of San Diego, amedical practice foundation, was formed to improve thedelivery of care to our patients while enhancing clinicalresearch, teaching and innovation. Research PartnershipsAs the major provider of pediatric care, RCHSD has become thepediatric clinical laboratory for its extended service area. Currentpartnerships include: UCSDThe Scripps Research InstituteSalk InstituteSanford-Burnham Medical ResearchInstituteSan Diego State UniversitySt. Jude Children’s Research HospitalChild Adolescent Service Research Center(CASRC): a consortium of over 100 investigators and staff frommultiple research organizations in San Diego County strategicallyfocused on improvement of pediatric mental health.16
Slide TemplateFingertip Facts In Fiscal Year 2010, Rady Children’s: Cared for 147,228 children220,000 outpatient visits and more than 15,600inpatient admissions1,159 trauma cases; Ambulance and helicoptertransport was used in 60 percent of all traumacases67,933 emergency care visitsMore than 20,000 surgeriesNearly 11,000 visits at the cardiology clinic andperformed 400 open-and closed-heart surgeriesPeckham Center for Cancer and Blood Disorders,cared for 200 new patients, attended to more than15,400 visits at the Carley Copley Outpatient Clinic,and performed 29 bone marrow transplants.New Acute Care Pavilion Opened on October 10, 2010 LEED-Certified (green) building Home to the incredible newPeckham Center for Cancer andBlood Disorders, the state-of-theart Warren Family SurgicalCenter, and a Neonatal IntensiveCare Unit that cares for ourcommunity’s most fragilenewborns.17
Slide TemplateAudience Question #2What is the status of EMRimplementation at your organization?*1 Partially implemented*2 Implementation in progress*3 Vendor selection underwayEHR Implementation at RCHSD andCHNWhat we did at Children’s Health Networkin San Diego, to select and deploy an EHRAcross the integrated delivery system:Background: Integrated Delivery System Rady Children’s Hospital-San DiegoRady Children’s Specialists San DiegoMedical Practice FoundationChildren’s Primary Care Medical GroupPractice Management GroupRady Children’s Physician ManagementServices18
Slide TemplateEHR Journey Started in2002 Single Repository, Simultaneous Access, Payorand Community MD Portal, MD completion,Legal Electronic Record – 2002 Selection of Epic across the IDS – CHN Revenue Cycle, HIM, ED, Urgent Care Satellites,Ambulatory – 2009 Care Everywhere (HIE), My Chart, EpicCare Link,Inpatient, Pharmacy, Surgery, Oncology - Kickoff – 2010Start with a clear oads/2007/11/df20021001.jpg19
Slide TemplateImprove Care throughInvestment in IT Seamless patient recognitionand access across all entitiesin the IDS Elimination of redundant datacollection points Achievement of “Paper-lite”and automation throughstandardization, integration,common infrastructure andapplications, andconsolidation as appropriate Full visit & encounter historywithin the IDS Alignment with performancemeasurement initiatives Sharing clinical data andpatient information acrossentities Support increasing demand fore-health functionality forCHN/IDS patients and clients Developing advanced clinicalfunctionality, clinical decisionsupportPlan your journey Develop a comprehensiveproject charter Clearly define andcommunicate vision &goals Create & adhere to guidingprinciples Guiding Principles Full Participation Full Focus Business/Clinical Ownership & Accountability Relentless Communication Early, Often Empower Decision Makers Excellence, not perfection Leverage Success of Others–Model System Standardization––Drive efficiency in quality by minimizingvariationValue and respect the business needs ofeach entity On Time/On Budget It’s for the Kids!20
Slide TemplateKeep an eye on what’saheadTimeline: Years 5-821
Slide TemplateIt takes a Village Core implementation team comprisedof: Executive Sponsors, Clinical Champions,Project Management and Team Assure diversity in disciplinerepresentation across theorganization Must be Clinical & Quality LeadershipdrivenAnd a super,Fabulous Team!22
Slide TemplatePlus more Leadership Subject Matter Experts Super Users23
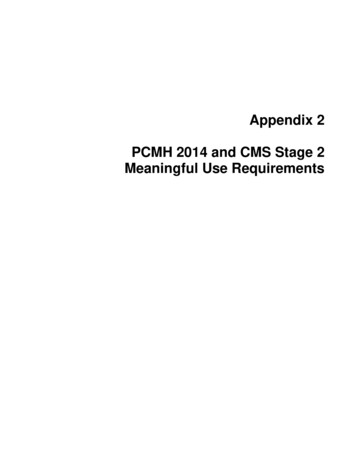
Slide TemplateGovernance is a must!RCHHCBoard ofDirectorsRCPMSBoard ofDirectorsRCSSDBoard ofDirectorsCPCMGBoard ofDirectorsPMGBoard ofDirectors“CHN" Executive CommitteeOrganizationLeadershipand AdviceStrategy/Plan9/05/2008Strategic leadership, policy setting,funding guidelines and budgetapproval for “CHN”projects/initiatives, (including IT),report to Board(s).Ad-hoc. Conflict resolution,enforcement of decisions.CIOAd-hoc. Conflict resolution,enforcement of decisions.EMR/RC Executive CommitteeEMR/RC Steering CommitteeTechnologyAdvisory CouncilClinical InformationAdvisory CouncilDirection/InitiativesRCPIP Stakeholder &Sponsor GroupInformationEMR/RC Workgroups (Ad Hoc)EMR/RC Governance StructureEMR/Rev Cycle strategy, prioritize allEpic related IT initiatives, makerecommendations to ExecutiveCommittee and allocate resources.Provide perspective to identify,evaluate, justify, prioritize,recommend, and monitor EMR/RevCycle project (need to make surethere is adequate representation fromeach Entity- these are workinggroups).Perform detailed tasks such as datagathering, analysis, andimplementation (process & systemdesign, build, validate, test, train,support).Organization Change Management Visibility is everything Ongoing updates, multiple methods MeetingsIntranetBulletin Boards, table tentsBrochuresMonthly Provider and OrganizationalNewslettersEvents! Epic DayProduct DemosIntegrated Workflow WalkthroughDress Rehearsal24
Slide TemplateManage CommunicationCloselySample announcements,posters & take-aways25
Slide TemplateSample announcements,posters & take-awaysSample announcements,posters & take-aways26
Slide TemplateGo-Live &Training PostersStay focused Manage your milestones carefullyand be comfortable with being a‘scope creep’ in order to avoidscope creep27
Slide TemplateBack to the Future Workflow Redesign Assess current state workflow, designfuture state thereafter Plan for optimal environment;understand revisions may occur asthe timeline and project advances Perform gap analysis of change Think out of the box!Sample Future State Workflow:ED to Inpatient A picture is worth a thousand words 28
Slide TemplateTraining & Education Critical success factor for implementationsuccess and long term adoption Mandate training; develop competencychecklist Stand firm on requirement for allroles/disciplinesFlex on duration and timing, depending on userand their level of system use or knowledge.Identify & Engage Super Users in end usertraining processAre we there yet?Understand (and accept) thatgo-live is just the beginning there is no true “end”29
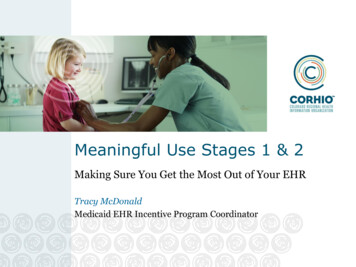
Slide TemplateEHR: Core, Ancillary, and Specialty ApplicationsBefore (2008)Core Clinical Information SystemICU ClinicalPatient RecordOncologyComputerizedPatient RecordAmbulatoryComputerizedPatient RecordNeonatalPoint of CareSurgical Apps- departmentalNeonatalComputerizedPatient RecordSurgical Apps- clinicalEDComputerizedPatient RecordMedicationManagementOnline PatientEducation &EntertainmentClinical TrialsHome HealthServicesNursing ClinicalDocumentationPhysicianDocumentationRT / PT &Speech TherapyOrdering andDocumentationIntegrated Inpatient& OutpatientAdvanced CarePlanning ClinicalProtocols andPathwaysIntelligent ResultsReportingLaboratoryPathologyOrder Communicationand OrderManagementBlood BankDietary andNutritionNeurology /EEG / EMGCardiology /PulmonaryRadiologyOutpatientPharmacy –E-prescribingDischarge Planning /SummaryData WarehouseResults ReviewInpatientPharmacyAdvanced Query andResearch ToolsMedicationAdministrationRecordDocument ImagingPoint of CareMAR with BarCodingKnowledge Engineand links toKnowledge BasesRegistration(ADT)SchedulingEMPIProfessional BillingHIM – Abstracting,Release ofInformationOutpatientPharmacy billingSurveillance ReportingHospital BillingKey:Clinical DataRepositoryAncillary SystemsComputerizedPhysician Order EntryCore System ComponentInterfaced ApplicationPACSPhysician PortalStandalone ApplicationNo ApplicationEHR: Core, Ancillary, and Specialty ApplicationsFall 2011Ancillary SystemsCore Clinical Information SystemICU ClinicalPatient RecordOncologyComputerizedPatient RecordAmbulatoryComputerizedPatient RecordNeonatalPoint of CareSurgical Apps- departmentalNeonatalComputerizedPatient RecordSurgical Apps- clinicalEDComputerizedPatient RecordMedicationManagementOnline PatientEducation &EntertainmentClinical TrialsHome HealthServicesNursing ClinicalDocumentationPhysicianDocumentationRT / PT &Speech TherapyOrdering andDocumentationIntegrated Inpatient& OutpatientAdvanced CarePlanning ClinicalProtocols andPathwaysIntelligent ResultsReportingLaboratoryPathologyOrder Communicationand OrderManagementBlood BankDietary andNutritionNeurology /EEG / EMGCardiology /PulmonaryRadiologyOutpatientPharmacy –E-prescribingDisc
Meaningful Use Stage 1 1. Use of certified EHR technology in a meaningful manner (e.g. e-Prescribing) 2. Electronic exchange of health information to improve quality of care 3. Report clinical quality measures using certified EHR technology CORE Set - 15 mandatory objectives Menu Set - Pick 5 of 10 objectives