Transcription
43rd Annual 2016 KY School of Alcohol and Other Drug Studies Louisville, KY July 17-19, 2016Treatment: The Connection Between Trauma andSubstance Use Disorders: Creating A HealingProcessHendree Jones, PhDProfessor, Department of Obstetrics and Gynecology, Executive Director,UNC HorizonsUNC Chapel Hill, NC
2Outline Define trauma and how it effects a personover the lifespan Identify the elements of theneurodevelopmental view of childhoodtrauma that can help guide treatments forwomen with substance use disorders andchildren Acquire practical tools to identify past andcurrent IPV Make brief office interventions to assist IPVvictims, and offer strategies to referCredit: inking-72318/
3What is Trauma: The EventA traumatic event is one in which a personexperiences (witnesses or is confronted with): Actual or threatened death Serious injury Threat to the physical integrity of self or anotherResponses to a traumatic event may include Intense fearHelplessnessHorrorDetachmentSAMHSA's Trauma and Trauma-Informed Care Experts Meeting; Andersen, R., (2012). SAMHSA's Trauma andTrauma-Informed Care Experts Meeting.
4What is Trauma: The Response Frequently, a sense of humiliation,betrayal, or silencing often shapes theexperience of the event. How the event is experienced may belinked to a range of factors:ooothe individual's cultural beliefsavailability of social supportsthe developmental stage of theindividualSAMHSA's Trauma and Trauma-Informed Care Experts Meeting; Andersen, R., (2012). SAMHSA's Trauma andTrauma-Informed Care Experts Meeting.
5Defining Trauma Individual trauma results from an event, series of events, or set ofcircumstances that is experienced by an individual as physically oremotionally harmful or threatening and that has lasting adverseeffects on the individual's functioning and physical, social,emotional, or spiritual well-being. Events and circumstances may include the actual or extreme threatof physical or psychological harm or the withholding of material orrelational resources essential to healthy development. These eventsand circumstances may occur as a single occurrence or repeatedlyover time. The individual's experience of these events or circumstances helpsto determine whether it is a traumatic event. A particular event maybe experienced as traumatic for one individual and not for another.Adapted from Griffin,E., (2012). Presentation at the NIDA/ACYF experts meeting on trauma and child maltreatment; Wilson, C. and Ford, J., (2012). SAMHSA'sTrauma and Trauma-Informed Care Experts Meeting; Andersen, R., (2012). SAMHSA's Trauma and Trauma-Informed Care Experts Meeting.
6What is Trauma: Effects The long-lasting adverse effects on an individual result from theindividual's experience of the event or circumstance. These adverse effects may occur immediately or over time. Some peoplemay not recognize the connection between the effects and the events. Examples of adverse effects include an individual's inability to: Cope with the normal stresses and strains of daily livingTrust and benefit from relationshipsManage emotions, memory, attention, thinking, and behaviorNeuro-physiological make-up, health and well-being can be harmedTraumatic experiences can lead to a constant state of arousal which eventuallywears a person down, physically, mentally, and emotionallyAdapted from Griffin,E., (2012). Presentation at the NIDA/ACYF experts meeting on trauma and child maltreatment; Wilson, C. and Ford, J., (2012). SAMHSA'sTrauma and Trauma-Informed Care Experts Meeting; Andersen, R., (2012). SAMHSA's Trauma and Trauma-Informed Care Experts Meeting.
7TraumaThe event the way the event isexperienced the effect on the person TraumaAdapted from Griffin,E., (2012). Presentation at the NIDA/ACYF experts meeting on trauma and child maltreatment; Wilson, C. and Ford, J., (2012). SAMHSA'sTrauma and Trauma-Informed Care Experts Meeting; Andersen, R., (2012). SAMHSA's Trauma and Trauma-Informed Care Experts Meeting.
8Types of TraumaOngoing abuse and violence can induce feelings of shock disbelief confusion terror isolation despair loss of self worthThese, in turn, can manifest as psychiatric symptoms (e.g., hyperarousal,depression, anxiety, and sleep disruption).Possible to develop chronic posttraumatic stress disorder (PTSD), adisorder that is a common response to overwhelmingtrauma and that can persist for years.
9Types of TraumaInterpersonal behaviors/interpersonal-violence/
10InterPersonal Violence (IPV):DefinitionA systematic pattern of intentional intimidation throughthe use of threats and violence for the purpose ofgaining power and control over one’s partner in anintimate ove-hatred-1377511/10
11IPV: Types Physical: Assault on the victim’s person (hit, kick,slap, etc.) Sexual: Forced or unwanted sexual acts Psychological: Woman’s psychological well-beingdeteriorates or remains at an unhealthy level(threats, destruction of property, etc.)11
12Facts About Trauma What trauma is/ How common it is How trauma effects the brain and body Relationship between trauma, substance use, andother mental health issues
13Facts About InterpersonalViolence/Trauma (IPV) Approximately 960,000 incidents of violence against a currentor former spouse, boyfriend, or girlfriend per year More than 1 in 3 women in the USA have experienced rape,physical violence, and/or stalking by an intimate partner More than 1 in 4 men in the United States have experiencedrape, physical violence, and/or stalking by an intimate partner Nearly 80% of female offenders with a mental illness reporthaving been physically and/or sexually abused More than 3 in 4 women and men in treatment for substanceuse disorders report trauma histories(U.S. Department of Justice, 1998; The Commonwealth Fund, 1999.;CDC,2013; Marcenich, 2009; SAMSHA/CSAT, 2000)
14Pregnancy Does Not Protect AgainstTrauma Review of the literature reported 1-20% prevalence of IPVduring pregnancy Among 104 Appalachian women during pregnancy: 81% reported some type of IPV during the current pregnancy 28% reporting physical IPV 20% reporting sexual violence Among 715 urban drug-dependent pregnant women attendinga drug addiction treatment program: Lifetime: 73% physical 71% emotional 45% sexual During pregnancy: 41% emotional, 20% physical 7% sexual
15Trauma: A Pediatric Health Crisis A report of child abuse is made every ten seconds in the USA Approximately 5 children die every day because of child abuseand/or neglect.(Childhelp, 2013; Child Welfare Information Gateway, 2006)
16Trauma: A Pediatric Health Crisis Children who experience child abuse and neglect are: 59% more likely to be arrested before 18 years of age 28% more likely to be arrested as an adult 30% more likely to commit violent crime(Childhelp, 2013; Child Welfare Information Gateway, 2006)
17The Adverse Childhood ExperiencesStudyAuthors: Drs. Robert Anda and Vincent FelittiN 17,421 adults who were having medicaldifficulties received a survey about theirchildhood experiences9 categories of adverse childhood experienceswere examinedA person’s ACE score is sum of the number ofcategories a person experienced
18Adverse Childhood Experiences:ACE Categories1.2.3.4.Recurrent physical abuseRecurrent emotional abuseSexual abuseNeglectGrowing up in a household where therewas:5. Domestic violence6. An alcoholic or drug abuser7. Someone chronically depressed, mentally ill or suicidal8. At least one biological parent was lost to the patient duringchildhood – regardless of cause9. Someone in prison
19ACE Study Demographics
20ACE Study Results Shows a relationship between aperson’s adverse childhood experienceand their physical and mental health asadult as well as death The higher the ACE score the greater thelikelihood that person would suffersignificant health problems in adulthood––––––Heart DiseaseChronic Lung DiseaseLiver DiseaseSuicideInjuriesHIV and STDs
21ACE Scores Are Related ToHealth Adolescent HealthTeen pregnancySexual abuseRisk of re-victimizationSmokingAlcohol use disordersIllicit drug use disordersMental healthRelationship stabilityWorkforce performance
22The ACE Pyramid
23Radiating Effects of TraumaPsychologicalPhysical/Stress Related AnxietyDepression/SuicidePTSDPoor self-esteemBlame and guiltUncontrollable emotionsSocial Isolation/Withdrawn Few social interactions Rigid sex-role expectationsCredit: le-face-818464/InjurySleep problemsNutritional/ Low weight gainSubstance use/ SmokingChronic painHypertensionInadequate prenatal careMiscarriagePre-term laborFetal fracture/ Fetal deathPlacental abruptionUterine rupture
24Trauma’s Effects on Children Children living in homeswhere there is domesticviolence are 15 times morelikely to be abused thanchildren from non-violenthomes - Hurt while trying to intervene Abuse and Neglect Sleeping disorders- Parents usually think childrendo not know what ishappening Children witness between 6080% of assaults When children live withinterpersonal violence theymay witness some of thephysical violencePhysical injuries Difficulty falling asleepWake frequentlyRefuse to sleep in their own bedNight maresAnxiety- Worry about parents- Worry about self PTSD
25The Brain and Trauma At birth about 100 billion neurons have been produced Genes (genetic code) and the environment both influencehow a baby’s brain develops Genes are responsible for the basic wiring of the brain Environment and experience are responsible for the finetuning of those ntiation-nerve-cell-1333354/
26The Brain and TraumaThe brain has a “bottom-up” organization
27The Brain and Trauma:Limbic System Responsible for:– Emotions– Attachment– Memory Regulates:– Appetite– Hormones– Immune system– Sexual urges– Sleeping
28The Brain and Trauma:Cortex Upper brainMakes up two-thirds of the brainCrumpled up space – if unfolded it would be about half a square yardDivided into two hemispheres and 4 lobesRegulates decision-makingControls thinking, reasoning and languageUnderstands time – past, present, futureAllows reflection, decisions and actionsResponsible for abstract thinkingContains 80% of the neurons
29The Brain and Trauma:Cortex Development The ability to regulate reactivity is related to how well yourcortex works Mature cortex controls aggressive and impulsive behaviorsbetter Factors that impair cortex functioning increases reactivity Alcohol/drugs Stress Trauma
30The Brain and Trauma:Connections Form Neurons and neuronal connections (synapses) changein an activity-dependent fashion This "use-dependent" development is the key tounderstanding the impact of maltreatment on children These areas organize during development and changein the mature brain in a "use-dependent" fashion
31The Brain and Trauma:Modified by Experience The more a neural system is activated, the more it will "build-in" thisneural state What occurs in this process is the creation of an "internalrepresentation" of the experience corresponding to the neuralactivation This "use-dependent" capacity to make an "internal representation"of the external or internal world is the basis for learning and memory The result of this sequential neurodevelopment is that theorganizing, "sensitive" brain of an infant or young child is moremalleable to experience than a mature brain
32The Brain and Trauma:Changes in Childhood The brain is most plastic (receptive to environmental input)in early childhood The consequence of sequential development is that asdifferent regions are organizing, they require specific kindsof experience targeting the region's specific function (e.g.,visual input while the visual system is organizing) in orderto develop normally These times during development are called critical orsensitive periods
33Brain Development andCaregiversA baby’s relationship with her primary caregivershas the biggest effect on how the brain developsBabies learn from the responses they receivefrom caregiving adultsWhen parents and caregivers respond in apositive, attentive way, babies begin to learn tocare about others.
34The Brain and Trauma:Maltreatment Effects If maltreatment leads to disruption in the timing, intensity, qualityor quantity of normal developmental experiences, however, it canhave a devastating impact on neurodevelopment – and to brainfunction Healthy development results in a top-heavy ratio of cortical andlimbic system relative to the midbrain and brain stem However, maltreatment during sensitive periods of braindevelopment can change the ratios to make the brain more bottomheavy, with lasting results
35The Brain and Trauma:ChangesImpact of Adverse Stress on the Brain and Brain DevelopmentWith trauma and neglect, the midbrain is overactive and grows in sizewhile the limbic and cortical structures are stunted in growth
36The Brain and Trauma:Stress Response Children that learn the caregiverwill be unavailable and/orrejecting when the child needshim/her may develop a chronicactivation of the physiologicalstress-response system The early memories of traumaexperiences may adversely colorour view of the world throughoutour lives
37The Brain and Trauma:Stress Response Exhaustion Adverse childhood experiences, which lead to chronically activatedstress systems, have detrimental, long-term effects on physicaland mental health The results of the chronically activated stress response systemmake the provider’s goal clear: To normalize the stress response to allow for a return to a calmsecure state.
38Impact of Early StressChildhood StressHyper-responsivestress responseDecreased copingChronic Flight orFightIncreased cortisolChanges in theBrain architecture
39Example of ChildhoodAdversity A young child living in a home with an abusive caregiver willcreate a set of associations between a multiple neutral cues andthreats These neural-cue associations become automatic – and will elicitfear response for the rest of the child’s life The cues can be smells, sounds, types of touch, sights, facialexpressions, body language In order to change these associations, the child must haveopportunities for new experiences that will allow the brain todecrease the overgeneralization of these trauma-relatedassociations
40Protective Factors AgainstTraumaDr. Bruce Perry’s Six Core Strengths for Children: A Vaccine Against ViolenceATTACHMENT: being able to form and maintain healthy emotional bonds andrelationshipsSELF-REGULATION: containing impulses, the ability to notice and controlprimary urges as well as feelings such as frustrationAFFILIATION: being able to join and contribute to a groupATTUNEMENT: being aware of others, recognizing the needs, interests, strengthsand values of othersTOLERANCE: understanding and accepting differences in othersRESPECT: finding value in differences, appreciating worth in yourself and othersFor more information on the Six Core Strengths, visit the “Meet Dr. Bruce Perry” page perry
41Interpersonal Violence:Intergenerational Cycle of Violence“A child’s exposure to the father abusing the mother is the strongest riskfactor for transmitting violent behavior from one generation to the next.”(American Psychological Association Presidential Task Force on Violence and the Family, 1996)Partner MaltreatmentSiblingsPeersMaltreatment ViolenceChild Abuse and Neglect
42Substance Use Disorders arePediatric IllnessesJust 5 percent of youth with a substance usedisorder get ata-teds
43Issues Facing Women withSubstance Use Disorders Exposure to violence and trauma Generational drug use Multiple psychiatric issues Legal involvement Gender inequality Lack of formal education Male-focused society Unstable housing History of child abuse and neglect Multiple drug exposures Limited parenting skills/resources Lack of job acquisition and maintenance skills Food insecurity and lack of nutrition Lack of positive/supportive relationships These factors with or without drug use can influence mother andchild outcomesCredit: “Stress Definition Indicates Explanation Pressures And Tension” by Stuart Miles
44Trauma Exposure: A Risk Factor forWomenHistory of Interpersonal Violence, Childhood SexualAbuse, and Other Traumas History of traumatic events, including:- sexual and physical assaults- childhood sexual and physical abuse- domestic violencehave been found to predict both initiation of drug use anddevelopment of drug use disorders in women Najavits et al. (1997) reported a lifetime history of trauma in 55-99% percentof women who used drugs, compared with population-based rates of 3651%Credit: -641528/Agrawal et al. 2005, Brady & Ashley, 2005; Hawke et al., 2000; Pettinati et al., 2000
45Challenges in Treating TraumaticStress and Substance Use Disorders Drug abstinence may notresolve comorbid traumarelated disorders – forsome PTSD may worsen 12-Step Models often donot acknowledge theneed for pharmacologicinterventions Confrontationalapproaches typical inaddictions settingsfrequently exacerbatemood and anxietydisorders Treatments for PTSDonly —such asExposure-BasedApproaches often maynot be advisable to treatwomen with addictionsor may be marked bycomplications
46Treatments for Trauma andSubstance Use Disorders– Sequential Model: Initial phase may focuson substance use disorder relatedsymptoms in preparation for working ontrauma related symptoms later– Concurrent Model : Additionalcomponents may be delivered at the sametime but sometimes in parallel– Integrated Model: Components are allworking together; one informing the other
47Trauma-Informed CareA definition of trauma-informed approach incorporates three keyelements:(1) Realizing the prevalence of trauma(2) Recognizing how trauma affects all individuals involved withthe program, organization, or system, including its ownworkforce(3) Responding by putting this knowledge into practice47
48Integrating Trauma TreatmentTrauma-Informed Treatmentvs.Trauma-Specific Treatment
49Trauma-Informed Services:Characteristics (WCDVS) Aware of the role of violence and victimization inwomen’s lives Minimize victimization and re-victimization Hospitable and engaging for survivors Facilitate recovery and healing Empower Respect a woman's choices and control over herrecovery Goals are mutual and collaboratively established Emphasize women’s strengthsSource: The Women, Co-Occurring Disorders and Violence Study 2015
50Trauma-Informed Services:Principles (WCDVS) Respect trauma as a central concern in awoman’s life Symptoms are adaptations to traumaticexperiences Reframe ‘Adaptive’ behavior as positivecoping Violence and trauma have broad impact Providers need to meet the woman whereshe is in her life experienceSource: The Women, Co-Occurring Disorders and Violence Study 2015
51Examples of Evidence-BasedTrauma-Specific and SUDInterventions ARTS: Assisted Recovery from Trauma andSubstances ATRIUM: Addictions and Trauma RecoveryIntegrated Model COPE: Concurrent Treatment with ProlongedExposure CBT for PTSD(Triffleman et. al, 1999)(Miller & Guidry, 2001)(Back et al., 2014)(McGovern et al., 2010) Seeking Safety Transcend(Najavits, 1998; www.seekingsafety.org)(Donovan et al., 2001)
52NIDA Clinical Trials NetworkTrauma Group Study SitesWashington NodeResidence XIIOhio Valley NodeMaryhavenNew England NodeLMG ProgramsNew York NodeARTCSouth Carolina NodeCharleston CenterFlorida Node GatewayCommunityFlorida NodeThe Village
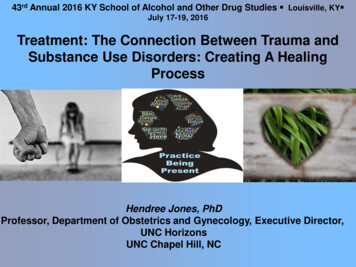
53Pathways to change: Use trajectories followingtrauma‐informed treatment of women with co‐occurringpost‐traumatic stress disorder and substance usedisordersSeeking Safety substance abusetreatment-as-usual (TAU) vs. Women’sHealth Education TAU.The researchers looked at the effect ofthese treatment options on bothsubstance use and the severity of PTSDsymptoms.Analyses showed large, clinicallysignificant reductions in PTSDsymptoms over the course of treatmentand follow-up, but no reliable differencebetween the study groups.Substance use outcomes were not significantly different over time between the two treatments andat follow-up showed no significant change from baseline.Drug and Alcohol ReviewVolume 34, Issue 3, pages 242-251, 4 MAR 2015 DOI: i/10.1111/dar.12230/full#dar12230-fig-0001
54NIDA Clinical Trials NetworkTrauma Group Study Sites Findings highlight the benefit of multiple treatment episodesand the relevance of adopting a broader, ‘long-range’ lens. SUD treatment careers of women played a significant role inwhich post-treatment use trajectory they would ultimatelyfollow. Those who reduced their PTSD symptoms during treatmentwere better able to manage their substance use in the yearfollowing treatment For clinicians, interventions for PTSD will not negativelyimpact SUD treatment, but may very well reduce the need ofpatients to use substances for self-medicating purposes.(Alvarez and Sloan, 2010)
55Phases of leranceProcessExposureCognitiveSomatosensory
56Potential forVicarious Traumatization Sensitivity for counselor survivors Conducting trauma treatment should be voluntary Supportive environments– Moderate caseloads– Regular bracing-loving-718562/
57Supervision is Critical Protocol training is only the beginning A safe place Individual or group supervision Should not be on the ‘back burner’ Ensure fidelity to the treatment
58Counselor Self-Care Practice what you tell others to do Rest and exercise Opportunities for personal renewal Personal therapy
59SAMHSA’s Six Key Principles of aTrauma-Informed ApproachThese principles may be generalizableacross multiple types of settings, althoughterminology and application may besetting- or sector-specific:1. Safety2. Trustworthiness and transparency3. Peer support4. Collaboration and mutuality5. Empowerment, voice and choice6. Cultural, historical, and gender issues
60Core of Trauma-Informed CareIf a program can say that its culture reflects each ofthese key principles in each contact, physical setting,relationship, and activity and that this culture isevident in the experiences of staff as well as thepatients/clients, then the program’s culture is traumainformed60
61Trauma-Informed CareThe event the way the event isexperienced the effect on the person TraumaHow we respond to the event in the shortterm and long terms matters!Healing must be the focusAdapted from Griffin,E., (2012). Presentation at the NIDA/ACYF experts meeting on trauma and child maltreatment; Wilson, C. and Ford, J., (2012). SAMHSA'sTrauma and Trauma-Informed Care Experts Meeting; Andersen, R., (2012). SAMHSA's Trauma and Trauma-Informed Care Experts Meeting.
62Trauma-Informed Care: Tools forHow to RespondDBT SkillsMindfulnessDistress ToleranceEmotional RegulationInterpersonal Effectiveness
63Interpersonal Violence:EmpowermentRespectConfidentialityBelieve Her andValidate HerExperiencesPromote Access toCommunity ServicesADVOCACYADVOCACYHelp Her PlanAcknowledge theInjusticefor Future SafetyRespectHerAutonomyDomestic Violence Project
64How to Identify Someonewith IPV64
65Reluctance to Assess Fear of re-traumatizing or upsettingpatients No follow-up support Feeling intrusive One’s own abuse issues Denial65
66Know Your State Laws Disclosing Limits of Confidentiality mandated reportingresponsibilities should always be discussed with patientsseeking care prior to assessing for domestic violence. It is absolutely critical for health care providers to ALWAYSdiscuss the limits of confidentially prior to doing anassessment for domestic or sexual violence. Providers need to be familiar with their state law and how it isimplemented. Not disclosing these limits can harm therelationship between patient and provider, can bedisempowering to the patients choice to disclose/not disclosedomestic violence and may put the patient at risk for retaliationby the batterer.66
67Primary Care PTSD Screen(PC-PTSD) Designed for use in primary care and other medical settings. Thosescreening positive should then be assessed with a structured interview forPTSD.Instructions:In your life, have you ever had any experience that was so frightening,horrible, or upsetting that, in the past month, you: Have had nightmares about it or thought about it when you did not wantto? YES / NO Tried hard not to think about it or went out of your way to avoidsituations that reminded you of it? YES / NO Were constantly on guard, watchful, or easily startled? YES / NO Felt numb or detached from others, activities, or your surroundings?YES / NOResearch suggests that the results of the PC-PTSD should be considered"positive" if a patient answers "yes" to any three items.67
68Substance Use during Pregnancy:Recognize Risk of ViolenceWomen Abuse Screening Tool (WAST) – Short (4 min to complete) In general, how would you describe your relationship?m A lot of tension m some tension m no tension Do you and your partner work out arguments with m Great difficulty m some difficulty m no difficulty Endorsing both underlined items correctly classified 92% victim and100% non-victim68
69HOW TO HELPSOMEONE WITH IPV69
70Responding To Risk of Violence If a person endorses these or other questions indicatingrisk for violence: Listen to him/her and believe herAcknowledge his/her feelings and let him/her know sheis not aloneLet him/her know that no one deserves to be abusedProvide resources (hotline, shelter, spiritual)70
71Empowering Survivors Strength based not deficit based approachPractice empathyPractice gratitudePractice recovery languagePractice telling story of recoveryPractice advocacyPractice parenting skillsPractice employment seeking skillsPractice economic independence skillsIndividualized care for attachment challenges
72Educate About Danger and AdaptTreatment ResponseSigns of Increasing Danger Recognizing that there is a highchance that women andexperienced one or moretraumatic brain injuries (TBI)Abuse happens more frequentlyAbuse gets rougherAbuser tries to choke herAbuser threatens to kill her A TBI has implications forThere is a gun in house/cartreatment and how best to helpAbuser forces sexwomen learn, remember andapply informationAbuser uses drugsAbuser hits woman during pregnancyAbuser has been reported for child abuseAbuser is extremely jealous, possessive, controllingJ. C. Campbell, Assessing Dangerousness, 1995.
73Support:Action PlanPatient ContactDocumentation in patient’s medical record Acknowledge Safety Containment Support/Affirm Focus on coping ReferralPatient’s own words of injury or abuseDiagram of the injuries (body map)Photographs of injuries (consent needed)Police phone callsSafety plan discussedMedical follow-up care advisedCommunity resources recommended
74IPV: Empowerment Advocacy RespectConfidentialityBelieve Her/Him and Validate Her/HisExperiencesPromote Access to Community ServicesHelp Her/His Plan for Future SafetyAcknowledge the InjusticeRespect Her/His Autonomy74
75What is Safety? Achieve abstinence from substances Eliminate self-harm Acquire trustworthy relationships Gain control over overwhelming symptoms Attain healthy self-care Remove oneself from dangerous situations (such asdomestic violence, unsafe sex) Seeking Safety: Lisa Najavits75
76SummaryCumulative experiences of stress andtrauma can alter brain developmentand have important implications forhow we treat patientsTrauma is a common and critical issueto address to help improve thepatient’s health and well-beingProviders can play a key role in helpingempower women to find safety andremain safe and healthyCredit: inking-72318/
6 The long-lasting adverse effects on an individual result from the individual's experience of the event or circumstance. These adverse effects may occur immediately or over time. Some people may not recognize the connection between the effects and the events. Examples of adverse effects include an individual's inability to: Cope with the normal stresses and strains of daily living