Transcription
HEALTH INDICATORS FOR WOMENIN LOS ANGELES COUNTYHighlighting Disparities by Ethnicity and Poverty LevelA Publication of the Los Angeles County Department of Public HealthOffice of Women’s Health and Office of Health Assessment & EpidemiologyJanuary 2017
2ACKNOWLEDGMENTSLos Angeles County Department of Public HealthOffice of Women’s HealthCompiled and Written by:Rita Singhal, MD, MPH, Medical DirectorRaúl Sobero, DrPH, MPHFred Dominguez, MPHAnnie Pham, MPHcEllen Eidem, MS, DirectorSummer NaganoLeora SteinbergEthel JohnsonOffice of Health Assessment & Epidemiology,Health Assessment UnitAmy S. Lightstone, MPH, MA, Interim ChiefYan Cui, MD, PhDYajun Du, MSJerome Blake, MPH, CPHMing H. Lee, MPH, MSAOM, L.Ac.Pei-Lin Chen, MPHOther Programs Contributing Data and ExpertiseLos Angeles County Department of Public HealthDivision of HIV and STD ProgramsInjury & Violence Prevention ProgramMaternal, Child & Adolescent Health ProgramsOffice of Health Assessment & Epidemiology,Epidemiology UnitTuberculosis Control ProgramLos Angeles County Cancer Surveillance Program, USCUCLA Center for Health Policy ResearchU.S. Census BureauHEALTH INDICATORS FOR WOMENIN LOS ANGELES COUNTYHighlighting Disparities by Ethnicity and Poverty LevelTable of ContentsForeword3Introduction3User Guide3Findings and Implications4Demographics6Determinants of Health8Health Status10Health Care Access12Health Behaviors14Health Conditions – Incidence/Prevalence16Health Conditions – Mortality18Special Health TopicsEconomic Security and Well-Being20Report Design and Layout byTrauma and Stress Among Mothers22Kathleen Pittman, Pittman CreativeSummer Nagano, Office of Women’s HealthAmerican Indian/Alaskan Native24Educational Level and Health25Homeless Women26Special Thanks toOffice of Women’s Health Policy CouncilWomen’s Health Data CommitteeData Sources and Notes27
FOREWORDWe are pleased to present our latest women’s healthdata report titled, “Health Indicators for Women inLos Angeles County: Highlighting Disparities by Ethnicityand Poverty Level, 2017.” This report offers a current andcomprehensive snapshot of women’s health in LosAngeles County using a variety of health indicators.Women compose slightly more than half of thepopulation in the county, and comparing these indicatorsby race/ethnicity and poverty level provides a powerfulfilter that reveals challenges and opportunities for healthimprovement.The health and well-being of women in Los AngelesCounty is influenced by a unique set of factors thatinclude biological differences as well as social, economic,and environmental circumstances. For instance,compared to men, women report lower income,increased caregiving responsibilities, and poorer selfreported health status. Understanding and addressingthe causes of these gender differences in health is criticalin promoting gender health equity.Further, the rich racial and ethnic diversity amongwomen in Los Angeles County highlights the need tobetter understand and address differences in healthstatus and determinants of health among these diversegroups of women. Certain communities have higherexposure to violence, discrimination, and institutionalracism, which result in an unequal burden of poorerhealth and more vulnerable populations.Promoting community health is an essential serviceof public health. While this report provides a variety ofhealth data, solving community health issues is a goalthat can only be achieved through collaboration with awide range of community stakeholders. We hope thatthis latest data report will raise awareness of issues anddisparities in women’s health and also provide guidanceand support to help solve these issues and enhance healthequity through the development and implementationof policies, programs, and services to improve the healthand well-being of women, their families and theircommunities throughout Los Angeles County.Cynthia A. Harding, MPHINTERIM DIRECTOREllen Eidem, MSIntroductionThis report describes the current status of women’s health and wellbeing in Los Angeles County using standard indicators that measuresocial and economic health determinants, health status, health careaccess, health behaviors, incidence and prevalence of selected healthconditions, and cause-specific mortality rates. Data are stratified byrace/ethnicity and by Federal Poverty Level (FPL) to better understanddisparities that exist. Where available and appropriate, Los AngelesCounty health indicators are compared to Healthy People 2020 targets,which are the benchmarks that our nation is striving to achieve.This 4th edition of the report includes some important changes andnew topics/indicators. One significant change is that the Asian/Pacific Islander race/ethnicity categorypreviously used throughout the report has been replaced with an Asian alone category due to changes in howdata is categorized and reported, and due to input from the Native Hawaiian and Other Pacific Islander communityadvocating to be removed from the Asian grouping. Examples of new topic areas include discrimination,emotional well-being, and access to health coverage. In addition, new indicators are included on access tofamily planning, use of e-cigarettes, depression, skin cancer, and chronic liver disease.Finally, in the Special Health Topics section, the health of American Indian/Alaskan Native and Homelesswomen is highlighted. Other special health topics focus on important determinants of health in the EconomicSecurity and Well-Being, Trauma and Stress Among Mothers, and Educational Level and Health pages.User GuideData for each race/ethnic group and FPL category are represented, asin the previous edition, by colored columns used uniformly throughoutthe main sections of this report. The columns in shades of purple givethe Healthy People 2020 targets, followed by data for all LA Countymen and women combined, and then LA County women alone. Datapresented are for adults 18 years and older, unless otherwise noted inthe Data Sources and Notes.Where statistical significance testing was possible and appropriate,each group was compared to the other three groups combined in thatcategory. Groups that fare statistically better are designated with a greenunderline; groups faring statistically worse are designated with a red underline. When statistical comparisonswere not conducted, the indicator row is marked with a “ ”. No statistical comparisons were performed forDemographics, Health Conditions – Mortality, and the Special Health Topics, except in the Trauma and StressAmong Mothers section.Please note, this edition of the report includes data from several new data sources using variousmethodologies. It is important to review the Data Sources and Notes to understand the data source and yeardata was collected for each indicator. Not all data will be comparable across the report. Some indicators in theSpecial Health Topics sections are the same or similar to indicators in the main section of the report, but due todifferences in the data sources, the data will not always be consistent. For example, insurance status data in theAmerican Indian/Alaskan Native special topics section comes from a different data source than the insurancestatus data in the Health Care Access section of the main report. Similarly, data in this report may not becomparable to data in previous editions of the report due to data source changes and methodology changes.For additional methodology questions, please see the website for the data source in question.DIRECTOR, OFFICE OF WOMEN’S HEALTHHEALTH INDICATORS FOR WOMEN IN LOS ANGELES COUNTY – 20173
4FINDINGS AND IMPLICATIONSIn this edition of the “Health Indicators for Women in Los Angeles County” report, there is evidence of the significant gains madein the health of women over the past 3 years. The rate of women without health insurance has been cut by more than half, thepercent of women unemployed and looking for work has decreased, less women report smoking cigarettes and mortality fromleading causes of death such as coronary heart disease continues to decline. However, over half of women continue to live in poverty,and homelessness has increased dramatically. In addition, deep-rooted determinants of health such as discrimination, trauma and stressserve as significant factors underlying the ongoing health inequities identified for women in Los Angeles County.Racial/Ethnic DisparitiesLos Angeles continues to be an increasingly diversecounty, with women of color now representing almost70% of women in the county. Latinas, representingthe largest proportion of women, experienceimportant socioeconomic challenges that put themat risk for health disparities. Latinas are more likelyto have less than a high school education, the lowestrates of obtaining four-year college degrees, and thelowest median annual earnings compared to womenof other race/ethnic groups. These conditions impactthe health of Latinas as noted by their high rates ofobesity, diabetes-related mortality, and self-reportedfair or poor health status. Without adequateintervention, aging Latinas may experience higherdisease rates and poorer health outcomes.Black women in LA County face unique factors thatadversely affect their health. They are more likely tobe single with children in the household, and amonghouseholds headed by single women with children,black women have the highest poverty rates. Theystruggle with the highest unemployment rates and aremuch more likely to be homeless than women fromother race/ethnic groups. In addition, black women aremore likely to experience discrimination and violence.These serve as significant barriers to attainingoptimal health despite black women having high ratesof health insurance. Poor health outcomes areapparent by the high rates of smoking, obesity,diabetes, heart disease, cancer, and maternal andinfant mortality. Addressing entrenched factors suchas discrimination, institutional racism, violence, andtrauma are needed to make significant gains in blackwomen’s health.Asian women have the longest life expectancyamong all race/ethnic groups and this number hassteadily increased over the last decade. Althoughthey may not encounter the same socioeconomicchallenges of other groups, Asian women are morelikely to speak English less than “very well” and havesignificant gaps in access to care, reporting difficultiesin accessing care and experiencing low rates ofreceiving clinical preventive services. Most important,to understand the true health disparities apparentamong Asian women, data for this heterogeneousgroup needs to be disaggregated and strengthened.For the first time, in this edition of the report, thehealth of American Indian/Alaskan Native (AI/AN)women is examined as a special health topic. Thefindings are significant, with this group reporting thehighest rates of overweight/obesity and high bloodpressure; and higher death rates from coronary heartdisease and diabetes compared to other race/ethnicgroups. They are also more likely to report their healthas being fair or poor, smoke cigarettes, and seriouslythink about committing suicide. The health of AI/ANwomen is challenged by a high rate of poverty, lowlevel of education, and high rate of having experiencedintimate partner violence. These factors, combinedwith decreased access to health care and low healthinsurance enrollment rates, make this group of womenone of the most vulnerable in the county.White women have high rates of high school andcollege graduation, highest median employmentearnings, and lowest poverty rates. Additionally, theyare least likely to report a fair or poor health statusand only 5% report being uninsured. However, almost1 in 4 have ever experienced intimate partner violenceand they have the highest rates of depression, suicidemortality and Alzheimer’s disease mortality. A largerproportion of white women are 65 years or older and,therefore, represent a large proportion of chronicdisease prevalence and mortality.Poverty and EducationPoverty is a key determinant of health. In Los AngelesCounty, low-income women have poorer healthbehaviors, health care access and health outcomes.Women living in poverty are four times more likely toreport a fair or poor health status compared to womenliving at the highest income level. Poverty is linked toother health determinants and a lower percentage oflow-income women report having food security, livingin safe neighborhoods and owning their homes. A closerlook at the economic security and well-being of womenreveals that LA County women tend to have lowermedian employment earnings than California womenand LA County men. The gender wage gap, which
Poverty and Education (continued)compares median earnings between women and menas a ratio, is 0.954 for LA County women but is as lowas 0.381 for Latinas when compared to white men.Level of education serves as an important socialdeterminant of health and has a significant impacton health status and quality of life. Approximatelyone-fourth of LA County women have less than a highschool education, and only 1 in 7 have a collegedegree. Women with lower education report higherrates of fair or poor health compared to women withhigher education levels. Women with less than acollege degree are also much more likely to be obeseand have diabetes than women with a college degree.Programs that promote and assist with literacy, highschool or GED completion, and college attendanceare needed to reduce educational inequity. Improvements in education levels will also expand the typeof employment opportunities that make it possible toreduce the proportion of women living in poverty.Stressors Impacting HealthAs additional research is available, it is apparent thatless-studied factors such as homelessness, trauma anddiscrimination are important determinants of health.These factors are examined in the special health topicpages Homeless Women, and Trauma and StressAmong Mothers. Homelessness among women inLA County has increased dramatically over the lastseveral years, with more than 14,000 homelesswomen reported in 2016. Homeless women are morelikely to report having mental illness, a history ofsubstance abuse and experiencing domestic violence.Lack of affordable housing in Los Angeles County iscontributing to homelessness. A staggering 70% ofHEALTH INDICATORS FOR WOMEN IN LOS ANGELES COUNTY – 2017households headed by single female renters reportspending over 30% of their income on rent, and onlyhalf of women in LA County report owning homes.Pregnancy is a particularly important time inwomen’s lives when optimal health will not onlyimpact the mother’s future health but also that ofher baby throughout its life. Exposure to trauma andstress during this period is significantly more of a factorfor black and Latina mothers than other race/ethnicgroups. Black and Latina mothers are significantly lesslikely to report their neighborhoods being safe fromviolence, being clean, and having good policeprotection. Although black mothers are more likely toreport experiencing a stressful event during pregnancy,Latina mothers report less social support duringpregnancy. Exposure to discrimination during theirlifetime is reported for over half of black motherscompared to 38% of mothers overall.Impact of Affordable Care Act andMedi-Cal ExpansionAs a result of the Affordable Care Act and Medi-Calexpansion, the percentage of uninsured womendecreased by more than 60% from 2011 to 2015.However, the degree of improvement was notconsistent across all race/ethnic groups, anddisparities in insurance status still exist. Latinasexperienced the largest decrease; however, theystill account for the highest percentage of uninsuredwomen. Despite the large overall decrease in thepercent of uninsured women, the proportion of thosewith ‘no regular source of care’ only decreased slightly,indicating that work is still needed to ensure the newlyinsured are using their insurance effectively. Effortsto assist the remaining uninsured women need to beredoubled through targeted outreach and enrollmentstrategies. Most important, united efforts are neededto protect the policies that have been implemented toensure the gains made are not lost.Looking to the FutureThe proportion of LA County women who are 65 yearsor older continues to rise, and the proportion of thosereaching age 85 years has increased. With thecontinued increase in women’s longevity, thisrepresents new challenges for the health care systemas older women tend to experience a higher prevalenceof functional limitations and higher rates of chronicdiseases compared to younger women. Not only willexpansion and improvement of health services forolder women be needed, but also increased availabilityof chronic disease self-management programs, andprevention activities over the lifespan.Equally important as the expansion and improvement of health care and prevention services,addressing important socioeconomic determinants forlow-income women and women of color is also keyfor reducing health disparities. Additional researchis needed on how social determinants such asdiscrimination, violence, housing and education areaffecting health and what policy, systems andenvironmental strategies are needed to address them.The hope is that the data contained in this reporteffectively highlights the social and economic factorsthat affect the health of LA County women and thedisparities that still exist despite substantial improvements in some areas. Ideally, the data in this reportshould help in program planning, resource allocation,and policy making to help improve the health statusof women throughout Los Angeles County.5
Women: Race/EthnicityAge Group Percent of adults who are 18 to 39 years1 Percent of adults who are 40 to 64 years1 Percent of adults who are 65 years or 94.195.9*96.9* 95.291.692.7*95.4* 763.157.342.425.2Foreign Born Percent of adults who were not born in the United States1 300% FPL44.6Disability Percent of adults with a disability1b200-299% FPL41.1Income Percent of adults with household incomes 100% of the Federal Poverty Level1a Percent of adults with household incomes 100 to 199% of the Federal Poverty Level1a Percent of adults with household incomes 200 to 299% of the Federal Poverty Level1a Percent of adults with household incomes 300 to 399% of the Federal Poverty Level1a Percent of adults with household incomes 400% of the Federal Poverty Level1a100-199% FPL42.7Sexual Orientation Percent of adults (18-70 years) who self-identify as straight or heterosexual2 Percent of adults (18-70 years) who self-identify as gay, lesbian, homosexual orbisexual2 Percent of adults (18-70 years) who self-identify as not sexual, celibate, noneor other2Women: Federal Poverty Level (FPL)N/ARace/Ethnicity Percent of adults who are American Indian/Alaskan Native1 Percent of adults who are Asian1 Percent of adults who are black1 Percent of adults who are Latino1 Percent of adults who are Native Hawaiian and Other Pacific Islander (NHOPI)1 Percent of adults who are white1 100% FPLWhiteLatinaBlackAsianLos Angeles County WomenLos Angeles County Men and WomenDEMOGRAPHICSHealthy People 2020 Target6
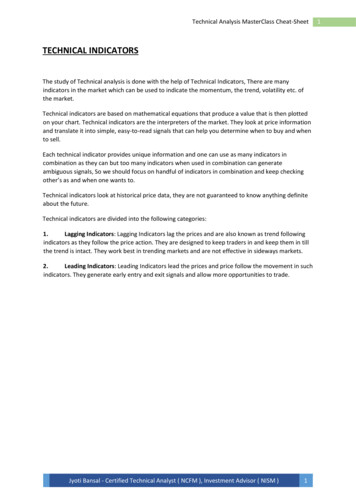
Years in the United States (U.S.) among Foreign Born Percent of foreign-born adults living in the U.S. 5 years1 Percent of foreign-born adults living in the U.S. 5 to 9 years1 Percent of foreign-born adults living in the U.S. 10 years1Language Used Most Often at Home Percent of adults who mostly speak English at home1 Percent of adults who mostly speak Spanish at home1 Percent of adults who mostly speak an Asian language at home1c Percent of adults who mostly speak some other language at home1cRelationship Status Percent of adults who are coupled1d Percent of adults who are single1dHousehold Type Percent of households where adults are single with .7N/A12.817.39.731.324.97.429.120.412.67.1N/A Data not available where noted*Estimate is statistically unstable**Cell size less than 5 - data not reported due to confidentialityWomen in Los Angeles County by Ageand Race/Ethnicity, 20151vxhbfghfgshs18 to 39 years40 to 64 years1009017131865 years or older1030Percent of Women8070604242403950454030204145435025100All LA CountyWomenAsianHEALTHINDICATORSFORFORWOMENIN LOSANGELESCOUNTYHEALTHINDICATORSWOMENIN LOSANGELESCOUNTY – 2017BlackLatinaWhite Latinas continue to make upthe largest proportion of womenin Los Angeles County (46%),followed by white (30%), Asian(14%), black (9%), NativeHawaiian and Other PacificIslander (0.4%*), and AmericanIndian/Alaskan Native (0.2%)women.1 Half of Latinas (50%) are 18 to39 years of age while 30% ofwhite women are 65 years ofage or older.1 L atinas are almost threetimes (72%) more likely toreport household incomesless than 200% FPL comparedto white women (24%).1a A higher percentage of blackwomen (31%) and white women(31%) report a disabilitycompared to Latinas (18%)and Asian women (12%).1b About 76% of Asian women and64% of Latinas are foreign born;among those, 92% of foreignborn Latinas report living inthe U.S. for 10 years or longercompared to 72% of foreignborn Asian women.1 Overall, about 62% of women7 in Los Angeles County reportmostly speaking English athome, and the percentage islower among Latinas (38%)and Asian women (47%)compared to black women (99%)and white women (94%).1 A higher percentage of blackwomen (72%) report beingsingle compared to Asianwomen (44%), white women(43%) and Latinas (43%).1d7
Women: Race/EthnicityEducation Percent of adults with less than a high school education1 Percent of adults who completed high school1 Percent of adults who completed some college, trade school, or associate’s degree1 Percent of adults with a college degree1 Percent of adults with a postgraduate degree1Employment Status Percent of adults who are employed1 Percent of adults who are unemployed (and looking for work)1 Percent of adults not in the labor force (includes retired, disabled, andunable to work)1Housing Percent of adults who report owning their home1 Percent of adults who report housing instability (homeless or not having their ownplace to live or sleep in the past 5 years)1Food Percent of adults with household incomes 300% FPL who are food insecure1e Percent of adults with household incomes 185% FPL who participate in theSupplemental Nutrition Assistance Program (SNAP)1 Percent of adults who eat and have access to fresh fruit and vegetables in theirneighborhood that report the fruit and vegetables are always or usually affordable2Neighborhood Percent of adults who believe their neighborhood is safe from crime1 Percent of adults who report their neighborhoods do not have walking paths, parks,playgrounds, or sports fields1 Percent of adults who consider tap water safe for drinking in their community1Violence Percent of adults who report ever experiencing physical and/or sexual violence byan intimate partner1 300% FPL200-299% FPL100-199% FPL 100% FPLWhiteLatinaBlackAsianLos Angeles County WomenLos Angeles County Men and WomenDETERMINANTS OF HEALTHHealthy People 2020 Target8Women: Federal Poverty Level .817.8
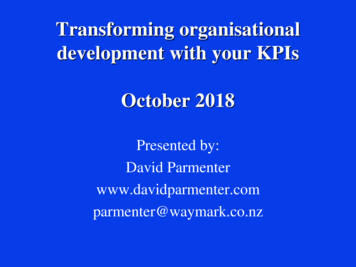
Percent of women with a recent live birth who report experiencing physical and/orsexual violence during their pregnancy3 Rate of emergency room visits (treated and released) for intimate partner violenceinjuries per 100,000 adults4a Rate of emergency room visits (treated and released) for assault injuriesper 100,000 adults4b Rate of hospitalizations for non-fatal assault injuries per 100,000 41.9*14.17.56.8N/AN/AN/AN/AN/AN/AN/AN/AN/A247.6 181.435.9616.7 150.4 9.122.219.522.3N/A32.738.931.1* 21.2*35.250.942.734.451.035.9Discrimination Percent of women with a recent live birth who report experiencing at least oneincident of discrimination over her lifetime3aSocial Support Percent of adults who report receiving the social and emotional support they need1Caregiver Percent of adults who provided care or assistance during the past month to anotheradult who is aging or living with a long-term illness or disability1 Percent of caregivers who cared for a person with memory loss or Alzheimer’sdisease in the past month1N/A Data not available where noted*Estimate is statistically unstable**Cell size less than 5 - data not reported due to confidentialityDeterminants of Health among Women in Los Angeles Countyby Federal Poverty Level (FPL), 20151 100% FPL100-199% FPL200-299% FPL 300% FPL1009494Percent of wn a homeHEALTH INDICATORS FOR WOMEN IN LOS ANGELES COUNTY – 2017Neighborhood safe fromcrime Latinas are at least four times(45%) more likely to have lessthan a high school educationthan Asian (10%), black (10%),and white (5%) women.1 The percent of black women whoare unemployed and looking forwork only minimally decreasedfrom 17% in 2011 to 16% in2015.1 Only 1 in 4 women with household incomes less than 100% FPLreport owning their home (23%),compared to 77% of women withhousehold incomes 300% FPLor above.1 A higher percent of black women(37%) and Latinas (36%) withhousehold incomes less than300% of FPL are food insecurecompared to white (23%) andAsian (14%) women.1eGroup fares betterGroup fares worseNo statistical testing done A significantly lower percent ofLatinas (75%) and black women(66%) report their neighborhoodis safe from crime comparedto white (95%) and Asian (86%)women.1 A significantly higher percentof black women (25%) and whitewomen (24%) report everexperiencing physical and/orsexual violence by an intimatepartner compared to Latinas(13%) and Asian women (7%).1 R ate of hospitalizations(42/100,000) and emergencyroom visits (617/100,000) fornon-fatal assault injuries isthree to four times greater forblack women compared to LosAngeles County women overall(12/100,000 and 181/100,000respectively).4b9
Women: Race/EthnicitySelf-Rated Health Percent of adults who report their health to be fair or poor1Poor Health Days Average number of poor mental health days reported by adults in the past month1 Average number of poor physical health days reported by adults in the past month1Days of Activity Limitation Average number of days in the past month for which adults reported their regulardaily activities were limited due to poor mental or physical health1Emotional Well-Being Percent of adults with moderate to severe psychological distress who report social lifeimpairment in the past year2a,2b Percent of working adults 70 years or younger with moderate to severe psychologicaldistress who report work life impairment in the past year2a,2b Percent of adults with moderate to severe psychological distress who report familylife impairment in the past year2a,2bLife Expectancy Average life expectancy at birth (in years)5 Percent of population who are expected to live to age 25 years5 Percent of population who are expected to live to age 65 years5 Percent of population who are expected to live to age 85 years5 300% FPL200-299% FPL100-199% FPL 100% FPLWhiteLatinaBlackAsianLos Angeles County WomenLos Angeles County Men and WomenHEALTH STATUSHealthy People 2020 Target10Women: Federal Poverty Level 57.669.743.161.754.1N/AN/AN/AN/AN/A Data not available where noted*Estimate is statistically unstable In Los Angeles County, anestimated 872,000 or 22%of women report their healthstatus to be fair or poor.1Group fares betterGroup fares worseNo statistical testing done L ife expectancy at birth forwomen has increased from 81.4years in 2000 to 84.5 years in2013, and in 2013 it was 5 yearslonger than life expectancy formen (79.5 year
Los Angeles County Cancer Surveillance Program, USC UCLA Center for Health Policy Research U.S. Census Bureau Report Design and Layout by Kathleen Pittman, Pittman Creative Summer Nagano, Office of Women's Health Special Thanks to Office of Women's Health Policy Council Women's Health Data Committee 2 HEALTH INDICATORS FOR WOMEN IN LOS .