Transcription
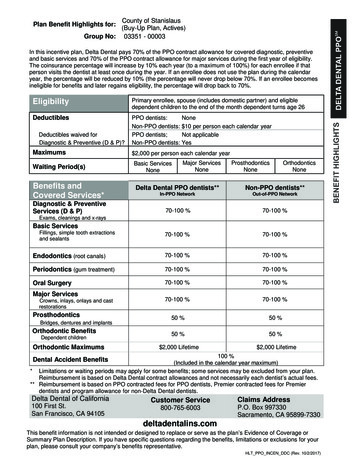
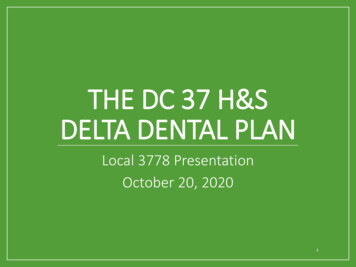
Delta Dental EPOCity & County of Denver #6026 – EPO PlanMAXIMUM BENEFIT - Calendar Year MaximumUnlimited – See copayment schedule for additional details.Orthodontic LifetimeUnlimited – See copayment schedule for additional details.CALENDAR YEAR DEDUCTIBLENo DeductiblePPO DENTISTBENEFIT INFORMATION (subject to Delta Dentalguidelines)COVERED SERVICES*DIAGNOSTIC AND PREVENTIVE SERVICESCo-payment (see attachedschedule of Co-paymentlistings)Oral Exams (all exam typesincluding consultation) &CleaningsTwice in a 12-month period.X-RaysBitewings: Once in a 12-month period / Full Mouth: Oncein a 60-month period.FluorideOnce in a 12-month period, through age 15Space MaintainersFor posterior primary teeth for children through age 13SealantsOnce per tooth in 36 months on unrestored molars inchildren through age 14Fillings (Amalgam, Resin &Composite)Benefits on the same surface limited to 1 in 12 monthsOral Surgery (Extractions)Please see benefit booklet for detailsGeneral AnesthesiaBenefit with covered Oral Surgery onlySurgical Periodontics (gum)Benefit once every 36 monthsRoot Canal TherapyPlease see benefit booklet for detailsCrownsBenefit 1 in 60-months on same tooth. Not a benefit forchildren under age 12.Benefit 1 in 60 months. Not a benefit under age 16.BASIC SERVICESCo-payment (see attachedschedule of Co-paymentlistings)MAJOR SERVICESCo-payment (see attachedschedule of Co-paymentlistings)Dentures, Partials, BridgesBridge/Denture RepairDenture Rebase/RelinePlease see benefit booklet for detailsBenefit 6 month after initial insertion and once in 36months.ORTHODONTICS (Adult and Child)Co-payment (see attachedschedule of Co-paymentlistings)Complete Orthodontic EvaluationActive Orthodontic TreatmentThe EPO benefits are based on the PPO Schedule of Allowance less any co-pays. Only services listed in the copayment schedule arecovered. You must see a PPO dentist for services as there is no benefit outside of the PPO network.Open Enrollment applies. Members may add coverage once per year.Find a PPO Dentist: deltadentalco.com or call (800)610-0201.This is a brief description of services covered under your dental plan. Please refer to the Employee Benefit Booklet for full plan details. Ifdifferences exist between this summary and the Employee Benefit Booklet, the Employee Benefit Booklet will govern.
Exclusive Panel OptionA Feature of Delta Dental PPOSMHOW DOES AN EPO PLAN WORK?EPO Plan PPO Provider NetworkIf you choose the EPO dental plan, you must see a PPO provider in order to receive benefits.* If you receivetreatment from a non-PPO provider, you will be responsible for all fees charged. Of course, with more than2,200 PPO providers practicing across the state, you have many choices.This EPO plan is only for dentists in Colorado.*When looking for a provider using our Find a Dentist online tool, limit your search to PPO providers.PPO dentists submit claim forms directly to Delta Dental of Colorado.Your EPO plan payments are based on a copayment schedule. Dentists submit codes to identify the servicesperformed, and those codes determine which copayment applies. You are responsible for your copayment atthe time of service. A list of codes along with the corresponding copayments can be found in the benefitbooklets posted on your employer’s website or that you received in the mail.Remember, it makes sense to find out how much your copayment for expensive procedures will be, so askyour dentist to submit a pre-treatment estimate. Delta Dental will review your dentist’s treatment plan andtell you exactly how much you are responsible for. This way, you will have a clear understanding of your costbefore you decide to proceed with the treatment.Please note that if you are in the middle of orthodontic treatment and your provider is not in the DeltaDental PPO network, your treatment will not be covered under the EPO plan.**LOOKING FOR A PPO PROVIDER?Visit our website at deltadentalco.com and use our Find a Dentist search tool.Download our free mobile app for iPhone or Android and tap on Find a Dentist.Contact customer service via email at customer service@ddpco.com or toll-free at 1-800-610-0201.*Some plans may have options to allow members to see out-of-state providers. See your benefit booklet.deltadentalco.com
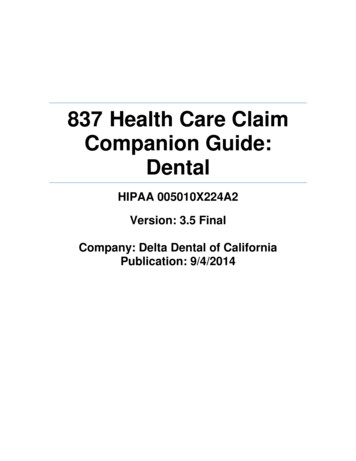
Delta Dental of ColoradoExclusive Panel Option (EPO)2019 Schedule EPO 1BList of Patient Copayments*See Special Provisions on Last PageProcCodePatientCo-PayProcedure Code DefinitionDIAGNOSTIC CODESD0120Periodic oral evaluationD0140Limited oral evaluation - problem focusedD0145Oral evaluation for a patient under three years of age and counseling with primary caregiverD0150Comprehensive oral evaluation - new or established patientD0160Detailed and extensive oral evaluation-problem focused, by reportD0180Comprehensive periodontal evaluation - new or established patientD0210Intraoral-complete series (including bitewings)D0220Intraoral-periapical-first filmD0230Intraoral-periapical-each additional filmD0240Intraoral-occlusal filmD0270Bitewing-single filmD0272Bitewings-two filmsD0273Bitewings-three filmsD0274Bitewings-four filmsD0277Vertical bitewings-7 to 8 filmsD0330Panoramic filmD0460Pulp vitality testsPREVENTIVE 1206Topical Fluoride Varnish - therapeutic application for moderate to high caries risk patientsD1208Topical application of Fuoride - excluding varnishD1351Sealant-per toothD1352Preventive Resin restoration in moderate to high caries risk patient - permanent toothD1353Sealant Repair - Per toothD1510Space maintainer-fixed-unilateralD1516Space maintainer-fixed-bilateral, maxillaryD1517Space maintainer-fixed-bilateral, mandibularD1520Space maintainer-removable-unilateralD1526Space maintainer - removable, bilateral, maxillaryD1527Space maintainer - removable, bilateral, mandibularBASIC SERVICES (Restorative Codes)D2140Amalgam-one surface, primary or permanentD2150Amalgam-two surfaces, primary or permanentD2160Amalgam-three surfaces, primary or permanentD2161Amalgam-four or more surfaces, primary or permanentD2330Resin-based composite-one surface, anteriorD2331Resin-based composite-two surfaces, anteriorD2332Resin-based composite-three surfaces, anteriorD2335Resin-based composite-four or more surfaces or involving incisal angle (anterior)D2391Resin-based composite-one surface, posteriorD2392Resin-based composite-two surfaces, posteriorD2393Resin-based composite-three surfaces, posteriorD2394Resin-based composite-four or more surfaces, posteriorD2520Inlay-metallic-two surfacesD2530Inlay-metallic-three or more surfacesD2543Onlay-metallic-three surfacesD2544Onlay-metallic-four or more surfacesD2710Crown-resin-based composite (indirect)D2740Crown-porcelain/ceramic substrateD2750Crown-porcelain fused to high noble metalD2751Crown-porcelain fused to predominantly base metalD2752Crown-porcelain fused to noble metalD2780Crown-3/4 cast high noble metalD2781Crown-3/4 cast predominantly base metalD2782Crown-3/4 cast noble metal11/1/2018EPO 1B 10.00 10.00 10.00 10.00 10.00 10.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 21.00 28.00 33.00 40.00 24.00 32.00 38.00 46.00 29.00 44.00 62.00 73.00 193.00 223.00 233.00 237.00 161.00 295.00 284.00 245.00 275.00 273.00 238.00 268.001
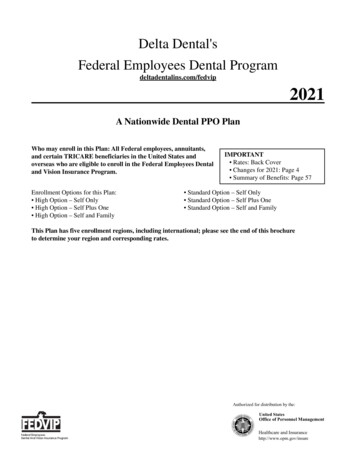
Delta Dental of ColoradoExclusive Panel Option (EPO)2019 Schedule EPO 1BList of Patient Copayments*See Special Provisions on Last full cast high noble metalCrown-full cast predominantly base metalCrown-full cast noble metalRecement inlay, onlay or partial coverage restorationRecement crownPrefabricated stainless steel crown-primary toothPrefabricated stainless steel crown-permanent toothPrefabricated resin crownPrefabricated stainless steel crown with resin windowSedative fillingCore buildup, including any pinsPin retention-per tooth, in addition to restorationCast post and core in addition to crownEach additional cast post - same toothPrefabricated post and core in addition to crownEach additional prefabricated post - same toothLabial veneer (resin laminate)-laboratoryLabial veneer (porcelain laminate)-laboratory 287.00 244.00 280.00 13.00 15.00 45.00 49.00 48.00 61.00 16.00 43.00 10.00 59.00 0.00 51.00 0.00 139.00 147.00BASIC SERVICES (Endodontic Codes)D3110Pulp cap-direct (excluding final restoration)D3220Therapeutic pulpotomy (excluding final restoration)D3310Anterior (excluding final restoration)D3320Bicuspid (excluding final restoration)D3330Molar (excluding final restoration)D3346Retreatment of previous root canal therapy-anteriorD3347Retreatment of previous root canal therapy-bicuspidD3348Retreatment of previous root canal therapy-molarD3410Apicoectomy/periradicular surgery-anteriorD3421Apicoectomy/periradicular surgery-bicuspid (first root)D3425Apicoectomy/periradicular surgery-molar (first root)D3426Apicoectomy/periradicular surgery (each additional root)D3430Retrograde filling-per rootD3450Root amputation - per root 10.00 26.00 110.00 129.00 172.00 191.00 225.00 297.00 114.00 126.00 150.00 41.00 34.00 80.00BASIC SERVICES (Periodontic Codes)D4210Gingivectomy or gingivoplasty-four or more contiguous teeth or bounded teeth spaces per quadrantD4211Gingivectomy or gingivoplasty-one to three contiguous teeth or bounded teeth spaces per quadrantD4212Gingivectomy or gingivoplasty to allow access for restorative procedure, per toothD4240Gingival flap procedure, including root planing-four or more contiguous teeth or bounded teeth spaces per quadrantD4241Gingival flap procedure, including root planing-one to three contiguous teeth or bounded teeth spaces per quadrantD4260Osseous surgery (including flap entry and closure)-four or more contiguous teeth or bounded teeth spaces per quadrantD4261Osseous surgery (including flap entry and closure)-one to three contiguous teeth or bounded teeth spaces per quadrantD4263Bone replacement graft-first site in quadrantD4264Bone replacement graft-each additional site in quadrantD4277Free soft tissue graft (including recipient and donor site) first tooth, implant or edentulous tooth positonD4278Free soft tissue graft (including recipient and donor site) each additional contiguous tooth, implant or edentulous tooth positionD4341Periodontal scaling and root planing-four or more teeth per quadrantD4342Periodontal scaling and root planing-one to three teeth, per quadrantD4910Periodontal maintenance 70.00 26.00 26.00 112.00 67.00 284.00 170.00 71.00 47.00 124.00 62.00 39.00 23.00 24.00MAJOR SERVICES (Prosthodontic Codes - Removable)D5110Complete denture, maxillaryD5120Complete denture, mandibularD5130Immediate denture, maxillaryD5140Immediate denture, mandibularD5211Maxillary partial denture-resin base (including retentive/clasping materials, rests and teeth)D5212Mandibular partial denture-resin base (including retentive/clasping materials, rests and teeth)D5213Maxillary partial denture-cast metal framework with resin denture bases (including any conventional clasps, rests and teeth)D5214Mandibular partial denture-cast metal framework with resin denture bases (including any conventional clasps, rests and teeth)D5221Immediate maxillary partial denture – resin baseD5222Immediate mandibular partial denture – resin base 349.00 349.00 377.00 377.00 243.00 243.00 364.00 364.00 238.00 238.0011/1/2018EPO 1B2
Delta Dental of ColoradoExclusive Panel Option (EPO)2019 Schedule EPO 1BList of Patient Copayments*See Special Provisions on Last 5850D5851Immediate maxillary partial denture – cast metal framework with resin denture basesImmediate mandibular partial denture – cast metal framework with resin denture basesAdjust complete denture, maxillaryAdjust complete denture, mandibularAdjust partial denture, maxillaryAdjust partial denture, mandibularRepair broken complete denture base, mandibularRepair broken complete denutre base, maxillaryReplace missing or broken teeth-complete denture (each tooth)Repair resin partial denutre base, mandibularRepair resin partial denutre base, maxillaryRepair cast partial framework, mandibularRepair cast partial framework, maxillaryRepair or replace broken retentive clasping materials per toothReplace broken teeth-per toothAdd tooth to existing partial dentureAdd clasp to existing partial dentureRebase complete maxillary dentureRebase complete mandibular dentureRebase maxillary partial dentureRebase mandibular partial dentureReline complete maxillary denture (chairside)Reline complete mandibular denture (chairside)Reline maxillary partial denture (chairside)Reline mandibular partial denture (chairside)Reline complete maxillary denture (laboratory)Reline complete mandibular denture (laboratory)Reline maxillary partial denture (laboratory)Reline mandibular partial denture (laboratory)Tissue conditioning, maxillaryTissue conditioning, mandibular 331.00 331.00 17.00 17.00 16.00 16.00 40.00 40.00 34.00 36.00 36.00 47.00 47.00 48.00 33.00 39.00 49.00 141.00 141.00 108.00 108.00 56.00 56.00 51.00 51.00 100.00 100.00 93.00 93.00 26.00 26.00MAJOR SERVICES (Prosthodontic Codes - Fixed)D6210Pontic-cast high noble metalD6211Pontic-cast predominantly base metalD6212Pontic-cast noble metalD6240Pontic-porcelain fused to high noble metalD6241Pontic-porcelain fused to predominantly base metalD6242Pontic-porcelain fused to noble metalD6545Retainer-cast metal for resin bonded fixed prosthesisD6750Crown-porcelain fused to high noble metalD6751Crown-porcelain fused to predominantly base metalD6752Crown-porcelain fused to noble metalD6780Crown-3/4 cast high noble metalD6790Crown-full cast high noble metalD6791Crown-full cast predominantly base metalD6792Crown-full cast noble metalD6930Recement fixed partial denture 274.00 250.00 255.00 276.00 241.00 268.00 100.00 280.00 251.00 268.00 272.00 283.00 256.00 266.00 33.00BASIC SURGERY (Oral Surgery Codes)D7140Extraction, erupted tooth or exposed root (elevation and/or forceps removal)D7210Surgical removal of erupted tooth requiring elevation of mucoperiosteal flap and removal of bone and/or section of toothD7220Removal of impacted tooth-soft tissueD7230Removal of impacted tooth-partially bonyD7240Removal of impacted tooth-completely bonyD7241Removal of impacted tooth-completely bony, with unusual surgical complicationsD7250Surgical removal of residual tooth roots (cutting procedure)D7251Coronectomy - intentional partial tooth removalD7285Biopsy of oral tissue-hard (bone, tooth)D7286Biopsy of oral tissue-soft (all others)D7310Alveoloplasty in conjunction with extractions-per quadrantD7320Alveoloplasty not in conjunction with extractions-per quadrant 22.00 43.00 48.00 60.00 70.00 100.00 42.00 85.00 58.00 36.00 34.00 49.0011/1/2018EPO 1B3
Delta Dental of ColoradoExclusive Panel Option (EPO)2019 Schedule EPO 1BList of Patient Copayments*See Special Provisions on Last PageD7471D7472D7473D7510D7960Removal of lateral exostosis (maxilla or mandible)Removal of torus palatinusRemoval of torus mandibularisIncision and drainage of abscess-intraoral soft tissueFrenulectomy (frenectomy or frenotomy)-separate procedure 68.00 68.00 68.00 25.00 51.00ORTHODONTIC CODESD8010Limited orthodontic treatment of the primary dentitionD8020Limited orthodontic treatment of the transitional dentitionD8030Limited orthodontic treatment of the adolescent dentitionD8040Limited orthodontic treatment of the adult dentitionD8050Interceptive orthodontic treatment of the primary dentitionD8060Interceptive orthodontic treatment of the transitional dentitionD8070Comprehensive orthodontic treatment of the transitional dentitionD8080Comprehensive orthodontic treatment of the adolescent dentitionD8090Comprehensive orthodontic treatment of the adult dentitionD8210Removable appliance therapyD8220Fixed appliance therapyD8660Pre-orthodontic treatment visitD8670Periodic orthodontic treatment visitD8680Orthodontic retention (removal of appliances, construction and placement of retainer(s))MISCELLANEOUS CODESD9110Palliative (emergency) treatment of dental pain-minor proceduresD9120Fixed partial denture sectioningD9222Deep sedation/general anesthesia - first 15 minutesD9223Deep Sedation/general anesthesia - each subsequent 15 minute incrementD9230Analgesia, anxiolysis, inhalation of nitrous oxideD9239Intravenous moderate (conscious) sedation/analgesia - first 15 minutesD9243Intravenous moderate (conscious) sedation/analgesia - each subsequent 15 minutesD9310Consultation (diagnostic service provided by dentist or physician other than practitioner providing treatment) 600.00 750.00 840.00 935.00 730.00 825.00 1,685.00 1,780.00 1,980.00 180.00 238.00 35.00 9,999.00 213.00 18.00 9.00 27.00 27.00 8.00 30.00 30.00 14.00* SPECIAL PROVISIONS:Services MUST be performed by a Delta Dental PPO dentist in order to be payable under this program.Services are subject to the limitations, exclusions and governing policies of the program.The submitted fee for any procedure NOT LISTED is the responsibility of the patient.General or orthodontic plan maximums may apply. Refer to the member's benefit information.11/1/2018EPO 1B4
This EPO plan is only for dentists in Colorado.* When looking for a provider using our Find a Dentist online tool, limit your search to PPO providers. PPO dentists submit claim forms directly to Delta Dental of Colorado. Your EPO plan payments are based on a copayment schedule. Dentists submit codes to identify the services