Transcription
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447COSMETICClinical Implications of Gluteal Fat GraftMigration: A Dynamic Anatomical StudyAQ1Daniel A. Del Vecchio, M.D.Nathaniel L. Villanueva,M.D.Raja Mohan, M.D.Bret Johnson, M.D.Dinah Wan, M.D.Aniketh Venkataram, M.D.Rod J. Rohrich, M.D.Boston, Mass.; Dallas, Texas; andBangalore, IndiaDBackground: The intraoperative mortality and overall complication rate forgluteal augmentation with fat transplantation is unacceptably high. The current controversy among experts regarding safety is whether fat should beplaced within the gluteus muscle or limited to only the subcutaneous space.The purpose of the present study was to test the hypothesis that under certainpressures, fat injected within the gluteal muscle can actually migrate out of themuscle and into a deeper plane containing critical neurovascular structures,by means of the process of deep intramuscular migration.Methods: A total of eight human cadaver dissections were performed. Fourhemibuttocks were selected for intramuscular fat injection. The patterns ofsubfascial fat migration were evaluated in three of these hemibuttocks by directvisual inspection and in one hemibuttock by endoscopic evaluation. Four otherhemibuttocks were selected for subcutaneous or suprafascial fat injection.Results: Proxy fat was found to migrate through the muscle and into the deepsubmuscular space with each intramuscular injection. With subcutaneous injection, no proxy fat was found during dissection in the intramuscular septaeor submuscular space.Conclusions: The intramuscular insertion of fat, which up to this point hasbeen considered reasonable to perform in the superficial muscle and evenrecommended in the literature, is now deemed to be an inexact and risky surgical technique. This technique, because of the migratory nature of injectedfat, should be avoided from further use in fat transplantation to the glutealregion. (Plast. Reconstr. Surg. 142: 00, 2018.)espite having the highest annual growthrate of any cosmetic surgical procedure, theintraoperative mortality rate for gluteal augmentation with fat transplantation (i.e., Brazilianbutt lift) is unacceptably high.1–7 A recent surveyperformed by the American Society of AestheticPlastic Surgeons estimates the intraoperative deathrate from this operation to be approximately onein 2351.1 In addition to these fatal complications,serious nonfatal complications, namely microfatembolism and sciatic nerve injury, are also surprisingly high.8,9 The root cause of these complicationsfocuses on the depth of fat insertion.1,4–6 The currentcontroversy among experts is whether fat shouldbe placed within the gluteus muscle or whether fatshould be limited to the subcutaneous space only,which lies superficial to the muscle fascia.7,10–31From Back Bay Plastic Surgery; the Department of PlasticSurgery, University of Texas Southwestern Medical Center;the Dallas Plastic Surgery Institute; and the Venkat Centerfor Skin and Plastic Surgery.Received for publication February 13, 2018; accepted July11, 2018.Copyright 2018 by the American Society of Plastic SurgeonsDOI: 10.1097/PRS.0000000000005020Surgeons who have experienced complicationsof sciatic nerve injury in their own patients as a resultDisclosure: Dr. Rohrich receives instrument royalties from Eriem Surgical, Inc., and book royaltiesfrom Thieme Medical Publishing. He is a clinicaland research expert for Allergan, Inc., and MTF Biologics, and the owner of Medical Seminars of Texas,LLC. No funding was received for this article. Dr. DelVecchio is a founder of Surgistem Technologies, LLC,a device company involved in fat transplantation,receives royalties from Microaire, and is a foundingmember of Peninsula Partners, LLC, a consultingfirm in the plastic surgery sector. The remaining authors have no financial interest to declare in relationto the content of this article.AQ8Supplemental digital content is available forthis article. Direct URL citations appear in thetext; simply type the URL address into any Webbrowser to access this content. Clickable linksto the material are provided in the HTML textof this article on the Journal’s website (www.PRSJournal.com).www.PRSJournal.com1Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
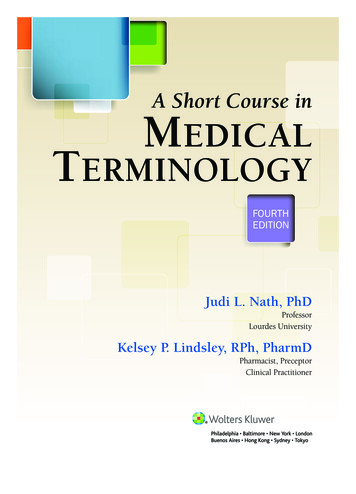
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Plastic and Reconstructive Surgery November 2018of gluteal fat transfer insist that fat was injected onlywithin the muscle and not below it.8 Similarly, surgeons who have experienced patient death frompulmonary fat embolism insist that their gluteal fatinjections remained only in the subcutaneous tissue and superficial muscle. Nevertheless, such devastating complications continue to be seen with theBrazilian lift, with a reported rate of 1.7 percent forsciatic nerve injuries alone.4 The fact that these morbidities and mortalities continue to be reported atunacceptably high rates despite seemingly superficial fat injections suggests that another mechanismof injury other than direct cannula hits of major gluteal vessels and nerves may be playing a role.In this study, we introduce the phenomenon ofdeep intramuscular migration, wherein large volumes of fat injected into the gluteus muscle havethe potential to migrate along the path of least resistance within the muscle and, ultimately, even out ofthe muscle in the setting of exceedingly high pressures. This process describes subjacent fat migration to danger zones deep to the gluteal muscleleading to potential pressure-induced injuries ofthe sciatic nerve or traction-induced tears of majorvenous structures in the region. This in turn mayexplain conditions of sciatic nerve impairment andpulmonary fat embolism after the Brazilian lift procedure despite surgeon insistence that injection wasperformed in a more superficial plane.The purpose of this study was to test thehypothesis that under certain pressures, fatinjected in the gluteal muscle can actually migrateout of the muscle into a deeper plane containingcritical neurovascular structures, by means of theprocess of deep intramuscular migration.Four other hemibuttocks were selected for subcutaneous or suprafascial fat injection.Intramuscular Fat InjectionDirect Inspection of Subfascial Fat MigrationOn three hemibuttocks, the posterior superioriliac crest, the sacral hiatus, and the greater trochanter were palpated. Drawing the letter A fromthe structures, the approximate location of theMATERIALS AND METHODSA total of eight dissections were performed infour fresh human cadavers obtained with permission from the Willed Body Program at the University of Texas Southwestern Medical Center. Thecadavers were selected randomly to be in one ofthree groups. Four hemibuttocks were selectedfor intramuscular fat injection. The patterns ofsubfascial fat migration were evaluated in three ofthese hemibuttocks by direct visual inspection andin one hemibuttock by endoscopic evaluation.By reading this article, you are entitled to claimone (1) hour of Category 2 Patient Safety Credit.ASPS members can claim this credit by loggingin to PlasticSurgery.org Dashboard, clicking“Submit CME,” and completing the form.Fig. 1. (Above) Landmarks, (center) dissection zone, and (below)posterior gluteus fascia.2Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
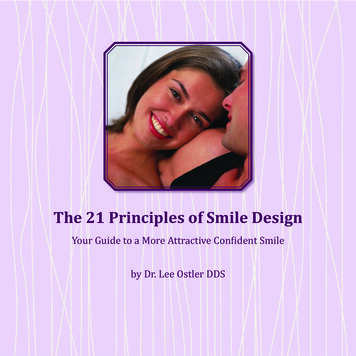
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Volume 142, Number 5 Gluteal Fat Graft MigrationF1superior gluteal and inferior gluteal vascular leasheswere marked (Fig. 1, above). A 10-cm-diameter circleencompassing these vascular structures was thenmarked on the skin (Fig. 1, center). Dissection of theskin and subcutaneous tissue was performed, revealing the superficial gluteal fascia (Fig. 1, below).Using a 4-mm Luer-lock multihole injectioncannula (Lipo, Farmingdale, N.Y.), applesauce(Motts, Inc., a division of Dr. Pepper Snapple,Plano, Texas) was stained using blue food coloring as a proxy for transplanted fat. This “proxyfat” was injected into the superficial intramuscularspace of the gluteus maximus muscle using 60-mlsyringes. Care was taken to avoid cannula passagedeeper than 2 cm, keeping the cannula tip visiblyin the superficial muscle throughout the course ofthe injection. With each progressive 60-cc syringeinjection, intramuscular recipient-site pressureswere measured using a Stryker compartment pressure monitor (Stryker, Inc., Kalamazoo, Mich.).The gluteus muscle was then reflected laterally off of its sacral origin to expose the subjacentmusculature and venous plexus of the superiorgluteal and inferior gluteal vascular systems, andto inspect for the location of fat migration. Thedeep surface of the gluteus muscle was examinedfor the presence of demonstrable fascia.Endoscopic Inspection of Intramuscular FatMigrationA 3-cm horizontal incision was made in theupper outer quadrant on one hemibuttock.Using digital dissection, the most cephalad portion of the gluteus medius was encountered.More distally, the cephalad border of the gluteus maximus was identified and the submuscular space was navigated using a 10-mm 0-degreeendoscope (Karl Storz, Charlton, Mass.). Anendoscopic breast system including a fiberopticcamera and an endoscopic breast retractor wasused to expose the superior gluteal and inferior gluteal vascular bundles. The proxy fat wasagain injected into the superficial intramuscularspace of the gluteus maximus muscle using 60-mlsyringes. Direct real-time inspection of the submuscular space was monitored for the appearance of migrated proxy fat.Subcutaneous Fat InjectionDirect Inspection of Subcutaneous(Suprafascial) Fat MigrationOn four hemibuttocks, a 10-cm-diameter circlein the same location as shown in Figure 1, abovewas drawn. Using a percutaneous needlestick, thesame 4-mm Luer-lock multihole injection cannulaused previously was placed beneath the skin, andproxy fat loaded into 60-ml syringes was injectedinto a subcutaneous space, directly between theestimated location markings of the superior andinferior gluteal vessels, and superficial to the gluteus maximus muscle fascia. With each progressiveinjection of 60-cc increments, intramuscular recipient-site pressures were measured using a Strykercompartment pressure monitor (Fig. 2, above) andthe location of the cutaneous contour change wasrecorded as the distance from the visible “migration front” to the injection epicenter (Fig. 2, below).At the completion of the subcutaneous injection,gross inspection of subcutaneous fat migration wasperformed by dissecting the subcutaneous layerfrom the superficial gluteal fascia. Finally, the gluteus maximus muscle was reflected laterally fromits sacral origin to inspect for the presence of fatmigration within the gluteus maximus muscle orinto the deep submuscular space in proximity tothe superior and inferior gluteal vascular systems.Anatomical DissectionUsing a traditional “pages of a book” dissection, skin and subcutaneous tissue of one hemibuttock was reflected inferiorly, followed by gluteusmaximus muscle, exposing the submuscular areolarspace, the gluteal vessels, the sciatic nerve, and thesciatic notch. (See Video, Supplemental Digital Content 1, which demonstrates anatomical dissection.The detailed anatomy deep to the gluteus maximusmuscle is shown. There is a robust posterior fasciaoverlying the gluteus maximus muscle but there isno clinically apparent anterior fascia. The locationof the gluteal vessels is highlighted in this dissection,available in the “Related Videos” section of the fulltext article on PRSJournal.com or, for Ovid users,available at http://links.lww.com/PRS/D46.)F2V1RESULTSDirect Inspection of Subfascial Fat MigrationSubfascial insertion of proxy fat volumesranged from 540 ml to 720 cc. With each 60 mlof proxy fat inserted, visual expansion of the buttock volume was observed. As larger volumes wereinserted, expansion of buttock projection wasobserved from the perisacral area all the way tothe greater trochanter, consistent with the shapeof the gluteus maximus muscle (Fig. 3). With eachprogressive 60 ml of proxy fat inserted, intramuscular compartment pressures increased progressively, as shown in Table 1. Of note, during oneof the injections, there was a sudden drop inAQ2F3T13Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Plastic and Reconstructive Surgery November 2018Fig. 2. (Above) Initiation of subcutaneous injection. O representsthe epicenter of proxy fat insertion. (Below) After 500 cc of proxyfat, a contour change representing the maximum migration front(MF) is identified and its distance from the epicenter O is measured.Video 1. Supplemental Digital Content 1 demonstrates anatomicaldissection. The detailed anatomy deep to the gluteus maximus muscle is shown. There is a robust posterior fascia overlying the gluteusmaximus muscle but there is no clinically apparent anterior fascia. Thelocation of the gluteal vessels is highlighted in this dissection, available in the “Related Videos” section of the full-text article on PRSJournal.com or, for Ovid users, available at http://links.lww.com/PRS/D46.4Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
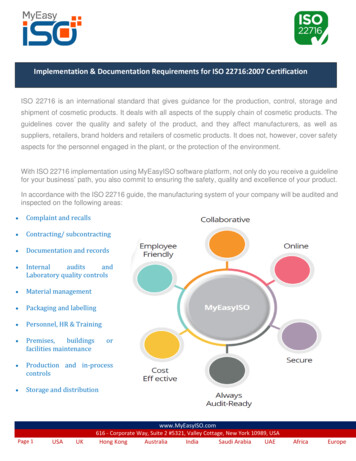
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Volume 142, Number 5 Gluteal Fat Graft MigrationFig. 3. Proxy fat placed in the central portion of the gluteus muscle(green arrow) results in submuscular proxy fat emanating near theorigin of the gluteus maximus muscle.Fig. 4. Deep intramuscular migration. Proxy fat (upper arrow)escaping between muscle fibers of the gluteus maximus muscle toenter the deep muscular space in the area of the superior glutealvessels (lower arrow).AQ3injection resistance followed by a decrease in pressure. On further volume injection, the pressurebegan to rise once more.Table 1. Subfascial Migration*Volume Injected (cc)60120180240300360420480540600660720780Pressure (mmHg)485555657079879295117121128112*Changes in intramuscular pressure with increasing injectionvolume.When the gluteus maximus muscle was releasedfrom its sacral origin, a large rush of proxy fat wasnoted to emanate from the submuscular space, inan area far medial and deep to the original cannula insertion (Fig. 4). [See Video, SupplementalDigital Content 2, which demonstrates the migration of intramuscular fat in gluteal augmentation.The landmarks to identify the location of the gluteal vessels are first shown. Underneath the subcutaneous layer, the posterior fascia over the gluteusmaximus muscle is observed. Applesauce (pseudofat) is injected into the superficial fascia of thegluteus maximus muscle. The pressure within thesubmuscular space increased with each injection.The pseudofat migrated underneath the muscleand spread throughout the submuscular space.Because of the lack of anterior fascia on the gluteus maximus muscle, the pseudofat migrateddeep to the muscle and surrounded the glutealF4,V25Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Plastic and Reconstructive Surgery November 2018Video 2. Supplemental Digital Content 2 demonstrates the migration of intramuscular fat in gluteal augmentation. The landmarks toidentify the location of the gluteal vessels are first shown. Underneath the subcutaneous layer, the posterior fascia over the gluteusmaximus muscle is observed. Applesauce (pseudofat) is injectedinto the superficial fascia of the gluteus maximus muscle. Thepressure within the submuscular space increased with each injection. The pseudofat migrated underneath the muscle and spreadthroughout the submuscular space. Because of the lack of anteriorfascia on the gluteus maximus muscle, the pseudofat migrateddeep to the muscle and surrounded the gluteal vessels, availablein the “Related Videos” section of the full-text article on PRSJournal.com or, for Ovid users, available at http://links.lww.com/PRS/D47.F5F6F7vessels, available in the “Related Videos” sectionof the full-text article on PRSJournal.com or, forOvid users, available at http://links.lww.com/PRS/D47.] When the gluteus maximus muscle wasreflected laterally to expose the gluteal vessels,proxy fat was noted to occupy the space beneaththe gluteus maximus muscle, tracking all the wayto the greater trochanteric insertion. In addition, fat was noted to occupy intermuscular septal spaces within the muscle itself (Fig. 5). Finally,during inspection of the undersurface of all gluteus maximus muscles in the study, there was noevidence of a deep fascial layer on the undersurface of the gluteus maximus muscle (Fig. 6).Endoscopic Inspection of Intramuscular FatMigrationDuring endoscopic inspection of the undersurface of the gluteus muscle, it was possible to safelyenter the deep submuscular space by means ofa cephalad approach and to identify the superiorand inferior gluteal vessels that closely coincidedwith the topographic cutaneous landmarks (Fig. 7).During simultaneous endoscopic inspection andreal-time intramuscular injection of proxy fat, fatwas noted to well up in the submuscular space,consistent with an intramuscular septal “blowout”and subsequent entrance of proxy fat into the submuscular space (Fig. 8). (See Video, SupplementalDigital Content 3, which demonstrates the migration of intramuscular fat in gluteal augmentation.After injection of pseudofat into the superficial fascia of the gluteus maximus muscle, we show that thepseudofat migrates deep and is deposited withinthe submuscular space. The pseudofat enters deepto the muscle through multiple areas within themuscle. Using an endoscope, we demonstrate thatthese injections of pseudofat into the superficial fascia of the muscle migrated into the space deep themuscle. The posterior fascia of the gluteus maximusmuscle acts as a backstop and prevents migration ofpseudofat into the subcutaneous space, available inthe “Related Videos” section of the full-text articleon PRSJournal.com or, for Ovid users, available athttp://links.lww.com/PRS/D50.)F8Direct Inspection of Subcutaneous (Suprafascial)Fat MigrationDuring subcutaneous insertion of 500 to 1500cc of proxy fat in 60-cc increments, intramuscular6Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Volume 142, Number 5 Gluteal Fat Graft MigrationFig. 5. Intramuscular fat migration. Fat was noted to occupy intermuscular septal spaces within the muscle itself.Fig. 6. Lack of anterior gluteal fascia. Note that on the deep or anatomically “anterior” side of the gluteus maximus muscle there is nofascial layer.F9compartment pressures did not change (remainedat 0). As the volume of proxy fat increased inthe subcutaneous space, topographic contourchange, as represented by a visible migrationfront, increased in dimension and subcutaneous pressures increased to as high as 55 mmHg.Postinjection dissection of the subcutaneousspace revealed proxy fat, which freely traversedthroughout the subcutaneous tissue. Neither thegluteus maximus intramuscular septae nor thedeep submuscular space subjacent to the gluteusmaximus muscle revealed any evidence of disruption or the presence of proxy fat (Fig. 9).DISCUSSIONIntramuscular fat grafting in the gluteal regionhas been a mainstay of Brazilian lift surgery forthe past decade or more.12–16,19,21–34 This is becauseof the theoretically increased volume capacity ofthe intramuscular space compared with the subcutaneous space. Without active disruption ofrecipient-site connective tissue, internal expansion of the subcutaneous space is impossible, asis the case when using traditional syringe-basedinjection techniques that simply “wedge” fat in asmicrodroplets.35 Thus, the intramuscular spacehas been traditionally favored as a recipient sitefor gluteal fat transfer. However, since the inception of expansion vibration lipofilling, which creates intraoperative expansion of the subcutaneousspace by means of mechanical disruption withinternal caged reciprocating cannulas, there hasbeen less reliance on the intramuscular space asthe only recipient site capable of accepting relatively large fat volumes.36 Expansion vibration lipofilling can potentially increase the capacity of thesubcutaneous recipient site and allow for effectivegluteal lipofilling without the need to resort to themuscle.37There has been much discussion about thesafety of intramuscular fat grafting to the glutealregion, many with the stipulation that surgeons7Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Plastic and Reconstructive Surgery November 2018Fig. 7. Accuracy of cutaneous markings and navigation of the submuscular space. (Left) The submuscular planecan be entered from above (this is the left hemibuttock). The inferior gluteal vascular leash is visible in the looseareolar submuscular plane, and its location coincides with the topographic markings. (Right) Endoscopic real-timeinspection of fat migration. Endoscopic view of the undersurface of the gluteus maximus muscle before subfascialfat injection. Note the absence of fascia.follow “safety zones” or stay in the “superficialmuscle.”3 Although the anatomical basis of the“safety triangle” theoretically makes sense, thereis insufficient clinical evidence to prove that itis failsafe in human patients. The opinion thatintramuscular fat transplantation is “safe” rests onan important assumption—that fat placed in theintramuscular space remains in the intramuscularspace. The findings of the present study suggestthat fat grafted within the muscle can migratethrough the deep side of the gluteus muscle intothe underlying submuscular space, implying thatthere is no zone within the gluteus maximus muscle that can be considered safe.Whether one inserts fat in the deep or superficial muscle, given enough volume, it will notremain in the muscle and will spill deep to thesubmuscular space. There have been reportsof the direction of cannula insertion as connoting some element of safety.10,38 Insertion fromthe inferior gluteal crease incision (from below)has been suggested to be more dangerous thaninjecting from a natal cleft approach (from above,medial). This has been traditionally explained bya “direct hit” paradigm, namely that angulatingthe cannula in certain directions poses increasedrisk for penetrating the submuscular space andhitting a deep vein coming from below. Thedeep intramuscular migration theory provides analternative explanation, whereby injecting fromthe natal cleft directs the cannula parallel to themuscle fibers, depositing fat along longitudinallyseparated fibers without disrupting the muscle. Bykeeping the muscle and connective tissues grosslyintact, the grafted fat is more likely to remainwithin the muscle. In contrast, injection frombelow results in a cannula course perpendicularto muscle fibers. By disrupting the muscle fibersand septae, the cannula creates a perpendicularpassage through the muscle fibers through whichfat can more easily track down to the submuscularspace, along the path of least resistance (Fig. 10).The absence of deep fascia on the gluteusmuscle has not been described previously. Otherlarge truncal muscles, including the latissimusdorsi and the pectoralis major muscle, exhibitsimilar anatomy, with a superficial subcutaneousfacing fascial component that is dense and a deepcomponent that is nonexistent. Similar to thegluteus muscle, fat injected into the pectoralismuscle can also be presumed to migrate posteriorly into the subpectoral space given the lackof deep fascia to serve as a barricade. Yet unlikegluteal fat injections, fat grafting to the pectoralismuscle has not been associated with pulmonaryfat embolism.39 The likely reason for this is twofold. First, the maximum fat volumes injected intothe pectoralis muscle are on the order of 100 toF108Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Volume 142, Number 5 Gluteal Fat Graft Migrationvolumes of fat preferentially migrate deep to themuscle because of the lack of deep fascial structures acting as a barricade.The migration of fat parallel to or longitudinally between muscle fibers appears to occur bothproximally and distally along the gluteal muscle tosome extent. However, there is higher resistancein this direction because the fibers must separatelongitudinally for fat deposition. This leaves onlythe deep egress as the path of least resistance. Inthis scenario, fat dissects between, or perpendicular to, muscle fibers, spreading only a small distance in the anterior direction before egressinginto the lower pressure submuscular space. Thefat exits the deep surface of the muscle in the areabetween the gluteal vessels and is deposited in thedeep intermuscular space near the sciatic notch.Fat entering the notch causing a wedge can potentially lead to sciatic nerve entrapment with subsequent transient or permanent nerve injury.Fig. 8. Endoscopic anterior septal blowout. After 180 cc of fat,proxy fat is noted to burst through muscle fibers and well up inthe subcutaneous space.150 cc, much less than volumes reported in gluteal fat injections. Without high volumes creatinga high-pressure effect, fat is less likely to egress.Second, unlike the deep gluteal region, the subpectoral space is devoid of significant large andfragile veins that carry with them the potential fordevastating embolisms.Because of the lack of deep fascia lining theundersurface of the gluteus muscle, sufficientvolumes of fat placed in the muscle can migratefreely out of the muscle from its deep surface intothe submuscular plane, along the path of leastresistance. The superficial surface of the gluteusmuscle, in contrast, is lined with a dense superficial fascia that acts as a “backstop” to prohibitintramuscular fat from egressing out of the muscle in the opposite direction, into the superficialsubcutaneous space. Indeed, in the current study,there was no egress through the superficial fasciaeven with recipient-site pressures exceeding 100mmHg. As such, the fascial anatomy of the gluteus muscle creates the basis for the deep intramuscular migration phenomenon, wherein highThe Venous Traction TheoryA mechanism of venous trauma, without directcannula contact injury to the vein, can be postulated to occur as a result of acute venous traction.This may occur when a volume of grafted fat collecting in the submuscular space causes posteriorprojection of the muscle (Fig. 11, left). As the muscle expands posteriorly, it puts traction stretch onthe fixed venous plexus, potentially causing failure, or venous tear, setting up a pressure gradientfor siphoning of fat into the venous system andpulmonary fat embolism (Fig. 11, right).Vascular surgical studies on the tensilestrength of veins suggest that as low as a 7 percent increase in axial length by traction on a filledvein can lead to failure of the conduit.40 Assuming the average length of a superior gluteal veinis 2.5 cm, a submuscular fat collection secondaryto deep intramuscular migration causing venoustraction of (0.07 25 mm) less than 2 mm couldpotentially lead to avulsion of the superior glutealvein.41 As such, deep intramuscular migration–induced traction injury poses another potentialmode of venous injury aside from the obviousdirect cannula trauma.The superficial gluteal fascia, not the muscle,acts as the lynchpin in this polemic. If the fasciaacts as a superficial backstop to force fat deeperduring intramuscular injection, pressure generated during the intramuscular injection can createthe danger. If, in contrast, the superficial glutealfascia acts as an equally powerful deep backstopduring “subcutaneous only Brazilian butt lift” (i.e.,SAFEBBL), it serves as an effective barricade toF119Copyright 2018 American Society of Plastic Surgeons. Unauthorized reproduction of this article is prohibited.
lww14/9/1814:584 Color Fig(s): F1-11Art: PRS-D-18-00447Plastic and Reconstructive Surgery November 2018Video 3. Supplemental Digital Content 3 demonstrates the migration of intramuscular fat in gluteal augmentation. After injection ofpseudofat into the superficial fascia of the gluteus maximus muscle, we show that the pseudofat migrates deep and is depositedwithin the submuscular space. The pseudofat enters deep to themuscle through multiple areas within the muscle. Using an endoscope, we demonstrate that these injections of pseudofat into thesuperficial fascia of the muscle migrated into the space deep themuscle. The posterior fascia of the gluteus maximus muscle actsas a backstop and prevents migration of pseudofat into the subcutaneous space, available in the “Related Videos” section of thefull-text article on PRSJournal.com or, for Ovid users, available athttp://links.lww.com/PRS/D50.prevent subcutaneously placed fat from enteringthe muscle. In this scenario, pressure generatedfrom the subcutaneous injection can be used tohelp guide the dispersion of fat within this space,a concept analogous to “lipotumescence.”42,43 Saiddifferently, “if pressure beneath the fascia is yourenemy, pressure above the fascia is your friend.”Some reading this may be wary of the conceptof creating intentionally high pressures in thesubcutaneous space in gluteal lipoaugmentation.Fig. 9. Inspection of subcutaneous migration. Fat injected into thesubcutaneous (suprafascial) space generated high subcutaneouspressures and migration through the subcutaneous tissue (redarrow), whereas the sub
From Back Bay Plastic Surgery; the Department of Plastic Surgery, University of Texas Southwestern Medical Center; the Dallas Plastic Surgery Institute; and the Venkat Center for Skin and Plastic Surgery. Received for publication February 13, 2018; accepted July 11, 2018. Clinical Implications of Gluteal Fat Graft