Transcription
Bull. Org. mond. San)e 1969, 41, 749-760Bull. Wld Hlth Org.Smallpox Vaccination by Intradermal Jet Injection*1. Introduction, Background and Results of Pilot StudiesJ. DONALD MILLAR,1 RONALD R. ROBERTO,2 HERTA WULFF,3 HERBERT A. WENNER4& D. A. HENDERSON 5Jet injection has met with great success in the rapid and effective mass administration ofseveral immunizing agents. The recent development of a jet injector nozzle specificallydesigned for intradermal inoculation suggested the possible extension of jet injector methodology to mass smallpox vaccination. A total of 156 volunteer subjects, 16 unvaccinated and140 vaccinated more than 5 years previously, received either undiluted smallpox vaccineby the multiple-pressure technique, or 0.1 ml of various dilutions of smallpox vaccine byjet injector using the new nozzle. Cutaneous and serological responses in revaccineesrevealed that jet injection of diluted vaccine with a titre of 107 TCID50/ml was as effectiveas multiple-pressure inoculation of undiluted vaccine. Among the small number ofprimaryvaccinees, jet injection of diluted vaccine with a titre of 106 TCID5o/ml appeared as effectiveas multiple-pressure inoculation of undiluted vaccine. No complications of vaccinationoccurred.The findings confirm the utility of the intradermal nozzle for jet injection of smallpoxvaccine. In view of the speed of administration and the economy of vaccine, it is suggestedthat there is a distinct role for jet injection in global smallpox eradication efforts. Furtherstudies on larger numbers of unvaccinated subjects and on persons with significant residualvaccinial immunity are needed to define the optimal concentration of vaccine for massvaccination by iet injection.Jet injection is now accepted as an effective, safe,and uniquely rapid means of inoculating manybiological agents. Until recently, only subcutaneousor intramuscular injection could be performed withjet-injection equipment; thus the advantages of thetechnique were not available to the administration ofsmallpox vaccine, which undergoes multiplication inthe epidermis. In 1962, Ismach and his associates 6developed a special nozzle for the jet injector topermit the dispersion of inoculum in the dermis andepidermis. This nozzle, applicable to smallpoxvaccination, offered the possibility of a revolutionarychange in the potential speed and effectiveness ofmass smallpox vaccination campaigns. With theview that smallpox vaccination by jet injection mightfavourably affect the progress of global smallpox* From the SmallpoxEradication Program, NationalCommunicable Disease Center, Health Services and MentalHealth Administration, Public Health Service, US Department of Health, Education, and Welfare, Atlanta, Ga., andSection of Virus Research, Department of Pediatrics, Schoolof Medicine, University of Kansas, Kansas City, Kans., USA.These studies were supported in part by the US ArmyResearch and Development Command, Office of the SurgeonGeneral, Department of the Army.1 Director, Smallpox Eradication Program, and formerlyEpidemic Intelligence Service Officer, National Communicable Disease Center, Public Health Service, US Departmentof Health, Education, and Welfare, Atlanta, Ga., USA.2 Formerly Chief, SmallpoxInvestigations Unit, SmallpoxEradication Program, National Communicable Disease Center, Public Health Service, US Department of Health,Education, and Welfare. Present address: State Departmentof Public Health, Berkeley, Calif., USA.3Fornrerly Research Fellow in Pediatrics, University ofKansas Medical Center, Kansas City, Kans. Present address:Ecological Investigations Program, National CommunicableDisease Center, Kansas City, Kans., USA.4Research Professor of Pediatrics, University of KansasMedical Center, Kansas City, Kans., USA. ResearchCareer Awardee, National Institutes of Health.5 Formerly Chief, Smallpox Eradication Program, NationalCommunicable Disease Center, Public Health Service, USDepartment of Health, Education, and Welfare, Atlanta,Ga., USA. Chief Medical Officer, Smallpox Eradication,World Health Organization, Geneva, Switzerland.6 At the US Army Medical Equipment Research and Development Laboratories, Fort Totten, New York, N.Y., USA.2430749-
750J. D. MILLAR AND OTHERSeradication campaigns, the National CommunicableDisease Center initiated studies in 1963 to comparethe efficacy and safety of smallpox vaccineadministered intradermally by jet injection withvaccination performed by the traditional multiplepressure technique. This paper reviews relevantprevious work and describes the results of pilotcomparative studies.BACKGROUNDIntradermal vaccination by jet injection differs inconcept from the traditional methods in 2 ways; theantigen is administered intradermally rather thanpercutaneously, and by jet-injection equipmentrather than with the aid of the scarification needle.Intradermal administration of smallpox vaccine bysyringe and needleThe intradermal administration of smallpoxvaccine held great interest for workers early in thiscentury. Wright (1918), seeking a method forconsistent satisfactory vaccination, reported successin the intradermal inoculation of smallpox vaccinediluted 1: 2 in distilled water. To 54 previouslyunvaccinated men, he administered diluted vaccineby intradermal injection and simultaneously vaccinated them by the scratch technique with undilutedvaccine. A total of 85 % of the intradermalinoculations produced " takes " while only 17% ofthe scratch vaccinations did so. Using this method,Wright felt that there was a reduced chance ofbacterial infection, and he considered that thedelivery of a known quantity of virus offered distinctadvantages as well.Roberts (1932), after reviewing studies of intradermal vaccination, concluded that successfulintradermal vaccination resulted in immunizationsimilar to that following successful vaccination byscarification. However, Roberts and other earlyworkers were concerned with the potential risk ofsecondary infection following intradermal injectionof smallpox vaccines which were heavily contaminated with bacteria. While isolated incidents ofabscess formation were reported (Kirstien, F., citedby Roberts, 1932), no major problems developed.The development by Rivers (1931) and byGoodpasture & Buddingh (1933) of vaccine virusescultured in chick embryo tissues and free frombacterial contamination increased the interest in theuse of intradermal vaccination. In initial studies,intradermal vaccination with the Rivers vaccineappeared to produce erythema and induration, butnot vesiculation (Rivers & Ward, 1935; Rivers,Ward & Baird, 1939); Ellis & Boynton (1939)showed in 3000 college students that successfulintradermal vaccination with the Rivers strainresulted in typical primary vesicles in no waydifferent from those observed following traditionalscratch and multiple-pressure methods. Since 1940,only a few scattered reports have appeared (Pierce &Willoughby, 1943; McCowan, 1940; Victoriano,1953; Rosenbusch, 1953; Vox, 1953).The earlier workers, however, showed convincingly that (1) intradermal inoculation of potentsmallpox vaccine produces successful vaccination;(2) the systemic and cutaneous responses areclinically similar to those produced by scarification;(3) diluted vaccines can be administered intradermally without a reduction in the " take rate ";and (4) vaccination in this manner is notaccompanied by an unusually high incidence ofpyogenic complications, despite the use of heavilycontaminated vaccines.Because of failure to demonstrate any notableadvantages of intradermal vaccination, investigatorslost interest in the technique. Nevertheless, theseearly findings became relevant with the advent of ajet-injection technique for intradermal inoculation.The development ofjet injectionThe history of the development of jet injection hasbeen reviewed by Hingson, Hamilton & Rosen(1963). While the principle of jet inoculation wasintroduced over 100 years ago, widespread application of the technique came only after the SecondWorld War. The most promising large-scale application has been in mass administration of immunizingagents, e.g., typhoid, poliomyelitis, diphtheria-pertussis-tetanus (DPT), and other antigens (Hingston,Hamilton & Rosen, 1963; Batson, Wall & Landy,1949; Lipson et al., 1958; Anderson, Lindberg &Hunter, 1958; Warren et al., 1955).As the design of jet-injector nozzles permitted onlysubcutaneous or intramuscular (rather than dermal)delivery of antigen, little work was attempted withsmallpox vaccine. Elisberg, McCowan & Smadel(1956), using a hand-operated, multiple-dose jetinjector equipped with the standard subcutaneousnozzle, inoculated 21 previously unvaccinatedindividuals with a chorio-allantoic membrane(CAM) vaccinia virus preparation containing 105CAM infectious units. Altogether, 20 subjectsdeveloped typical primary cutaneous reactions; sera
SMALLPOX VACCINATION BY INTRADERMAL JET INJECTION. Iobtained from 14 of them showed haemagglutination-inhibition (HI) antibodies. Of 10 revaccinatedadults, 2 showed " accelerated" reactions while theremaining 8 had " immediate" reactions., Serological evidence of successful revaccination wasfound in 2 out of 9 individuals whose sera werestudied for HI antibodies. Subcutaneous inoculation of the same vaccine by syringe and needlerevealed no cutaneous or serological response.These workers vaccinated 1056 military recruits byjet injection; only 1 failed to develop either an"immediate ", an " accelerated " or a " primary"reaction. The results indicated that smallpoxvaccine administered in this way yielded satisfactoryresults without untoward reactions. Success wasattributed to the small amount of virus trapped inthe superficial skin layers as the stream of vaccinepassed through to the deeper tissues.Meyer et al. (1964) attached a short plastic sleeveto the nozzle of the injector, thereby raising it fromthe skin, with the expectation that an increasedamount of vaccine would be delivered superficially.Among 300 unvaccinated children who received1.5 x 106 tissue culture infective doses (TCID,O) ofsmallpox vaccine in this manner, 97 % developedtypical primary cutaneous vaccinial reactions. Of237 children, 99.6 % showed evidence of seroconversion by HI antibody determination.A nozzle specifically designed to deliver injectedmaterials intradermally was introduced by Ismach in1962. Benenson & Ismach (personal communication) observed that jet injection with this nozzleproduced a small superficial bleb similar to thatwhich followed intradermal inoculation with syringeand needle. In July 1962, Millar & Henderson(unpublished data), using the new device, inoculated41 previously vaccinated young adults with a dilutedsmallpox vaccine. A total of 32 subjects hadcutaneous evidence of satisfactory revaccination8 days later. These findings prompted a furtherclinical and serological trial of intradermal administration of smallpox vaccine by jet injection.Objectives of the present studyThe study was designed to compare the efficacy ofvaccination performed by the traditional multiplepressure technique with vaccination performed by jetinjection, employing the newly developed " intradermal nozzle ". Moreover, an attempt was made todefine the vaccinia virus concentrations that wouldbe adequate to ensure successful vaccination by thismeans.751MATERIALS AND METHODSStudy populationA total of 156 adult males were recruited on thebasis of vaccination history from volunteers in theAtlanta Federal Penitentiary and the Georgia StatePrison; none claimed vaccination within theprevious 5 years. In all, 140 bore scars of previoussuccessful vaccinations; the remaining 16 hadneither old vaccination scars nor a history ofvaccination and were considered to be unvaccinated.The 140 subjects with vaccination scars weredivided into 6 approximately equal groups(Table 1). Group 1 was vaccinated with undiluted,reconstituted lyophilized smallpox vaccine by multiple-pressure technique; the remaining 5 groupswere vaccinated with the jet injector, receiving 0.1 mleach of different dilutions of the vaccine, designatedrespectively, ID-Jet 1, ID-Jet 2, ID-Jet 3, ID-Jet 4and ID-Jet 5. The 16 primary vaccinees were soallocated that at least 1 subject received vaccinationby each of the 6 alternative methods.VaccineLyophilized calf lymph smallpox vaccine from asingle commercial production lot 1 meeting standards set by the Division of Biologics Standards,National Institutes of Health, was used for allvaccinations. The vaccine, when titrated in primaryrhesus monkey kidney tissue culture tubes using halflog dilution steps, had a titre of 108-5 TCID50/ml.For multiple-pressure vaccination, this vaccinewas reconstituted with the standard commercialdiluent containing 50% glycerol (USP) and 0.25%phenol (USP) in sterile water. Vaccine for jetinjection use was prepared as follows. To a vialcontaining 0.3 ml of smallpox vaccine reconstituted for multiple-pressure vaccination, 10 ml ofHanks' solution was added. The preparation wastermed the " ID-Jet 1 " vaccine. Sequential 10-folddilutions were made in Hanks' solution yieldingvaccines designated " ID-Jet 2 ", " ID-Jet 3 ", " IDJet 4" and " ID-Jet 5 ". Calculated virus concentrations of these diluted vaccines are shown in thesecond row of Table 1.Vaccination techniquesEach subject was inoculated on the left deltoidarea, either by multiple pressure or by intradermal1 Kindly provided as Dryvax, Lot No. 177101A, byWyeth Laboratories, Inc., Marietta, Pa., USA.
752J. D. MILLAR AND OTHERSTABLE IPREVACCINATION CHARACTERISTICS OF SUBJECTS BY GROUPGroupsCharacteristic 12Vaccination methodVaccine titre bNumberAge:MeanRangeMean No. of years since lastvaccinationPrevaccination neutralizingantibody titre: 1010-4041-160161-640 640Geometric mean titrea3Multiplepressure(undiluted)8.523ID-Jet I aID-Jet 2 aID-Jet 3 aID-Jet 4 aID-Jet 5 a7.0 334023127038110252227Intradermal jet injection of 0.1 ml of vaccine.b Expressed as log TCIDS"/ml.c The titre of 7.0 reflects the 1: 33 volumetric dilution described in the text.et injection. Multiple-pressure vaccinations wereperformed by I vaccinator with a single-pointedneedle making 30 tangential pressures through adrop of undiluted vaccine. Intradermal jet-injectionvaccinations were performed with an automatichypodermic jet-injection apparatus,1 equipped withthe new intradermal nozzle. The mechanicalprinciples of injector operation and design have beendescribed by Benenson (1959) and a diagram of theintradermal nozzle is given in Hendrix, Nichols &Hirsch (1966).The nozzle consists essentially of a centralinjection tip with an eccentric aperture and asurrounding cup. The nozzle cups the skin into asmall mound and angles the injection streamtangentially into the superficial skin layers. Roberto(unpublished data, 1966), after injecting Indian inkinto the skin of pigs, showed that while smallamounts of injected material reached the subcutane1 Manufactured by the Scientific Equipment Manufac-turing Corporation, Lodi, N.Y., USA.ous tissue, the bulk of vaccine was contained withinthe dermal layer.In the present studies, jet-injection inoculationswere performed with the dose adjustor set at the 0.1ml calibration. The nozzle was placed against theskin of the left deltoid area with the injector atapproximately right angles to the long axis of thearm. The arm and injector were held firmly in placeduring the injection. In most subjects, a drop ofvaccine remained on the surface of the skin afterinoculation.Evaluation of resultsThe cutaneous responses following revaccinationwere interpreted according to the recommendationsof the WHO Expert Committee on Smallpox (1964,p. 20). A " major reaction " is termed " one which,on examination one week (six to eight days) later,shows a vesicular or pustular lesion or an area ofdefinite palpable induration or congestion surrounding a central lesion, which may be a scab or ulcer ".
SMALLPOX VACCINATION BY INTRADERMAL JET INJECTION. 1Anything less than this is judged an " equivocalreaction ". The "major reaction" is held to beindicative of virus multiplication (and the consequent development of immunity) while the " equivocal reaction " may be due to a degree of pre-existingimmunity sufficient to prevent virus multiplication,to application of inactive vaccine, or to faultytechnique.In this study, the site of vaccination was examinedimmediately following inoculation and then daily forthe next 14 days. The extent of erythema andinduration of the developing lesions, as well as thepresence or absence of vesiculation, were observedand recorded daily. Photographs were made of thelesions at each examination.The neutralizing antibody response was measuredas an additional index of response to vaccination.Previous work by McCarthy, Downie & Bradley(1958) suggests that neutralization antibody issuperior to either complement-fixing or haemagglutination-inhibition antibody for quantitative assay ofserological responses.A 10-ml sample of blood was obtained from eachsubject immediately prior to vaccination and again30 days after the vaccination. Sera were separated,frozen, and transported in solid carbon dioxide tothe laboratories of the National CommunicableDisease Center, Atlanta, Ga. They were kept frozenat -20 C until serological tests were performed.The neutralizing antibody titre was determined bya method described by Cutchins, Warren & Jones(1960), modified as follows:Dried smallpox vaccine,' passed in monkey kidneytissue cultures, was used as antigen. The maintenance fluid for monkey kidney tissue culture tubeswas high-cystine, altered Eagle's medium (the pHbeing adjusted to 7.4 with sodium bicarbonate).After inactivation (30 minutes at 560C) the serawere diluted in 4-fold steps in phosphate-bufferedsaline (PBS) starting with the dilution 1: 4. Virusdilutions (30-60 pock-forming units per 0.1 ml) weremade in PBS with 200% skimmed milk. Equalamounts of virus and serum dilutions were incubatedfor 24 hours at 36 C in a water-bath. Four rhesusmonkey kidney tissue culture tubes were inoculatedwith each virus-serum mixture. Cultures wereincubated at 36.5 C for 40 hours. Antigen controls,a rabbit immune serum control and a negative serumcontrol, were incorporated in each test.1 Dryvax; Wyeth Laboratories.753After the 40-hour incubation period, 0.2 ml of a0.04% solution of neutral red in distilled water wasadded to each culture. The tubes were thenincubated in a stationary rack for an additional30 minutes at 37 C and 1 hour at room temperature(20 C-22 C). Plaques with a diameter at least 1 mm,which developed during the first infectious cycle,were counted.The average number of plaques in the viruscontrols (6 cultures) and in the tubes which wereino ulated with the virus-serum mixture wascalculated. The percentage of plaque inhibition inthe different serum dilution steps was plotted onprobability paper against the logarithm of the serumdilution and the 50% plaque reduction titre wasdetermined.RESULTSCharacteristics of study groupPrevaccination characteristics of the groups ofvolunteers studied are summarized in Table 1. Eachgrouping was considered essentially equivalent in allrelevant aspects at the outset of the study.Performance of the jet injectorThere were no mechanical failures of the injectorin inoculating any of the subjects. Immediately aftera jet injection, a clearly visible superficial bleb waspresent at the inocu'ation site in each inoculatedindividual. A small amount of liquid remained onthe skin surface at the inoculation site indicating thatsomewhat less than 0.1 ml had actually penetratedthe epidermis.Evaluation Qf clinical resultsRevaccinees. Lesions following jet injection werenot grossly different in character from thosefollowing the multiple-pressure technique. In mostinstances erythema and induration developed duringthe first 24 hours, with maximal skin responses notedbetween the second and eighth days.The frequencies of cutaneous responses on day 7are summarized in Table 2, using the WHO ExpertCommittee on Smallpox (1964) criteria for interpreting revaccination reactions. All subjects vaccinated by the multiple-pressure technique withundiluted vaccine, and all those vaccinated with theID-Jet 1 vaccine by jet injection, developed majorreactions. A progressively diminishing proportionof subjects in groups 3, 4 and 5 showed majorreactions; no subject developed a major reactionfrom the ID-Jet 5 vaccine. Conversely, equivocal
754J. D. MILLAR AND OTHERSTABLE 2CUTANEOUS REACTIONSa IN REVACCINATED SUBJECTSIGroupVaccination method1Multiple pressure (undiluted)ID-Jet 1I D-Jet 2ID-Jet 3ID-Jet 4ID-Jet 523456aNumber ofVaccinesubjectstitre b 7 (2) c23 (8) c25 (13) c-277195100Criteria of the WHO Expert Committee on Smallpox (1964).TCID5o/ml.b Expressed as logc Values in parenthesesindicate number of subjects with no dermal response.reactions occurred with increasing frequency ingroups 3, 4, 5 and 6. Among subjects receiving theID-Jet 5 vaccine, over half developed no reaction atall.No complications of vaccination were observed.During the first 7 days following vaccination, a totalof 33 individuals complained of sore arms and 5developed axillary lymphadenopathy. These occurred most frequently among those vaccinated bymultiple-pressure or by jet injection with ID-Jet 1and ID-Jet 2 vaccines (Table 3).Primary vaccinationAmong the 16 adults apparently vaccinated for thefirst time, 12 developed typical Jennerian vesicles.These included all of those who received either theundiluted vacci4he by multiple pressure, the ID-Jet 1vaccine or the ID-Jet 2 vaccine. Only 1 of the 3individuals vaccinated with the ID-Jet 3 vaccinedeveloped a primary take; no takes were recorded in2 subjects receiving the more dilute vaccines(Table 4).Results of serological evaluationRevaccinees. There was a wide range ofprevaccination neutralizing antibody titres in eachgroup. No single group, however, had more than4 subjects with prevaccination titres higher than 160;the prevaccination geometric mean antibody titresfor the separate groups were similar, ranging fromTABLE 3ARM PAIN AND AXILLARY LYMPHADENOPATHY AMONG REVACCINATED SUBJECTSaExpressed as logTCIDso/ml.
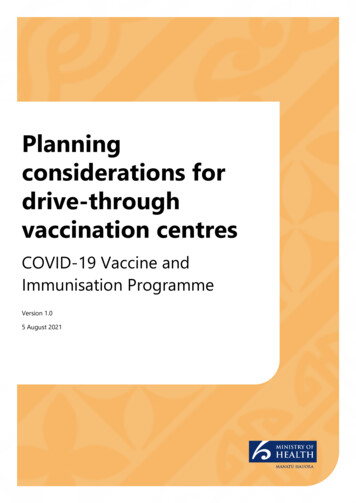
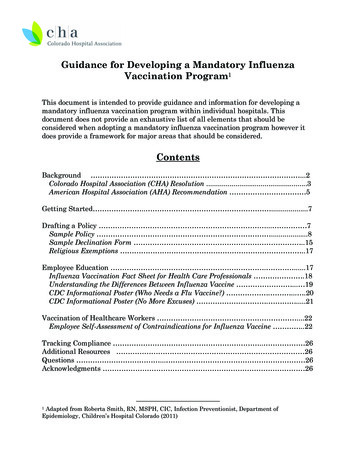
755SMALLPOX VACCINATION BY INTRADERMAL JET INJECI1ON. ITABLE 4NEUTRALIZING-ANTIBODY RESPONSE IN REVACCINATED SUBJECTS BYCUTANEOUS REACTION AND PREVACCINATION NEUTRALIZING-ANTIBODY TITREGroupVaccination methodNumber ofVacc*ne subjects titrePrevaccinationPrevaccin ationtitres: aantibodymajor reactionsantibody titres: aequivocal reactions 160IMultiple pressure (undiluted) 8.5232I D-Jet 17.02236.0225.0245I D-Jet 2I D-Jet 3I D-Jet 44.0246 I D-Jet 53.0254aExpressedb Number ofb 160b16/2017/1912/151/60/1f1 /31/30/10/1-ITotalIb%ob ;1 60b 160 oab 17/23 - - - i17/23 73.9l18/2218/22 81:.812/16 0/32/32/614/22 63.68.31/70/31/141/172/2400110/190/40/230/240 /4 0/25 0/25 0 - 0/21log TCIDso/ml.subjects with 4-fold antibody rise/number of subjects with dermal reaction.as22 to 38. The geometric mean titres followingvaccination were strikingly higher in groups 1, 2, and3 than in the remaining 3 groups (240, 462, 272,compared with 28, 20, 22, respectively).An analysis of neutralizing antibody responses ispresented in Table 4 and Fig. 1-4. Correlationsbetween 4-fold or greater increases in antibodyand cutaneous responses are presented. In thesummation of results in all groups, a correlationbetween increase in antibody and an observed majorcutaneous reaction is apparent. Of 69 subjectsdevelopi,ng. major reactions, 48 (69.2 %) showedevidence of a 4-fold or greater increase in antibodytitre. Of the 71 individuals who were judged to haveequivocal reactions, 3 (4.2 %) developed 4-foldincreases in antibody.Differences between groups 1, 2, and 3 are notsignificant. A sharp decline, however, is noted bothin serological and cutaneous responses between the,first 3 groups and those receiving ID-Jet 3 vaccine.No response was observed among those receivingID-Jet 4 and ID-Jet S vaccines.Primary vaccinees. Among the 12 individuals whodeveloped primary reactions, 7 developed detectableneutralizing antibody (Table 5).TABLE 5ADULT PRIMARY VACCINATIONS; CUTANEOUS ANDNEUTRALIZING-ANTIBODY RESPONSESNeutralizingGroupValCCi nation methodtitre asubjcinteds10 8.s10 7210 '105,10 4 10 32IMultiple pressure (undiluted)2I D-Jet 13I D-Jet 2ID-Jet 3I D-Jet 4 ID-Jet 54b6aExpressed as TCID50/Ml.irvesicle N converters range212055444216-248-163101O 0O 0
D. MILLAR AND OTHERS J.7567560 0 CZwNZ 'E04 40 -0-0 .0 *F-0 ui 0 0)0(L I.I.00 a- -0 z00 0OEu *0000 1 ci0400-3.J44 !4U014DA.4SODAJ60C 1W000-0.0.1)11 U0I10UII 0A-1SO. 4.- .-----u.
757SMALLPOX VACCINATION BY INTRADERMAL JET INJECTION. 10zC b \ z wz EZZEL,.10-'0Zwa.\\CI 0NRt Z 08 i041! U0140DUi)DA-4Sod joK0141(E50jU0i40Ui 0A-4S0CDd0 0.0z Uz FF-\j L)o0 0. 6C,s0HOzC 4-- 7 o 0. 0DI0 x 0oF--Fuzow)0)c OJ4!4U014OUl-3D0A-4SodJo-mIL.Oaj4!4 013 U01IUl)0UIDA-jS0601I
758J. D. MILLAR AND OTHERSDISCUSSIONVaccination confers immunity to smallpox. Atleast 4 factors seem to be involved in recovery fromvaccinial infections and probably play a role inprotection against smallpox: (1) humoral antibodyproduction (McCarthy, Downie & Bradley, 1958);(2) a delayed hypersensitivity phenomenon (Friedman & Baron, 1961; Pincus & Flick, 1963);(3) interferon production (Wheelock, 1964; ScientificCommittee on Interferon, 1962; and (4) cellularresistance measurable in vitro (Stienberger &Rights, 1963). Insufficient evidence is at hand toassess the importance of any single factor, or todetermine the synergistic effect of the variousfactors.Except for natural challenge with variola virus, thedefinitive test of immunity, cutaneous and neutralizing antibody responses are the most useful indicesin man for comparing smallpox vaccines, dilutionsof vaccine, and techniques of administration. Thevisible skin response presumably provides information reflecting the phenomena of delayed hypersensitivity and interferon production, which often exert aprimary effect in local control of vaccinial infections;the serological evaluation provides informationregarding protection which may be afforded byhumoral antibody.The 'present study demonstrates that successfulintradermal vaccination by jet injection produces aresponse which is indistinguishable, clinically andserologically, from that following successful vaccination by the multiple-pressure technique. Within thestatistical limits set by the small numbers involved,there is no evidence to suggest a difference withrespect to the safety of the 2 techniques.In this study, the ID-Jet 1 vaccine administeredintradermally by jet injection produced results inrevaccinated persons as good as, or better than, thosewith undiluted vaccine administered by multiple pressure. From the very limited number of observationsin primary vaccination, it would appear that the IDJet 2 vaccine might be as effective for primary vaccination as undiluted vaccine by the multiple-pressuretechnique.This study showed a reasonably consistentrelationship between neutralizing antibody anddermal response patterns. The WHO criteria forinterpreting dermal responses are useful in the mainfor classification of cutaneous responses in " late"revaccination, i.e., in persons with limited residualimmunity. However, the antibody and dermalresponse patterns were not always in agreement. Asnoted, only 70% of the subjects developing majorreactions also developed 4-fold or greater neutralizing antibody rises, and nearly 5% of those withequivocal cutaneous responses did develop 4-foldincreases in antibody titre. Thus, in assessing thefull effect of the vaccine, it,is important to measureas many of the parameters of response tovaccination as possible.The differences in response to ID-Jet 1 and IDJet 2 vaccines are worthy of attention. The ID-Jet lvaccine appears to produce optimal results inrevaccinees, as well as primary vaccinees. Responsesamong revaccinees to ID-Jet 2 vaccine appear to beslightly reduced.The quantity of virus particles needed to ensure asuccessful vaccination by jet injection may becalculated. Since the minimum required titre ofvaccine appears to be 106 107 TCID50/ml, theminimum quantity of delivered virus (0.1 ml) toensure successful vaccination of subjects with limitedresidual immunity is approximately 105 106 TCID50.Espmark (1965), in studying the multiple-pressuretechnique in man, showed that the vaccine titresneeded to ensure successful takes in 50% of " late "revaccinees varied from 105-9 TCID50/ml to 106.4TCID50/ml. The theoretical vaccine titre requiredfor a 50 % take rate in our studies was approximately105.6 TCID50/ml,' or about 1/2 log lower than thatdetermined by Espmark. This difference probablyrelates to the fact that virtually all the vaccine virusdose' is administered by jet injection compaired withthe unknown (but obviously lower) quantity of virusdelivered through the skin by the multiple-pressuretechnique.The limited number of primary vaccinationsreported demands an extension of these studies withthe jet injector to deal with this important group.Studies of recent revaccinees will assist in definingmore precisely minimum doses of vaccinia virusrequired for field use. It now appears certain,however, that the advantages of mass smallpoxvaccination by jet injection, that made jet injectionso popular for mass inoculations of other antigens,
Eradication Program, National Communicable Disease Cen-ter, Public Health Service, US Department of Health, . (DPT), andother antigens (Hingston, . Lipson et al., 1958; Anderson, Lindberg & Hunter, 1958; Warrenet al., 1955). Asthedesignofjet-injectornozzlespermittedonly subcutaneous or intramuscular (rather than dermal) delivery of antigen .