Transcription
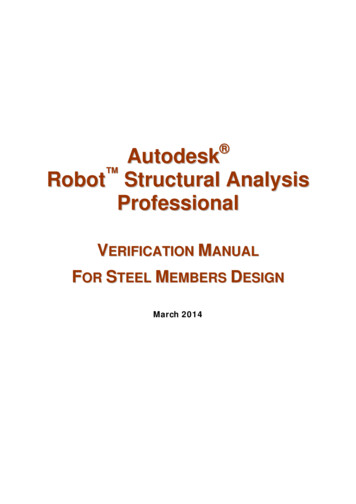
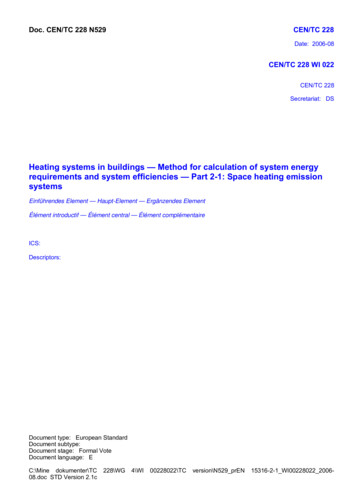
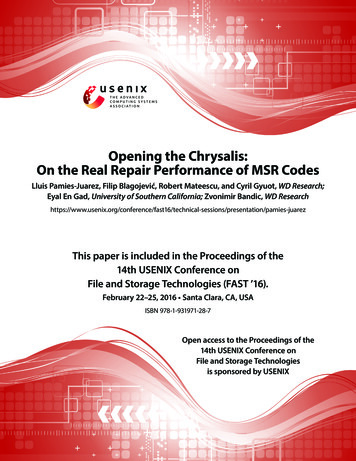
LRCS Instructions (Labor Rate Calculation Sheet)04/24/2017Please submit your Labor Rates and all required back-up to the AEC Cost Estimator,John Minuth, within 14 calendar days after receiving your contract.First, download the latest Labor Rate Calculation Sheet (LRCS), [Rev 04/24/2017], atthe AEC website [AEC Website: Contractor Links]. Also available at this site is the“Contractors’ Quotation Sheet” (CQS), on which any and all quotations for extra workmust be submitted.Second, read the "Instructions" tab carefully and follow them explicitly. Any questionsshould be directed to John Minuth, AEC Cost Estimator, at (734) 763-3317 or[minjohn@umich.edu]Third, the following documents must be included with your Labor Rate Submittal and bee-mailed together, directly to the Cost Estimator:1. One Excel "LRCS" workbook for each of the trades being submitted for approval.Filling-out the Journeyman Sheet will populate many cells on the othertabs of this workbook. Submit an ENTIRE EXCEL WORKBOOK, in “.xlsx” format,for each trade. PDF's OF THE WORKBOOK PAGES WILL BE REJECTED.2. An un-protected PDF copy of the corresponding Union Local wage rate breakdownfor each submitted trade. If "Prevailing Wages" are being submitted, provide PDFcopies of the source document from the State of Michigan Department of Licensingand Regulatory Affairs (LARA). Please indicate the applicable rate groupings bycheck marks and/or circling the correct rates if there are multiple categories on theback-up document. When entering the "CRAFT/TRADE", utilize a completedescription, i.e. "Carpenter - CA687Z2" or “Carpenter – Zone1” or “Ironworker –Structural”.3. An un-protected PDF copy of company's current Workers' Compensation PolicyInformation form, which includes the "Workers' Comp Class Codes" and theiraffiliated "Rates of Remuneration per 100" and a listing of all applicable discountsand additional costs related to the submitted trades. Two of the strategic valuesrequired for the SUTA calculation are the Manual (undiscounted) Premium and theTotal Estimated (net) Annual Premium.4. An un-protected PDF copy of the Michigan “Employer’s Quarterly TaxReport” (forms UIA 1028 or UIA MiWAM) for each quarter of the previousyear (2016).5. A summary of the total hours for the previous year (2016) including hourly andsalaried workers. This document can be in the form of a payroll report or aMIOSHA Form 300a.Once your Labor Rates have been approved, enter the approved Labor Rates in theContractors’ Quotation Sheet on the tab entitled “1 Approved Labor Rate Summary”.Once this is done, the CQS document can be saved as a “MASTER” copy until theexpiration date of those Labor Rates.
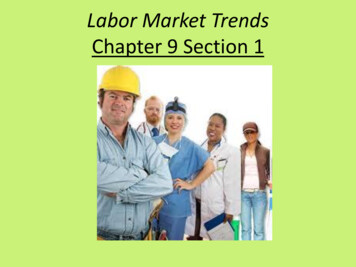
Authorized ByMCL 421.1 et seq.State Of MichiganDepartment of Licensing and Regulatory AffairsUnemployment Insurance Agency3024 W Grand Blvd, Detroit, MI 48202www.michigan.gov/uiaUIA 1028(Rev. 10-14)Rick SnyderGOVERNORSharon MoffettMasseyDIRECTORMail To:MI Tax Form Example 1Unemployment Insurance Agency PO Box33598Detroit, MI 48232-5598Employer’s Quarterly Wage/Tax ReportYOU MUST FILE THIS REPORT EVEN IF YOU ARE UNABLE TO PAY OR HAVE NO PAYROLL FOR THE QUARTER.For details about completing this report, see the instructions page.Employer Type: Contributingo(Complete Sections 1, 2, 3 & 4)Reimbursingo(Complete Sections 1, 2 &4)SECTION 1oCheck this box if this is an Amended report. Explain:UIA Employer Account No:Provide the number of all full-time employees plus partFEIN:Quarter Ending Date (mm/dd/yyyy)-time employees who worked during or received pay for The paythperiod that includes the 12 of the month:03/31/20151st Month2nd Month3rd Month16146SECTION 2List only employees who had wages during this quarter.FamilyOwnedEnter“F”Delete“X”Social SecurityNumber362-11-1955Employee Last NameEmployee First NameCLEARYDo364-15-2750Not Show Personal/PrivateInformation.MollGross WagesPaid -7803ST OLLChristopher9,579.01JASON2,308.75364-84-9003If more lines are needed to enter employee information, continue to Section 1 on back of form. When finished entering employees,continue to Section 3 for Contributing Employers or Section 4 for Reimbursing Employers.For UIA Use Only. Do Not Write Below Line.REV 04/16/
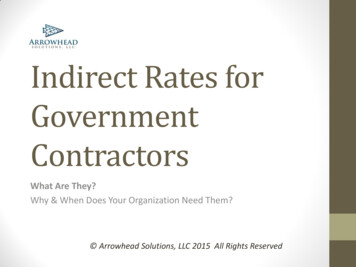
UIA 1028(Rev. 10-14)SECTION 2 ial SecurityNumberEAN:Employee Last NameEmployee First NameGross WagesPaid SH7,025.75Beginning in the first quarter 2015, all employers must use MiWAM to file online; this includes employers who are reporting out-of-state wagesand/or entering J-1 or H-2B wages.SECTION 3Total Gross Wages paid this quarter:Excess Wages:Taxable Wages:UI Tax Rate (ABC CBC NBC):UI Tax Due (UI Tax Rate x Taxable Wages) Round to Nearest :Obligation Assessment (OA) Rate: OADue (OA Rate x Taxable Wages) Do Not Round: TotalAmount Due (UI Tax Due OA Due):Prior Balance:Amount Enclosed:Taxable Wage Limit:DUE DATE:144,787.7228,708.37116,079.35x 0.10300%11,956.00x 15oCheck this box if this is the Final Report for this business. (Prepare and submit Form UIA 1772)o I meet the requirements to apportion my payments and elect this option.(See instructions for more information)SECTION 4YOUR CERTIFICATION: I certify that I have examined this report, and that to the best of my knowledge and belief, it is correct andcomplete.SignatureTitleDateContact Phone NumberREV 04/16/15 OSPQuestions: If you have any questions, please contact the Office of Employer Ombudsman (OEO) at 1-855-484-2636) or by email at OEO@michigan.govMAKE A COPY OF THIS REPORT FOR YOUR RECORDSPage 2of2
Hours Summary Example 1Great Lakes Mechanical Co20122012
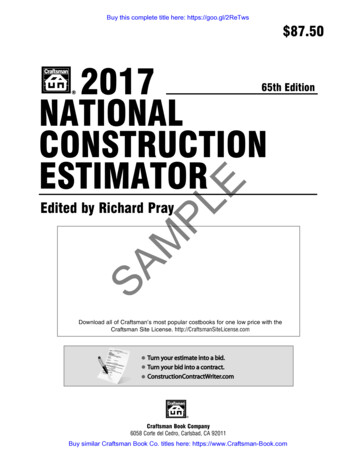
Hours Summary Example 2202015YearSUMMARY OF WORK-RELATED INJURIES AND ILLNESSESAll establishments covered by Public Law of 1970 (P.O. 91-596) and Michigan Occupational Safety and Health Act 154, P.A. 1974, Patt 11,Michigan Administrative Rule for Recording and Reporting of Injuries and Illnesses, must complete this Summary page, even if no injuries orillnesses occurred during the year. Remember to review the Log ta verify that the entries are complete and accurate before completing thissummary. Yau may be fined for failure ta comply.Using the Log, count the individual entries you made far each category. Then write the totals be/aw, making sure you've added the entries fromevery page of the log. If you had no cases write "O."Employees former employees, and their representatives have the right to review the MIOSHA Farm 300 in its entirety. They also have limitedaccess to the MJOSHA Form 301 or its equivalent. See Part 11, R408.22135 Rule 1135, in MIOSHA's Recordkeeping rule, for further details onthe access provisions for these forms. .' ",.,:" · ·".·Total number ofdeathsEstablishment informationYour establishment nameTotal number ofcases with daysaway from workTotal number of caseswith job transfer orrestrictionTotal number ofother recordablecases0004(G)(H)(I)(J)Goyette Mechanical Co Inc.Street 3842 GoreCityNumber of Cases.-'F- li nt---------StateMlZipIndustry description (e.g., Manufacture of motor truck trailers)Construction-Mechanical ContractorStandard Industrial Classification (SIC), if known (e.g., SIC 3715)OR North American Industrial Classification (NAICS), if known (e.g., 336212)Employment infonnationTotal number ofdays away fromTotal number of days ofjob transfer or restrictionAnnual average number of employees172\Alt"\rlr00(K)(l)Total hours worked by all employees lastyear320384Sign hereTotal number of.(M)(1) Injury(2) Skin Disorder(3) RespiratoryConditionsKnowingly falsifying this document may result ina fine.400(4) Poisonings(5) Hearing Loss(6) All Other Illnesses00Icertify that I have examined this document and that to the best of my knowledge the entries are true, accurate, andcomplete.0VPOperationsMatt BurkeCompany ExecutiveTitlePhoneDate810-743-6883Post this Summary page from February 1to April 30 of the year following the year covered by the fonnPublic reporting burden for this collection of information is estimated to average SO minutes per response, including lime to review the instruction, search and gather the dataneeded, and complete and review the collection of information. Persons are not required lo respond lo the collection of information unless it displays a currently valid OMB controlnumber. If you have any comments about these estimates or any aspects of this data col!ection, contact Michigan Department of Energy, Labor & Economic Growth, MIOSHA,MTSD, 7150 Harris Dr. P.O. Box 30643, Lansing Ml 48909-8143. (517) 322-1848. Do not send the completed forms to this office.MIOSHA-300A Rev. 09/09 EffecUve 01/011200412Michigan Department of Energy, Labor & Economic GrowthMichigan Occupational Safety and Health Administration (MIOSHA)21112013
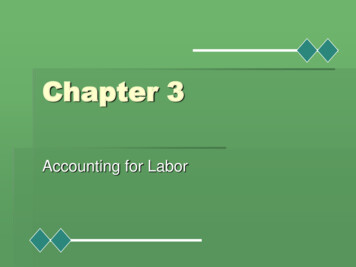
1489ACUITYWORKERS' COMPENSATIONA Mutual Insurance CompanyWorkers' Comp. Example 1Information Page1 . Named Insured and Address:Agency Name and Number :VALENTI TROBEC CHANDLER INC6648-AJSTE 200TROY Ml 48098Insured Policy Number: X63634Policy Number: CWC-X63634-00R L SHEKELL INC34904 FOREST STWAYNE Ml 48184Identification Number:FEIN: 38277428 1Ml Risk ID: 3746798AThe Named Insured is:CORPORATION2. Policy Period:3. A.Inception03-01-16Expiration 03-01-1712:01 A.M. standard time at the address of the insured stated herein.Workers ' Compensation Insurance: Part One of the policy applies to the Workers ' CompensationLaw of the states listed here:Michigan8.Employers' Liability Insurance: Part Two of the policy applies to work in each state listed in Item3.A. The limits of our liability under Part Two are:Bodily Injury by AccidentBodily Injury by DiseaseBodily Injury by DiseaseC.Each Accident. . . . . . . . . . . . . . . . . . . . . . . Policy Limit . . . . . . . . . . . . . . . . . . . . . . . . .Each Employee . . . . . . . . . . . . . . . . . . . . . .1,000,0001,000,0001,000,000Other States Insurance: Part Three of the policy applies to the states , if any, listed here:All states except North Dakota, Ohio, Washington and Wyoming and States designated in Item3.A. above.D.Endorsements:Form NumberForm TitlePremiumWC 00 04 06 (08-84)WC 00 03 13 (04-84)Premium Discount Endorsement . . . . . . . . . . . . . . . . . . . . Waiver of Our Right to Recover From Others Endorsement .WC 00 00 00 B(07- 11) Workers ' Compensation and Employers' Liability InsurancePolicy . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .Experience Rating Modification Factor Endorsement . . . . . .WC 00 04 03 (04-84)Pending Rate Change Endorsement . . . . . . . . . . . . . . . . .WC 00 04 04 (04-84)WC 00 04 14 (07-90) Notification of Change in Ownership Endorsement . . . . . . .WC 21 03 03 (06-01) Michigan Notice to Policyholder Endorsement . . . . . . . . . . .WC 21 03 04 (04-84)Michigan Law Endorsement . . . . . . . . . . . . . . . . . . . . . . .Insured Renewal or Replacement Number: X63634Renewal or Replacement Number: CWC-X63634-00WC 00 00 01 A(6-01 )Policyholder - Originalso01 02/20/ 15
1490Page 2X63634Insured Policy Number:Policy Number: CWC-X63634-00Effective Date:03-01-16Form NumberForm TitlePremiumIL-7084 (01-09)Michigan Filing Exemption . . . . . . . . . . . . . . . . . . . . . . . . .WC 00 04 22 A(09-08 ) Terrorism Risk Insurance Program Reauthorization ActDisclosure Endorsement . . . . . . . . . . . . . . . . . . . . . . . . . .WC 00 04 21 C(09-08) Catastrophe (Other than Certified Acts of Terrorism ) PremiumEndorsement . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .4. Premium: The premium for this policy will be determined by our Manual of Rules, Classifications, Ratesand Rating Plans. All information required below is subject to verification and change by audit.Classificationof OperationsPremium BasisRates(Estimated TotalAnnualRemuneration)(Per 100 o.Concrete Work - Floors, Drivewaysand Drivers0015221300,000Concrete Construction NOC0025213If Any10.33IncludedDrivers NOC003738050,0004.552,275 .00Clerical Office Employees NOC004881080,000.140059812MichiganEmployers' Liability With Work Comp Iner. Limits 1,000,000 Bl per Accident 1,000,000 Disease per Employee,1,000,000 Aggregate Disease Limit 7.0421 ,120.00112.00470 .00Manual Premium23 ,977.00Experience Modification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .x.83019,901 .00Less Schedule Amount . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2,985.00Less Premium Credit Amount . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2 ,537.00Additional Premium Waiver OfSubrogation--Not Subject ToExperience Rating008911511550.001650.00Less Premium Discount . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .896 .00Expense Constant . . . . . . . . . . . . . . . . . . . . . . . . . . 0900 . . . . . . . . . . . . . . . . . . . . . . . . . . . . .180.00Provisions for Terrorism0069740430,000.03129.00Provisions for Catastrophe (Otherthan Certified Acts of Terrorism)0079741430 ,000.0143 .00WC 00 00 01 A(6-01)so 0102/20/ 16-.--·
Page 3Insured Policy Number: X63634Policy Number: CWC-X63634-00Effective Date:03-01-1515ContractsTotal Estimated Annual Premium . . . . . 13,885.00Annual Minimum Premium . . . . . 700.0016Per ContractNamed InsuredR L SHEKELL INCFederal Employer Identification Number: 382774281State Unemployment Number:Locations Covered:34904 FOREST STWAYNE Ml 481845353 COGSWELL RDWAYNE Ml 48184Countersigned by VALENTI TROBEC CHANDLER INCAuthorized RepresentativeDate of Issue: 02-20-16'----WC 00 00 01 A(6-01)so 0102/20/ 16
t n LH Lll J f\. J 1 JJ Vll'.11 11 I LUll'J.r 1\.J I.THECINCINNATIINSllKANCE COMrANl SWORKERS COMPENSAT ION AND EMPLOYERS LIABILITY INSURANCE POLICYEXTENS ION OF INFORMATION PAGEWorkers' Comp. Example 2,'POLICY NUHBER. 11'I.POLICY,i' PERIOD .iJ·FROMweJ. 1t JU. RENEWAL"1-; CARRIERRISK . ID NO .· "AGENCY:,TO1862156-0105/01/15 05/0l/16 WC 1862156-00 271972040034A'. ,.,,,AGENT:;1.·.,.,,.·,·:,!1i.·;- .-1 ·.,. .1 : ·. NAMED INSURED AND ADDRESS,'ITEM ERIE WELDING AND MECHANICALBROOKS INSURANCE AGENCYCONTRACTORS INCl.1120 MADISON AVE9776 s DIXIE HIGHWAY BOX 254TOLEDOOH 43604ERIE MI 48133FEIN 383166475.t'11'34-120r ;· , ',;INC OLICY AGE3TEM 4.LOC CODENOu 001 5183881087423365CLASSIFICATIONS;r·" PLUMBING NOCCLERICAL OFFICE EMPLOYEESSALESPERSONS-OUT SIDEWELDING NOCPREMIUM BASISRATE PER ESTIMATEDTOTAL ESTIMATED 100 OFANNUALANNUAL REMUNERATION REMUNERATION PREMIUM148,4604.67 6,93317,800.366490,000.665947.030IF ANYSUB-TOTALPREM FOR INCREASED PART TWO LIMITS, EFF 05/01/14EXPERIENCE MOD, EFF 05/01/14, USING FACTORMI SCHEDULE MODIFICATION7,591.0100.89001.2500TOTAL FOR MICHIGAN0900EXPENSE CONSTANT9740TERRORISM RISK INSURANCE ACT OF 2002TOTAL ESTIMATED ANNUAL PREMIUMwe 000001A (08109)00SCHEDULEPAGE1:T980798989889 · P · .,,.ISSUE DATE 04/14/15768431,7068,530200.02051 8,781INSURED COPYIncludes copyright material or t he Nalional Council on Compensal ion Insurance, used with its permission. Copyrighl 1987 National Councll on Compensal ion Insurance.
An un-protected PDF copy of company's current Workers' Compensation Policy Information form, which includes the "Workers' Comp Class Codes" and their . Two of the strategic values required for the SUTA calculation are the Manual (undiscounted) Premium and the Total Estimated (net) Annual Premium. . Workers' Comp.Example1. WC 00 01 A(6-01 .