Transcription
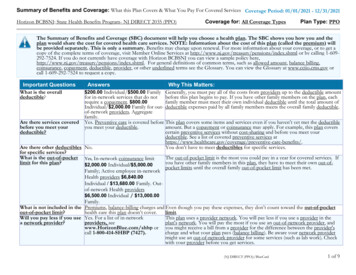
Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered ServicesCoverage Period: Beginning on or after 01/01/2017Geisinger Quality Options: Platinum PlanCoverage for: All Coverage Tiers / Plan Type: PPOThe Summary of Benefits and Coverage (SBC) document will help you choose a health plan. The SBC shows you how you and the plan would share thecost for covered health care services. NOTE: Information about the cost of this plan (called the premium) will be provided separately. This is only asummary. For more information about your coverage, or to get a copy of the complete terms of coverage, call 1-844-390-8332 or visit www.geisinger.org/health-plan. For general definitions of common terms, such as allowed amount, balance billing, coinsurance, copayment, deductible, provider, or otherunderlined terms see the Glossary. You can view the Glossary at www.healthcare.gov/sbc-glossary or call 1-844-390-8332 to request a copy.Important QuestionsAnswersFor preferred providers 0 person / 0 family. ForWhat is the overallnon-preferred providersdeductible? 5,000 person / 10,000family.Yes.Preventive care andAre there services covered primary care services arebefore you meet yourcovered before you meet yourdeductible?deductible.Are there other deductibles No.for specific services?What is the out-ofpocket limit for thisplan?For preferred providers 1,500 person / 3,000family. For non-preferredproviders 10,000 person / 20,000 family.Premiums, balance billingWhat is not included in the charges, and health care thisout-of-pocket limit?plan doesn't cover.Will you pay less if youuse a networkprovider?Do you need a referralto see a specialist?Why This Matters:Generally, you must pay all of the costs from providers up to the deductible amount before this planbegins to pay. If you have other family members on the plan, each family member must meet theirown individual deductible until the total amount of deductible expenses paid by all family membersmeets the overall family deductible.This plan covers some items and services even if you haven't yet met the deductible amount. But acopayment or coinsurance may apply. For example, this plan covers certain preventive serviceswithout cost sharing and before you meet your deductible. See a list of covered preventive services fits.You don't have to meet deductibles for specific services.The out-of-pocket limit is the most you could pay in a year for covered services. If you have otherfamily members in this plan, they have to meet their own out-of-pocket limits until the overall familyout-of-pocket limit has been met.Even though you pay these expenses, they don't count toward the out-of-pocket limit.Yes. Seewww.geisinger.org/health-planor call 1-844-390-8332 for a listof network providers.This plan uses a provider network. You will pay less if you use a provider in the plan's network. Youwill pay the most if you use an out-of-network provider, and you might receive a bill from a providerfor the difference between the provider's charge and what your plan pays (balance billing). Beaware, your network provider might use an out-of-network provider for some services (such as labwork). Check with your provider before you get services.No.You can see the specialist you choose without a referral.Geisinger Quality Options, Inc. - Platinum Plan1 of 6
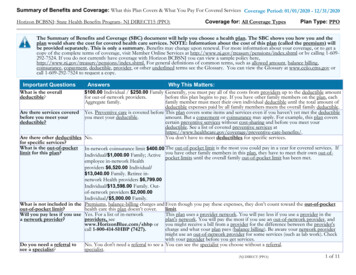
All copayment and coinsurance costs shown in this chart are after your deductible has been met, if a deductible applies.CommonMedical EventIf you visit a healthcare provider's officeor clinicIf you have a testIf you need drugs totreat your illness orconditionMore information aboutprescription drugcoverage is available atwww.geisinger.org/health-planIf you have outpatientsurgeryWhat You Will PayServices You May NeedPreferred Provider(You will pay the least)Limitations, Exceptions, & OtherImportant InformationNon-Preferred Provider(You will pay the most)Primary care visit to treat aninjury or illnessSpecialist visit 20 copayment / visit30% coinsuranceNone 35 copayment / visit30% zationNo charge30% coinsuranceDiagnostic test (x-ray, bloodwork)Covered: cost share basedon place of service.30% coinsuranceImaging (CT/PET scans,MRIs)Generic drugs (Tier 1)No charge30% coinsurance 4 copayment retail / 10copayment mail order50% coinsurancePreferred brand drugs(Tier 2)Non-preferred brand drugs(Tier 3)Specialty drugs (Tier 4) 20 copayment retail / 50copayment mail order 40 copayment retail / 100copayment mail order50% coinsurance50% coinsuranceYou may have to pay for services that arenot preventive. Ask your provider if theservices needed are preventive. Then checkwhat your plan will pay for.Precertification/prior authorization requiredCovers up to a 30-day supply retail, 90 daysupply mail order. Out-of-network coverageonly applies when the member is unable touse a network pharmacy. Member must payin full and submit for reimbursement.Cost varies by drug based on 50% coinsuranceaboveFacility fee (e.g., ambulatorysurgery center) 100 copayment / visit30% coinsurancePrecertification/prior authorization maybe required.Physician/surgeon feesNo charge30% coinsurancePrecertification/prior authorization may berequired.Geisinger Quality Options, Inc. - Platinum Plan2 of 6
CommonMedical EventWhat You Will PayServices You May NeedNon-Preferred Provider(You will pay the most) 100 copaymentEmergency medicaltransportationNo chargeNo chargeEmergency medical transportation: NoneUrgent care 50 copayment30% coinsuranceUrgent care: None.Facility fee (e.g., hospitalroom) 250 copayment / admission 30% coinsurancePhysician/surgeon feesNo charge30% coinsurancePrecertification/prior authorization required. 20 copayment / visit30% coinsuranceInpatient services 250 copayment /admission30% coinsuranceOutpatient Services: None.Inpatient Services: Deductible (if any)applies.Office visitsCovered under globalmaternity fee.30% coinsuranceChildbirth/deliveryprofessional servicesNo charge30% coinsuranceChildbirth/delivery facilityservices 250 copaymentEmergency room careIf you needimmediate medicalattentionIf you have ahospital stayIf you need mentalhealth, behavioralhealth, or substanceabuse servicesIf you are pregnantLimitations, Exceptions, & OtherImportant InformationPreferred Provider(You will pay the least) 100 copayment,Outpatient servicesEmergency services: Copayment waived ifadmitted to hospital.Precertification/prior authorization required.Pregnancy office visits: None. Cost sharingdoes not apply for preventive services.Depending on the type of services, acopayment, coinsurance or deductible mayapply.Inpatient professional and facility services:Deductible (if any) applies andPrecertification/prior authorization.30% coinsuranceGeisinger Quality Options, Inc. - Platinum Plan3 of 6
CommonMedical EventIf you need helprecovering or haveother special healthneedsIf you child needsdental or eye careWhat You Will PayServices You May NeedHome health careRehabilitation servicesPreferred Provider(You will pay the least)No charge 35 copayment / visitNon-Preferred Provider(You will pay the most)30% coinsurance30% coinsuranceHabilitation services 35 copayment / visit30% coinsuranceSkilled nursing care 250 copayment / admission30% coinsuranceDurable medical equipmentHospice servicesChildren's eye examChildren's glassesChildren's dental check-upNo chargeNo chargeNot coveredNot coveredNot covered30% coinsurance30% coinsuranceNot coveredNot coveredNot coveredLimitations, Exceptions, & OtherImportant InformationLimited to 120 visits/benefit periodLimited to 60 days of servicecombined/benefit period and combine withHabilitation.Check with Plan for details and limitations.Limited to 120 days / benefit period.Check with Plan for coverage and limitations.NoneNoneNoneNoneExcluded Services & Other Covered Services:Services Your Plan Generally Does NOT Cover (Check your policy or plan document for more information and a list of any other excluded services.) Cosmetic Surgery Long-Term Care Private-Duty Nursing Dental Care Non-Emergency Care when Traveling Routine Foot CareOutside the U.S. Routine eye care (Adult) Weight Loss ProgramsOther Covered Services (Limitations may apply to these services. This isn't a complete list. Please see your plan document.) Acupuncture Chiropractic Care Infertility Treatment Bariatric Surgery Hearing AidsYour Rights to Continue Coverage: There are agencies that can help if you want to continue your coverage after it ends. The contact information for those agenciesis: The U.S. Department of Labor, Employee Benefits Security Administration at 1-866-444-3272 or www.dol.gov/ebsa/healthreform, or the U.S Department of Healthand Human Services at 1-877-267-2323 x61565 or www.cciio.cms.gov. Other coverage options may be available to you too, including buying individual insurancecoverage through the Health Insurance Marketplace. For more information about the Marketplace, visit www.HealthCare.gov or call 1-800-318-2596.Geisinger Quality Options, Inc. - Platinum Plan4 of 6
Your Grievance and Appeals Rights: There are agencies that can help you if you have a complaint against your plan for a denial of a claim. This complaint is called agrievance or appeal. For more information about your rights, look at the explanation of benefits you will receive for that medical claim. Your plan documents alsoprovide complete information to submit a claim, appeal, or a grievance for any reason to your plan. For more information about your rights, this notice, or assistance,contact 1-877-881-6388.Does this plan provide Minimum Essential Coverage? YesIf you don't have Minimum Essential Coverage for a month, you'll have to make a payment when you file your tax return unless you qualify for an exemption from therequirement that you have health coverage for that month.Does this plan meet Minimum Value Standards? Yes.If your plan doesn't meet the Minimum Value Standard, you may be eligible for a premium tax credit to help you pay for a plan through the Marketplace.Language Access Services:To access our Language helpline, please call 1-844-390-8332.Spanish (Español): Para obtener asistencia en Español, llame al 1-844-390-8332.Tagalog (Tagalog): Kung kailangan ninyo ang tulong sa Tagalog tumawag sa 1-844-390-8332.Chinese (中文): � 1-844-390-8332.Navajo (Dine): Dinek'ehgo shika at'ohwol ninisingo, kwiijigo holne' �–––––––To see examples of how this plan might cover costs for a sample medical situation, see the next –––––Geisinger Quality Options, Inc. - Platinum Plan5 of 6
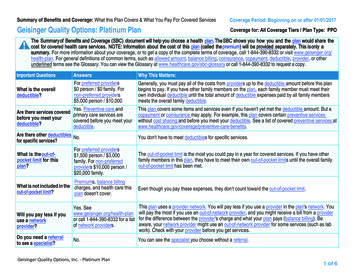
About these Coverage Examples:This is not a cost estimator. Treatments shown are just examples of how this plan might cover medical care. Your actual costs will be differentdepending on the actual care you receive, the prices your providers charge, and many other factors. Focus on the cost sharing amounts(deductibles, copayments and coinsurance) and excluded services under the plan. Use this information to compare the portion of costs you mightpay under different health plans. Please note these coverage examples are based on self-only coverage.Peg is Having a BabyManaging Joe's type 2 Diabetes(9 months of in-network pre-natal care and ahospital delivery)(a year of routine in-network care of a wellcontrolled condition) 0 350%0%The plan's overall deductibleSpecialist copaymentHospital (facility) coinsuranceOther coinsuranceThis EXAMPLE event includes services like:Specialist office visits (prenatal care)Childbirth//Delivery Professional ServicesChildbirth/Delivery Facility ServicesDiagnostic tests (ultrasounds and blood work)Specialist visit (anesthesia)Total Example CostThe plan's overall deductibleSpecialist copaymentHospital (facility) coinsuranceOther coinsurance 0 350%0%This EXAMPLE event includes services like:Primary care physician office visits (includingdisease education)Diagnostic tests (blood work)Prescription drugsDurable medical equipment (glucose meter) 12,800In this example, Peg would pay:Total Example CostThe plan's overall deductibleSpecialist copaymentHospital (facility) coinsuranceOther coinsurance 7,400Total Example Cost 0What isn't coveredLimits or exclusionsThe total Peg would pay is 516 0DeductiblesCopaymentsCoinsurance 10 526What isn't coveredLimits or exclusionsThe total Joe would pay is 1,900In this example, Mia would pay:Cost SharingDeductiblesCopaymentsCoinsurance 0 350%0%This EXAMPLE event includes services like:Emergency room care (including medicalsupplies)Diagnostic test (x-ray)Durable medical equipment (crutches)Rehabilitation services (physical therapy)In this example, Joe would pay:Cost SharingMia's Simple Fracture(in-network emergency room visit and follow upcare)Cost Sharing 0 635 0DeductiblesCopaymentsCoinsurance 0 205 0 60 695What isn't coveredLimits or exclusionsThe total Mia would pay is 0 205The plan would be responsible for the other costs of these EXAMPLE covered services.Geisinger Quality Options, Inc. - Platinum Plan6 of 6
Discrimination is against the lawGeisinger Quality Options, Inc. complies with applicablefederal civil rights laws and does not discriminate on the basisof race, color, national origin, age, disability, sex, genderidentity, or sexual orientation. Geisinger Quality Options, Inc.R Sc d ShQ[eRS S [S b dbSNd dWS] RXůSbS d[i PSQNecS of race, color, national origin, age, disability, sex, genderidentity, or sexual orientation.Geisinger Quality Options, Inc.: Provides free aids and services to people with disabilitiesd Q ]]e XQNdS SůSQdXfS[i gXdW ec ceQW Nc DeN[XűSR cXV [N VeNVS X dSb bSdSbc Written information in other formats (large print,audio, accessible electronic formats, other formats) Provides free language services to people whose primarylanguage is not English, such as: DeN[XűSR X dSb bSdSbc Information written in other languagesIf you need these services, call Geisinger Quality Options, Inc.at 800-447-4000 or TTY: 711.If you believe that Geisinger Quality Options, Inc. has failed toprovide these services or discriminated in another way on thebasis of race, color, national origin, age, disability, sex, genderXRS dXdi b cSheN[ bXS dNdX i e QN ű[S N VbXSfN QS gXdW Civil Rights Grievance CoordinatorGeisinger Health Plan Appeals Department100 North Academy Avenue, Danville, PA 17822-3220Phone: 866-577-7733, TTY: 711Fax: 570-271-7225GHPCivilRights@thehealthplan.comL e QN ű[S N VbXSfN QS X Sbc b Pi ]NX[ TNh b S]NX[Ͷ T i e SSR WS[ ű[X V N VbXSfN QS dWS 5XfX[ EXVWdc 9bXSfN QS Coordinator is available to help you.L e QN N[c ű[S N QXfX[ bXVWdc Q ] [NX d gXdW dWS HͶFͶ 6S Nbd]S d T ;SN[dW N R ;e]N FSbfXQSc BŶQS T b 5XfX[ EXVWdc S[SQdb XQN[[i dWb eVW dWS BŶQS T b 5XfX[ EXVWdc Complaint Portal, available at https://ocrportal.hhs.gov/ocr/portal/lobby.jsf, or by mail or phone at:HͶFͶ 6S Nbd]S d T ;SN[dW N R ;e]N FSbfXQSc RS S RS QS 3fS eS FJͶ E ] 8HHH Building, Washington, DC 20201CW S Ν Ν Ν Ν ͥG66ͦComplaint forms are available atWdd ώώgggͶWWcͶV fώ Qbώ ŶQSώű[SώX RShͶWd][ͶATTENTION: If you speak a language other than English, language assistance services, free of charge, are available to you. Call 800-447-4000 or TTY: 711.ATENCIÓN: si habla español, tiene a su disposición servicios gratuitos de asistencia lingüística. Llame al 800-447-4000 (TTY: 711).㲐シ烉 㝄ぐἧ䓐 橼ᷕ㔯炻ぐ ẍ 屣䌚 婆妨 㚵 ˤ婳农暣ġ800-447-4000㸦TTY㸸711㸧ˤCHÚ Ý: Nũu bįn nói Tiũng Viŭt, có các dƌch vǖ hƲ trƹ ngôn ngǜ miŬn phí dành cho bįn. Gƭi sƯ 800-447-4000 (TTY: 711).ġ ́ ̀ ́ ̴̺̱ ̪̈́ ̷̷̫̪̹̱̻̭ ̶̧ ̷̵̹̼̺̺̳ ͈̰̳̭̈́ ̷̻ ̵̧̪ ̷̸̶̬̺̻̼̈́ ̸̴̶̧̩̭̺̻̭̈́ ̴̼̺̼̫̱ ̸̷̧̭̹̭̪̬Ͷ ̷̶̪̱̻̭ 800-447-4000 ̴̸̧̻̭̭̻̲ͥ 711).ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachliche Hilfsdienstleistungen zur Verfügung. Rufnummer: 800-447-4000 (TTY: 711).㨰㢌aGG䚐ạ㛨 G 㟝䚌㐐 Gᷱ㟤SG㛬㛨G㫴㠄G Gⱨ ⦐G㢨㟝䚌㐘G G㢼 UG800-447-4000 (TTY: 711) ⶼ㡰⦐G㤸䞈䚨G㨰㐡㐐㝘UATTENZIONE: In caso la lingua parlata sia l'italiano, sono disponibili servizi di assistenza linguistica gratuiti. Chiamare il numero 800-447-4000 (TTY: 711).711 ϢϜΒϟ ϭ Ϣμϟ ϒΗΎϫ Ϣϗέ 800-447-4000 ϢϗήΑ ϞμΗ ϥΎΠϤϟΎΑ Ϛϟ ήϓ ϮΘΗ ΔϳϮϐϠϟ ΓΪϋΎδϤϟ ΕΎϣΪΧ ϥΈϓ ˬΔϐϠϟ ήϛΫ ΙΪΤΘΗ ΖϨϛ Ϋ· ΔυϮΤϠϣATTENTION : Si vous parlez français, des services d'aide linguistique vous sont proposés gratuitement. Appelez le 800-447-4000 (ATS : 711).ACHTUNG: Wenn Sie Deutsch sprechen, stehen Ihnen kostenlos sprachliche Hilfsdienstleistungen zur Verfügung. Rufnummer: 800-447-4000 (TTY: 711).k Wh: Ks S\p ȤKk hSj Zs Sh es, Ss iW:Ƀƣk D [hch deh] dpahB S\h h \hN ;X ƞV Jp . YsW D s 800-447-4000 (TTY: 711).ɅIHJ393 SDzS[X ]ƣgXck [cZe ] DzSck cZ bkicdNŕ k PSk ƗNd SY ] Qi YŤkiZ gSYͶ MNRkg Ɲ R e]Sb 800-447-4000 (TTY: 711).3G3AFLBA FX g N[S bSiƧ[ 3iXciS VS cŢfXc ŢR e [ang ki disponib gratis pou ou. Rele 800-447-4000 (TTY: 711).ƅŞŻȽŅŚɉ ȒŞȋơǯřēƴŚ éřǯžŻ ŴƤȓîŷ Ƅ, ȒơƑĐșřȇŻȓŧŚéŴƤ ȒīŻŶǯřóǯŅĕśƉȉ óǽƷĆŹřơșƇŞȥŞșȒ Ƅ ǶƴŚ éɇ ĆȄ Ƅ ŏȄ ƄơȽŬŐ 800-447-4000 (TTY: 711)ɇATENÇÃO: Se fala português, encontram-se disponíveis serviços linguísticos, grátis. Ligue para 800-447-4000 (TTY: 711).;C@ N[P A RXcQbX]X NdX RSfͶ Ͷ Ͷ L ϑ ϑ 8X[S N R HcS ώ ώ
Geisinger Quality Options: Platinum Plan . Coverage for: All Coverage Tiers / Plan Type: PPO. Summary of Benefits and Coverage: What this Plan Covers & What You Pay For Covered Services . Coverage Period: Beginning on or after 01/01/2017 The Summary of Benefits and Coverage (SBC) document will help you choose a health plan.