Transcription
When Survivors Give BirthOvercoming the Legacy of Childhood Sexual Abuse:The Role of Caregivers and Childbirth EducatorsPenny Simkin, PT
When Survivors Give Birth
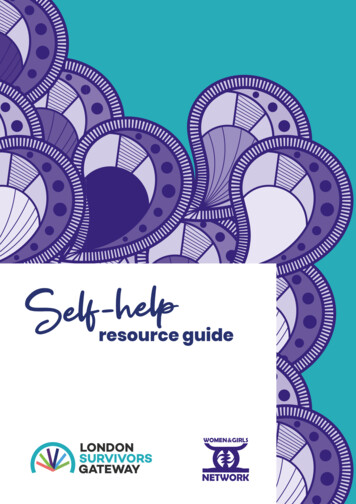
Child MaltreatmentFacts at a Glance2010Note: S orne numhers have been rounded.Nonfatal Cases of Child MaltreatmentChild Maltreatment In 2008, u.s. state and local child protective services (CPS)received 3.3 million reports of children being abused orneglected.' In 2008, CPS reported the approximate rates of childmaltreatment victims: 21.7 per 1,000 for infants less than 1 year old; CPS estimated that 772,000 (10.3 per 1,000) of childrenwere victims of maltreatment. Approximately threequarters of them had no history of prior victimization. 12.9 per 1,000 for 1 year-olds; 12.4 per 1,000 for 2 year-olds; 11.7 per 1,000 for 3 year-olds; Seventy-one percent of the children were classifiedas victims of child neglect; 16 percent as victims ofphysical abuse; 9 percent as victims of sexual abuse; and7 percent as victims of emotional abuse. A non-CPS study estimated that 1 in 5 U.S. childrenexperience some form of child maltreatment:approximately 1 percent were victims of sexual assault;4 percent were victims of child neglect; 9 percent werevictims of physical abuse; and 12 percent were victims ofemotional abuse.'Note: A child is counted each time she or he is a subject of a report, which meansa child mt!Y be counted more than once as a victim of child maltreatment.Gender and RaceDisparities among Children 11.0 per 1,000 for 4 to 7 year-olds; 9.2 per 1,000 for 8 to 11 year-olds; 8.4 per 1,000 for 12 to 15 year-olds; and 5.5 per 1,000 for 16 to 17 year-olds.' Non-CPS studies have reported higher rates of nonfatalchild maltreatment cases, ranging from 15 to 43 per 1,000children.v'Deaths from Child Maltreatment In 2008, an estimated 1,740 children ages 0 to 17 died fromabuse and neglect (rate of 2.3 per 100,000 children).' 80 percent of deaths occurred among children youngerthan age 4; 10 percent among 4-7 year-olds; 4 percentamong 8-11 year-olds; 4 percent among 12-15 yearolds; and 2 percent among 16-17 year-olds. In 2008, some children had higher rates of victimization: African-American (16.6 per 1,000 children). American Indian or Alaska Native (13.9 per 1,000children). 39% of deaths were non-Hispanic White children. Multiracial (13.8 per 1,000 children).' 16% of deaths were Hispanic children.30% of deaths were African-American children. Overall, rates of victimization were slighdy higher forgirls (10.8 per 1,000 children) than boys (9.7 per 1,000children).'References1.Characteristics of Perpetrators Most children are maltreated by their parents versus otherrelatives or caregivers.' Perpetrators are typically less than 39 years of age.! Female perpetrators, mostly mothers, are typically youngerthan male perpetrators.'/:-" "' c,.,.,{ A\ J -"' .;:;:jFor more information,u.s. Department of Health and Human Services, Administration on Children,Youth and Families. Cbitd Mallrea/men/2008 [Washington, DC: U.S. GovernmentPrinting Office, 2010] available at: http://www.acf.hhs.gov.2. Finkelhor D, Turner H, Ormond R, Hamby SL. Violence, abuse, and crimeexposure in a national sample of children and youth. Pediatrics2009; 124:1411-1423.3. Theodore AD, Chang]], Runyan DK, Hunter WM, Bangdewala st, Agans R.Epidemiologic features of tbe physical and sexual maltreatment of children inthe Carolinas. Pediolrics2005; 115: e331-e337.4. Finkelhor D, Ormrod H, Turner H, Hamhy S. The victimization of children andyouth: a comprehensive national survey. Child Mal/reatment 2005; 10: 5-25.please contact:Centers for Disease Control and PreventionNational Center for Injury Prevention and Control1-800-CDC-INFO www.cdc.gov/violenceprevention cdcinfo@cdc.gov
When Survivors Give BirthDefinition of Childhood Sexual AbuseChildhood sexual abuse takes place between a child (anyone under 18 years of age) and someone whomthe child perceives as more powerful than the child herself. It consists of any activity—physical,psychological, or verbal—that causes sexual arousal in the abuser or in someone else.Physical sexual abuse may include intercourse, vaginal or anal penetration by fingers or objects, oral sex,fondling the child, or making the child to fondle the abuser. It may e accompanied by physical violence,or by kindness, favoritism, rewards, or flattery.Psychological sexual abuse may include exposing the genitals, voyeurism, intrusive interest in the child’ssexual development, or forcing the child to view pornographic materials or witness inappropriate sexualactivities.Verbal sexual abuse includes erotic talk or innuendo, accusations of “sexy,” “loose,” or “whore-like”behavior, or other explicit language.Many of these activities leave the child victim hurt, frightened, or confused. She feels that something iswrong, that maybe she is to blame, and is not sure of how or whether to stop it. These feelings areincreased when the abuser is someone she cannot avoid, whom she loves, or on whom she depends forshelter and food. While familiar adults (parents, stepparents, grandparents, or other relatives) are themost likely abusers, others include baby-sitters, mother’s boyfriends, respected elders, neighbors,schoolmates, religious leaders, or strangers. Sometimes a sibling or cousin, or someone whom the girl isdating, who is close in age to the victim, is the abuser.Ritual or cult abuse involves groups of perpetrators and victims in a closed social group. It ischaracterized by many extremely damaging forms of sexual, physical and psychological violence,brainwashing, enforced secrecy, and isolation from the outside world.Simkin, P., & Klaus, P. (2004). When Survivors Give Birth: Understanding and Healing the Effects of EarlySexual Abuse on Childbearing Women.
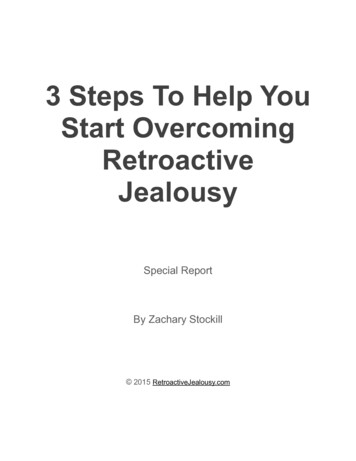
The American College of Obstetricians and GvnecologistsWomen's Health Care PhysiciansCOMMITTEEOPINIONNumber 498 August 2011Committee on Health Care for Underserved WomenThis information should not be construed as dictating an exclusive course of treatment orprocedure to be followed.Adult Manifestations of Childhood Sexual AbuseABSTRACT:Long-term effects of childhood sexual abuse jre varied, complex, and often devastating. Manyobstetrician-gynecologistsknowingly or unknowingly provide care to abuse survivors and should screen allwomen for a history of such abuse. Depression, anxiety, and anger are the most commonly reported emotionalresponses to childhood sexual abuse. Gynecologic problems, including chronic pelvic pain, dyspareunia, vaginismus, nonspecific vaginitis, and gastrointestinal disorders are common diagnoses among survivors. Survivors maybe less likely to have regular Pap tests and may seek little or no prenatal care. Obstetrician-gynecologistscanoffer support to abuse survivors by giving them empoweringduring sensitive examinations.Women who are survivors of childhood sexual abuseoften present with a wide array of symptoms. Frequently,the underlying cause of these symptoms is unrecognizedby both the physician and patient. The obstetrician-gynecologist should have the knowledge to screen for childhood sexual abuse, diagnose disorders that are a resultof abuse, and provide support with interventions. Adultchildhood sexual abuse survivors disproportionately usehealth care services and incur greater health care costscompared with adults who did not experience abuse (1).DefinitionsChild sexual abuse is defined as any sexual activity witha child where consent is not or cannot be given. Thisincludes sexual contact that is accomplished by force orthreat of force, regardless of the age of the participants,and all sexual contact between an adult and a child,regardless of whether there is deception or the childunderstands the sexual nature of the activity. Sexualcontact between an older child and a younger child alsocan be abusive if there is a significant disparity in age,development, or size, rendering the younger child incapable of giving informed consent. The sexually abusiveacts may include sexual penetration, sexual touching, ornoncontact sexual acts such as exposure or voyeurism(2). Legal definitions vary by state; however, state guidelines are available by using the Child Welfare Informa-messages, counseling referrals, and empathic caretion Gateway (www.childwelfare.gov/systemwidellawspolicies/ state).PrevalenceAlthough the exact prevalence is unknown, it is estimatedthat 12-40% of children in the United States experience some form of childhood sexual abuse. Shame andstigma prevent many survivors from disclosing abuse.Incest, once thought to be rare, occurs with alarmingfrequency (3). Survivors come from all cultural, racial,and economic groups (4). Approximately one in fivewomen has experienced childhood sexual abuse (4).From 2006 to 200S, among females aged lS-24 yearswho had sex for the first time before age 20 years, 7%experienced nonvoluntary first sex (5). Twelve percentof girls in grades 9-12 reported they had been sexually abused; 7% of girls in grades 5-S reported sexualabuse. Of all girls who experienced sexual abuse, 65%reported that the abuse occurred more than once,57% reported that the abuser was a family member,and 53% reported that the abuse occurred at home (6).SequelaeSymptoms or behavioral sequelae are common andvaried. More extreme symptoms can be associated withabuse onset at an early age, extended or frequent abuse,incest by a parent, or use of force. Common life events,
like death, birth, marriage, or divorce may trigger thereturn of symptoms for a childhood sexual abuse survivor. The primary aftereffects of childhood sexual abuseinclude the following: EmotionalSymptomsof posttraumaticM1aketihelyabuse, Normalizethe experience.Physiciansmay offerekplanatory statements, such as: "About one womani five was sexually abused as a child. Because theseefperiencescan affect health, I ask all my patientsabout unwantedsexual experiences in childhood"(19).stressSurvivorsmay experienceintrusiveor recurringthoughts of the abuse as well as nightmares or flashbacks. DistortedPhysical EffectsChronic and diffuse pain, especially abdominal or pelvicpain 0), lower pain threshold (7), anxiety and depression, self-neglect, and eating disorders have been attributed to childhood sexual abuse. Adults abused as childrenare four to five times more likely to have abused alcoholand illicit drugs (8). They are also twice as likely to smoke,be physically inactive, and be severely obese (8).Sexual EffectsDisturbancesof desire, arousal, and orgasm may resultfrom the association between sexual activity, violation,and pain. Survivors are more likely to have had 50 ormore intercourse partners, have had a sexually transmitted infection, and engage in risk-taking behaviors thatplace them at risk of contractinghuman immunodeficiency virus (HN) (8,9). Early adolescent or unintendedpregnancy and prostitutionare associated with sexualabuse (10, 11). Gynecologic problems, including chronicpelvic pain, dyspareunia,vaginismus,and nonspecificvaginitis, are common diagnoses among survivors (12-14).Survivors may be less likely to have regular Pap tests andmay seek little or no prenatal care (15).Interpersonal EffectsAdult survivors of sexual abuse may be less skilled atself-protection.They are more apt to accept being victimized by others (15, 16). This tendency to be victimized repeatedly may be the result of general vulnerabilityin dangeroussituationsand exploitationby untrustworthy people.Obstetrician-Gynecologistfor Sexual ViolenceScreeningWith recognitionof the extent of family violence, it isstrongly recommendedthat all women be screened for ahist01 of sexual abuse (15, 17). Patients overwhelminglyfavor niversal inquiry about sexual assault because theyI2."t h e questionnatura. I"Wh en p hvsiYSIClans rouincorporatequestions about possible sexualthey will develop increased comfort (19).IGive the patient control over disclosure. Ask everypatient about childhood abuse and rape trauma, butlet her control what she says and when she says it inorder to keep her emotional defenses intact (19).self-perceptionSurvivors often develop a belief that they caused thesexual abuse and that they deserved it. These beliefsmay result in self-destructiverelationships.of this subject reactionsEmotions such as fear, shame, humiliation,guilt, andself-blame are common and lead to depression andanxiety. report a reluctance to initiate a discussion(18). Following are some guidelines: If the patient reports childhoodsexual abuse, askwhether she has disclosed this in the past or soughtprofessional help. Revelations may be traumatic forthe patient. Listening attentively is important becauseexcessive reassurance may negate the patient's pain.he obstetrician-gynecologistshould consider referr I to a therapist.1jhe examinationmay be postponeduntil anothervisit. Once the patient is ready for an examination,questions about whether any parts of the breast orpelvic examinationcause emotional or physical discomfort should be asked.If the physiciansuspects abuse, but the patientdoes not disclose it, the obstetrician-gynecologistshouldremain open and reassuring. Patients may bring up thesubject at a later visit if they have developed trust in theobstetrician-gynecologist.Not asking about sexual abusemay give tacit support to the survivor's belief that abusedoes not matter or does not have medical relevance andthe opportunityfor interventionis lost (20).Obstetrician-GynecologistIntervention for Sexual ViolenceOnce identified, there are a number of ways that theobstetrician-gynecologistscan offer support.Theseinclude sensitivity with the gynecologic or obstetric visitand examinationin abuse survivors, the use of empowering messages, and counseling referrals.Obstetric and Gynecologic Visits andExaminations in Abuse SurvivorsPelvic examinationsmay be associated with terror andpain for survivors. Feelings of vulnerability in the lithotomy position and being examined by relative strangersmay cause the survivor to re-experiencepast feelings ofpowerlessness,violation, and fear. Many survivors maybe traumatizedby the visit and pelvic examination,butmay not express discomfort or fear and may silently experience distress (20). All proceduresshould be explainedin advance, and whenever possible, the patient should beCommittee Opinion No. 498I
allowed to suggest ways to lessen her fear. For example,the patient may desire the presence of friends or family during the examinationand she has the right to stopthe examinationat any time. Techniques to increase thepatient's comfort include talking her through the steps,maintaining eye contact, allowing her to control the pace,allowing her to see more (eg, use of a mirror in pelvicexaminations),or having her assist during her examination (eg, putting her hand over the physician's to guidethe examination)(20). It is important to ask permissionto touch the patient.Pregnancy and childbirth may be an especially difficult time for survivors. The physical pain of labor anddelivery may trigger memoriesof past abuse (21-23).Women with no prior conscious memories of their abusemay begin to experience emotions,dreams, or partialmemories. Pregnant women who are abuse survivors aresignificantly more likely to report suicidal ideation anddepression (7, 24). There are no consistent data regardingadverse pregnancy outcomes for women with histories ofchildhood sexual abuse.Positive MessagesSome positive and healing responses to the disclosure ofabuse include discussing with the patient that she is thevictim of abuse and is not to blame. She should be reassured that it took courage for her to disclose the abuse,and she has been heard and believed (19, 20).Counseling ReferralsTraumatizedpatientsgenerally benefitfrom mentalhealth care. The obstetrician-gynecologistcan be a powerful ally in the patient's healing by offering support andreferral. Efforts should be made to refer survivors toprofessionals with significant experience in abuse-relatedIssues.Physiciansshould compile a list of experts withexperience in abuse and have a list of appropriatecrisishotlines that operate in their communities.Contactingstate boards of psychology or medicine can be beneficialin locating therapists who are skilled in treating victimsof such trauma. Veterans' centers, battered women's shelters, and rape crisis centers often are familiar with therapists and programs that treat various types of trauma, asare many university-basedcounseling programs. Becauseof the relationship between trauma histories and alcoholand drug abuse, therapists should be skilled in workingwith individuals who have dual diagnoses (25).When discussing with a patient referral to a mentalhealth professional,it is helpful to identify a specificpurpose for the referral. For example, "I would like Dr.Hill to assess you to determine if your past abuse is contributing to your current health problems" is more effective than telling the survivor that her symptoms are allpsychological and that she should see a therapist (26). Itis important to secure the patient's express authorizationbeforj referring her to a mental health specialist, as wellCommittee Opinion No. 498as helping the patient to not feel abandonedwhen a counseling referral is made.or rejectedConblusionFor s me survivors of childhood sexual abuse, there isminirral compromiseto their adult functioning.Otherswill experiencepsychologic,physical, and behavioralsympjorns as a result of their abuse. An understandingof th magnitude and effects of childhood sexual abuse,along I with knowledgeabout screening and intervention methods, can help obstetrician-gynecologistsofferappropriatecare and support to patients with such histories.References1. Leserman J. Sexual abusehistory: prevalence, health effects,mediators, and psychological treatment. Psychosom Med2005;67:906-15.2. Saul J, Audage NC. Preventing child sexual abuse withinyputh-serving organizations: getting started on policiesand procedures. Atlanta (GA): Centers for Disease Controlahd Prevention, National Center for Injury Prevention andControl; 2007.3. 1-fendricks-Matthews M. Caring for victims of childhoodsexual abuse. J Fam Pract 1992;35:501-2.4. 'aden P, Thoennes N. Prevalence, incidence, and cons quences of violence against women: findings from theational Violence Against Women Survey. Research inJrief. Washington, DC: U.S. Department of Iustice, Officeof Justice Programs; 1998. Available at: http://www.ncjrs.gov/pdffiles/ 172837.pdf. Retrieved May 5, 20 II.5. Abma JC, Martinez GM, Copen CEo Teenagers in theUnited States: sexual activity, contraceptive use, and childbearing, National Survey of Family Growth 2006-2008.National Center for Health Statistics. Vital Health Stat 232010;(30):1-79. Available at http://www.cdc.gov/nchs/data/series/sc23/sr23 030.pdf. Retrieved May 5, 2011.6. Schoen C, Davis K, Collins KS, Greenberg L, Des Roches C,Abrams M. The Commonwealth Fund survey of the healthof adolescent girls. New York (NY): Commonwealth Fund;1 997. Available at: ications/Fund%20Report/I997/N ov/The%20Con monwealth%20Fund%20Survey%20of%20the%20Heal h%200f%20Adolescent%20Girls/Schoenadolescentgir s%20pdf.pdf. Retrieved May 5, 201l.17. Scarinci IC,cDonald-Haile J, Bradley LA, Richter JE.Altered pain erception and psychosocial features amongwomen with astrointestinal disorders and history of abuse:a preliminamodel. Am J Med 1994;97:108-18.8. FelittiVJ,AnEdwards V,household ddeath in adulStudy. Am Ja RF,Nordenberg D, WilliamsonDF,SpitzAM,t al. Relationship of childhood abuse andsfunction to many of the leading causes ofs. The Adverse Childhood Experiences (ACE)rev Med 1998;14:245-58.9. Bensley LS, an Eenwyk J, Simmons KW. Self-reportedchildhood se al and physical abuse and adult HTV-riskbehaviors an heavy drinking. Am J Prev Med 2000;18:151-8.3
10. Noll JG, Shenk CE, Putnam KT. Childhood sexual abuseand adolescent pregnancy: a meta-analytic update. J PediatrPsychol 2009;34:366-78.11. Wilson HW, Widom CS. The role of youth problembehaviors in the path from child abuse and neglect to prostitution: a prospective examination. J Res Adolesc 2010;20:210-36.20. Holz KA. A practical approach to clients who are survivorsof childhood sexual abuse. J Nurse Midwifery 1994;39:13-8.21. Grant LJ. Effects of childhood sexual abuse: issues forobstetric caregivers. Birth 1992;19:220-1.12. Britton H, Hansen K. Sexual abuse. Clin Obstet Gynecol1997;40:226-40.22. Waymire V. A triggering time. Childbirth may recall sexualabuse emories. AWHONN Lifelines 1997;1:47-50.13. Paras ML, Murad MH, Chen LP, Goranson EN, Sattler AL,Colbenson KM, et al. Sexual abuse and lifetime diagnosis ofsomatic disorders: a systematic review and meta-analysis.JAMA 2009;302:550-61.23. Rhodesl N, Hutchinson S. Labor experiences of childhoodsexual abuse survivors. Birth 1994;21:213-20.14. Reissing ED, Binik YM, Khalife S, Cohen 0, Arnsel R.Etiological correlates of vaginismus: sexual and physicalabuse, sexual knowledge, sexual self-schema, and relationship adjustment. J Sex Marital Ther 2003;29:47-59.15. Baram DA, Basson R. Sexuality, sexual dysfunction, andsexual assault. In: Berek JS, editor. Berek & Novak's gynecology. 14th ed. Philadelphia (PAl: Lippincott Williams &Wilkins; 2007. p. 313-49.16. Rieker PP, Carmen EH. The victim-to-patient process:the disconfirmation and transformation of abuse. Am JOrthopsychiatry 1986;56:360-70.17. American I College of Obstetricians and Gynecologists.Guidelines for women's health care: a resource manual.3rd ed. Washington, DC: ACOG; 2007.18. Friedman LS, Samet JH, Roberts MS, Hudlin M, Hans P.Inquiry about victimization experiences. A survey ofpatient preferences and physician practices. Arch InternMed 1992;152:1186-90.I19. Wahlen SO. Adult survivors of childhood sexual abuse.Tn: Hend icks-Matthews M, editor. Violence education:4Itoward a solution. Kansas City (MO): Society of Teachersof Family Medicine; 1992. p. 89-102.24. Ainderson G, Yasenik L, Ross CA. Dissociative experiencesahd disorders among women who identify themselves ass xual abuse survivors. Child Abuse NegI1993;17:677-86.I25. Hendricks-Matthews M. Recognition of sexual abuse. J AmBoard Fam Pract 1993;6:511-3.26. ::.fG x n e: ee i 18 1: .men'smedical prob-CopyrightAu ust 2011 by the American College of Obstetricians andGynecologist, 409 12th Street, SW, PO Box 96920, Washington,DC 20090-69 O. All rights reserved. No part of this publication maybe reproduce , stored in a retrieval system, posted on the Internet,or transmitte , in any form or by any means, electronic, mechanical, photocop ing, recording, or otherwise, without prior written permission frorI] the publisher. Requests for authorization to makephotocopies should be directed to: Copyright Clearance Center, 222Rosewood Dive, Danvers, MA 01923, (978) 750-8400.Adult manife tations of childhood sexual abuse. Committee OpinionNo. 498. A encan College of Obstetncians and Gynecologists.Obstet Gyne 012011;118:392-5.Committee Opinion No. 498
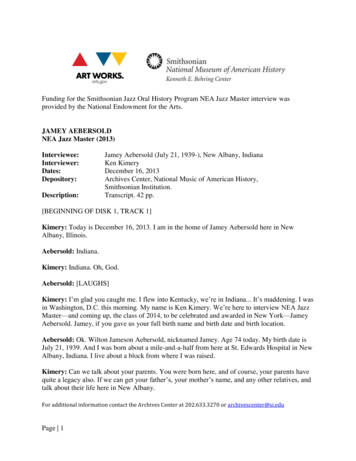
When Survivors Give BirthPossible Impact of Childhood Sexual AbuseSuspect a history of sexual abuse without an obvious physical or psychological cause.Human Responses to Trauma:Note: No single person exhibits all these symptoms. Nor is every person who exhibits one or a few of these symptoms necessarily a survivor ofsexual abuse.2. Physical and Medical1. Sexualsexual dysfunction/addictionsprostitutionteen pregnancy/promiscuityasthmainfertilitychronic gastro intestinal disordersmigraineschronic pelvic pain and other painvaginismusconstipationmusculoskeletal pain and tensionfibromyalgia, chronic fatiguetempero mandibular joint (TMJ)Impact of Childhood SexualAbuse on Adult4. Mental health3. Psycho socialdysfunctional relationshipssubstance abusediscomfort with touchfear of medical, dentalprocedureshigh achievement (nevergood enough)trust issues with authorityfiguresRevised 1/12obsessive compulsive disordersnumerous mental illnessesdissociative disorders, DIDphobiasnightmaresdepressionanxiety (hyper vigilance), panicattackslow self imageanorexia, bulimia, morbid obesitypost traumatic stress or PTSD 1995 by Penny Simkin and Phyllis Klaus. All Rights Reserved
When Survivors Give BirthPossible Impact of Childhood Sexual AbuseSuspect a history of sexual abuse without an obvious physical or psychological cause.Note: No single person exhibits all these symptoms. Nor is every person who exhibits one or a few ofthese symptoms necessarily a survivor of sexual abuse.2. Physical and Medical1. Sexualfear of permanent damage duringbirthfocus on sexual parts of bodydisturbingphobias of needles, vaginal exams,other invasive proceduresexaggerated symptoms ofpregnancyrejection of bodily changes ofpregnancy (evidence of sexuality)repeated miscarriagehyperemesis gravidarumpregnancy induced hypertensionfertility problemspreterm laborImpact of Childhood SexualAbuse on Pregnancy3. Psycho social4. Mental healthbonding failuredesire for abortionstrained relationship withfather/partnerfetus perceived as a parasite orinvaderdifficulty with (mistrust of oroverdependence on caregiverfear of being out of control ordependentfear of birth painfear of not being a good motherrecurrence of previous sexualabuse memoriesanxietydepressiondreams & nightmaresgender preference for baby &caregiver 1995 by Penny Simkin and Phyllis Klaus. All Rights ReservedRevised 1/12
When Survivors Give BirthSuggestions for How to Ask a Client If She Has Ever ExperiencedSexual or Other Abuse:1.On a printed intake form:Please answer the following questions to help us discover if there are potential problemswhich we should discuss together. This information is completely confidential.Is there anything about your sexual development that you’d like to discuss?YesNoHave you ever been or are you now in an abusive relationship (that is, physically oremotionally threatened, insulted, beaten, injured, or made to take part in sexualactivities against your will)?Yes2.NoDirect questioning of the client:“Many women have had unpleasant sexual experiences—being touched or forced intosex—or they have been physically abused. Have you ever experienced anything likethat?”3.Question for the counselor, caregiver, or nurse to ask her/himself (whenthere has been no disclosure):“Would everything that I see, hear, and feel with this client seem more natural orunderstandable, and make more sense if she were in fact a victim of abuse?”
When Survivors Give BirthThe Power Differential between Caregiver and ClientPenny Simkin, PTand Phyllis Klaus, MFT, LCSW1. Physical2. Mental3. EmotionalCaregiver:Pregnant or laboring woman:is uprightis lying downis clothed in prestigiousuniform (scrubs or white coat)is partly naked, wearing hospitalissued gownis strongis weakis free to come and gois restricted to room or in bed withtubes and linesdoes painful or stressful thingsto womansubmitshas knowledgehas less or no knowledgeis the expertis not an expertuses medical jargondoes not understand medical jargondiscusses impersonal risks,benefits, odds, "science"responds with unscientific, personalfeelings and worrieshas tools (machines, tests)depends on caregiver's interpretationis not in painis in painis not in physical dangerfeels in dangeris in controlis stressed, frightenedremains composedis in a position where her publicperson (makeup, clothing, hairstyle)is stripped awayis independentis dependent, vulnerable 1994, 2004Revise d 1 / 1 2
When Survivors Give BirthPossible Impact of Childhood Sexual AbuseSuspect a history of sexual abuse without an obvious physical or psychological cause.Note: No single person exhibits all these symptoms. Nor is every person who exhibits one or afew of these symptoms necessarily a survivor of sexual abuse.1. Sexual2. Physical and Medicalfear of male caregiver (orfemale)vaginal exams &instruments as rapenakedness, modesty issuesbaby in vagina (bodymemories)postdates pregnancy?(induction)vomiting in labor?dysfunctional labor(augmentation, cesareansection)excessive pain and tensionImpact of ChildhoodSexual Abuse on Labor3. Psycho social4. Mental healthcontrol issues (re: management &self control)"fighting" staff & laborpassivity, submission, "easy, goodpatient"abandonment, isolation issueslack of cooperation with staff,pushing, positionsbonding difficultiesdependency on partner, doula,caregiverfear, repugnance of blood,secretionsfear of the unknown, danger"body memories of abuse" &intense distressambivalence re: c/s , epiduralfear of invasive procedureshypervigilancetraumapanicdissociation ("withdraws,""goes away") 1995 by Penny Simkin and Phyllis Klaus. All Rights Reserved
When Survivors Give BirthPotential “Triggers” That May Cause Anxiety or Body Memories forChildhood Sexual Abuse Survivors During Pregnancy, Birth, and Postpartumby Penny Simkin, PTand Phyllis Klaus, MFT, LCSWFollowing are some specific actions, events, or factors that may occur during childbirth. Each has raisedundue anxiety, fear, resistance, or tension in some survivors. Caregivers should recognize that when theirclients react extremely to several of these items, it may indicate a history of sexual abuse, which mayexplain their apparently extreme reactions.Match the theme to the trigger:1. Control and loss of controlSelf-control (crying out, struggling, being agitated)Restraint (being trapped, tied down, hooked up)Control over what is done to her2. Pain, injury, and damage to her body; invasion3. Dependency on partner, doula caregiver4. Mistrust of strangers5. Shame and being judged over body image, behavior, "weakness", secretions6. Exposure (modesty, people staring, looking and feeling inside)7. Ignorance: fear of unknownIntrinsic to Pregnancy1. Hormonal/bodily changes2. Evidence of sexuality3. Conflicting feelings (shame, anxiety,excitement, worry, self-disgust)4. Necessity of prenatal visits (client mayavoid coming). Many women out of touchwith feel
as victimsof child neglect; 16 percent asvictims of physical abuse; 9 percent as victims of sexual abuse; and 7 percentas victims of emotional abuse. A non-CPS study estimated that 1in 5 U.S.children experiencesome form of child maltreatment: approximately 1percent were victims of sexual assault; 4 percent were victims of child neglect .