Transcription
Treating deadly aneurysms withrevolutionary hybrid technique
-Fall 2019insideLHSCTable of ContentsPatient Experiences03Changing lives throughlifestyle and surgicalinterventionLHSC’s Bariatric Centre of Excellenceoffers a rigorous, full-service bariatricsurgery program.06Treating deadly aneurysmswith thoraflex graft leadsto quicker recoveryBarbara Palmateer had a remarkable recoveryfrom complex aortic surgery and was back toher routine after one month. Recovery fromconventional complex aortic surgery can takeup to a year.12Prostate cancer is also ayounger man’s diseaseJohn Oliveira was in his 40s when he wasdiagnosed with prostate cancer. He is passionateabout raising money for research and awarenessthat prostate cancer is also a young man’s disease.In Focus08LHSC’s Multi-Organ TransplantProgram: a rich history ofinnovation, bold future aheadA transplant program steeped in discovery andworld firsts continues its quest for innovationsthat extend the boundaries of transplantationto better the lives of patients.Research & Innovation14No Fixed AddressIn a community-focused project from LawsonHealth Research Institute, a team of researchersis tackling the issue of homelessness from withinhospital walls.PATIENT EXPERIENCESWho We AreOne of Canada’s largest academic healthorganizations with a mandate of care,teaching and research, London HealthSciences Centre (LHSC) cares for the mostcritically ill patients in the region. Located inLondon, Ontario, Canada, LHSC encompasses: University Hospital Victoria Hospital Children’s Hospital Byron FamilyMedical Centre Victoria FamilyMedical CentreCHANGING LIVESthrough lifestyle and surgical interventionWhen Lori Masterson shops for clothes now, she’s likely to come home with outfits much too big for her.Six months past her bariatric surgery, Lori has lost 90 pounds and can’t quite recognize herself in the mirror.“I still don’t see the weight loss in myself, I don’t see it to the degree that other people notice it,” says Lori, who has had twocomplete wardrobe changes since surgery in January.“I have so much more selection and shop in regular clothing shops now, before I had only two stores to shop for clothing in London.” Kidney Care Centre(at WestmountShopping Centre) 54 Riverview Avenue siteLHSC is the home of: CSTAR (Canadian Surgical Technologies andAdvanced Robotics) Fowler Kennedy Sport Medicine Clinic London Regional Cancer ProgramDid You Know?15Anesthesiologists provideindividualized patient care Children’s Health Research Institute Lawson Health Research Institute Children’s Health Foundation London Health Sciences FoundationAnesthesiologists are the physiciansresponsible for the careful administration ofanesthetics before, during and after surgery.You Asked Us16Treating deadly aneurisms withrevolutionary hybrid techniqueOn the CoverDr. Michael Chu and his team areleaders in the use of the thoraflexgraft for complex aortic surgery.Read the story on page 6.02How does the EmergencyDepartment triage patients?The triage system is a standard sortingprocess used in emergency departmentsacross Canada that determines how quicklypatients receive care depending on theseverity of their illness.Patient feedback: Your feedback is important tous and helps us to be better. The Patient Relationsoffice is here to support you. Whether you have acomplaint, a suggestion, a compliment or a good storyto share, we’d like to hear from you. The PatientRelations office can be contacted at 519-685-8500ext. 52036.Visit us onlineVisit inside.lhsc.on.ca to read more,browse previous issues and watch videos.And don’t miss the next issue of insideLHSC!033
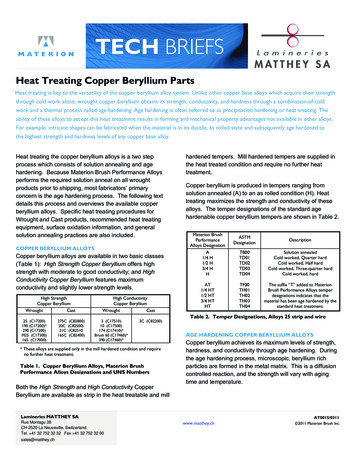
PATIENT EXPERIENCESHer weight loss has brought about significant health benefits.Her blood pressure is down to normal, her blood sugar andcholesterol levels are good. She is being referred to the sleepclinic to see if her sleep apnea has improved.Lori is thankful for regaining her health and for her careat LHSC.“Everyone on the care team was incredibly supportive,”says Lori. “Life is easier, work is easier and, most importantly,keeping up with my daughter is easier.”Were there any unexpected changes since surgery?“There’s the first time your clothing size changes. I don’tthink I was quite prepared for how fast your size changes,”says Lori.“It takes longer to catch up with the mental picture of whatsize I am. I see an image in the shop window and it takes me afew seconds to realize that it’s me.”London HealthSciences CentreBariatric Centreof Excellence“We offer a rigorous, fullservice bariatric surgeryprogram that startswith assessment, andprovides comprehensivecare before, during andafter surgery,” says Dr.Christopher Schlachta,surgeon and regional leadfor bariatric surgery at LHSC.Dr. Christopher Schlachta, left, and Dr. Ahmad Elnahas performed gastric bypass surgery on Lori Masterson.Lori has struggled with her weight her wholelife. Ten pounds at birth, she has always beenconsidered a bigger person.Health issues led her to consider bariatricsurgery. She had high blood pressure, sleepapnea, poor blood sugar and high cholesterol.“I have a 10-year-old daughter who needsa healthy mom and dad. She was my mainmotivator,” says Lori. “I couldn’t have lostweight and regained my health without surgery.I had tried different programs in the past,but I could never lose the weight. I neededa bigger tool.”Bariatric surgery reduces the patient’sstomach and therefore limits the amount offood and liquid that can be consumed.When her husband Kevin made the decisionto have bariatric surgery two years ago to helpovercome obesity, he had to travel to Windsorfor appointments and then to Toronto to havethe surgery.Two years later, Lori was able to receivethe same services in London with theestablishment of the Bariatric Centre ofExcellence at LHSC.Her family physician referred her to thebariatric centre at LHSC and she went to herfirst information session, taking along twofriends to support her.04The two-hour session includes anoverview of the program, patientquestionnaire, as well as a referral forblood work and a stomach ultrasound.A few weeks later, Lori had her initialnursing assessment to review her completedquestionnaire, consent for research,set up a sleep study, and ensure all testingwas complete.“I have a 10-year-olddaughter who needsa healthy mom anddad. She was my mainmotivator.”–Lori MastersonAt this time important bariatricinformation – the process, expectationsand possible complications – and therequirement for a long-term commitment tolife-style change were reviewed to ensure sheunderstood the full implications of the surgery.“We also had a nutrition class which talkedabout food intake after surgery and what lifewill look like three months after surgery, whatour new normal would be,” says Lori.Patients then have a number of individualappointments to assess readiness for surgeryand post-surgery life, including an assessmentwith a social worker.Social worker Claire Davies works withpatients to assess, for example, social supports,the ability to deal with the stress of surgery,and any past substance abuse or psychiatricdisorder. She also does screening for bingeeating disorders, night cravings, and bulimia.“When we meet again for our secondappointment, we talk about their emotionaltriggers for food and how they are coping tofurther their awareness, and we talk about howto make lifestyle and behaviour changes,” saysClaire. “Emotional eating is most common,and can be triggered by feelings either negativeor positive.”For many people it is difficult to separatethe habit of eating with the activity, such ashabitually snacking when you’re watching TVin the evening.“It’s about relearning to do these activitieswithout food,” says Claire.There is also navigating eating in socialsituations. Claire says some relationships willchange as a result of the significant weight lossand she helps patients build skills for that. Thegoal is to eat three meals a day and three snacksa day, even when they’re not hungry.“After surgery they are working on aschedule to normalize their eating patterns,”says Claire.Post-surgeryLHSC surgeons performed a roux-en-ygastric bypass surgery for Lori. This is alaparoscopic surgery that partitions thestomach by making a small pouch at the endof the esophagus and connecting it to thesmall intestine, thereby bypassing much of thesmall bowel.Lori was home after one night in hospitaland, as outlined in her sessions with an LHSCdietitian along with handouts specifying herdietary requirements, started with liquids,introducing purees and soft foods over aperiod of 10 weeks until she was eating solidfoods again.“When I’m not hungry, food is nolonger a priority and meal prep is no longertop of mind.”While she does not have many foodcravings, she did miss chicken wings, whichwere one of her favourite foods.“So I ate one, but I didn’t feel wellafterwards and now I don’t miss eating them.”“Patients receive thoroughassessments and education priorto bariatric surgery, and are closelyfollowed post-operatively for a period ofup to five years.”The program accepts adult patients with a bodymass index of 40 or higher, or 35-40 with anobesity-related co-morbidity such as sleep apnea,hypertension or diabetes.Obesity is a recognized disease that is caused bymultiple factors including genetics, hormones,and psychology.Over the past year about 200 patients receivedthis surgery at LHSC.Eating after bariatric surgeryLHSC dietitian Helen Abrams works with bariatric surgery patients both before and after surgery.“We are teaching lifestyle changes and healthy eating behaviours from the time of the first orientationsession. It’s about making small changes ahead of the surgery and continuing with these good habits aftersurgery,” says Helen.By the time they have surgery patients have a full understanding of how their lives will change interms of their eating.“We work with the patient to put together a structured eating program that iscustomized to the patient and their lifestyle,” says Helen.The first couple of days following surgery, the patient has only broth, dilutedjuice and unsweetened Jell-O.Helen explains that at this point the stomach pouch is about the sizeof an egg and can take two-to-four tablespoons of food or liquid. Incomparison, the stomach is normally the size of a small football.For the first two weeks after surgery the patient consumes a full fluid dietof milk, yoghurt, cream soups, puddings, and high protein drinks.This is then followed by two weeks of pureed foods such as mashedpotatoes, poached eggs, pureed meats, vegetables and fruits. This isfollowed by four weeks on a soft diet, which includes cheese, crackers,cereals and moist meats, fish, soft cooked vegetables, and peeled fruits.“The point of the progression diet is to respect the healing process of thepouch,” says Helen.At six months the patient begins a regular diet by transitioning in one new foodat a time.Patients sometimes find that some foods they previously enjoyed are no longer as tasty or don’ttaste the same.Eventually the pouch becomes the size of a tennis ball and can hold about one cup of food.A typical day of eating consists of three small healthy meals a day with two to three quality snacks,pairing protein with carbs. Patients eat protein for all meals and snacks, about 80g a day, to keep uptheir energy level.It’s about choosing the right food to make sure that nutritional needs are met, looking at nutrient densefoods and taking their vitamin and mineral supplements every day, says Helen.There is only one item patients can no longer have, and that is carbonated beverages because the air inthe drink fills up and stretches out the stomach.Patients also can’t have any alcohol for the first year and the dietitians encourage lifetime drink avoidance.When do patients stop losing weight?ONLINE EXCLUSIVE“Many plateau at about 12 to 18 months, but everybody is different. Some may plateau sooner and getfrustrated, however this is usually for a short time and then they begin to lose more weight,” says Helen.“Our focus is on how people feel, how healthy they are, their medical benefits, and not on the scale.”Meet Lori andhear her storyVisit us at inside.lhsc.on.ca05
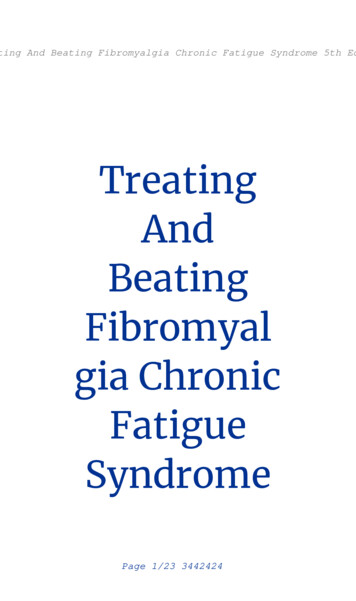
PATIENT EXPERIENCESFROMONE YEAR TOONE MONTHThoraflex graft patientsrecover quicker from complexaortic surgeryMost days Barbara Palmateer swims lengths at the local pool. It is not unusual for herto do 20 to 30 laps, but three years ago she found herself suddenly doing less and less.“One day I could only do one length and I couldn’t breathe. Within a week I hadgone from 20 laps to one, and I felt sick,” says Barbara.The Belleville resident went to her family doctor and was referred for diagnostictesting in Kingston.The hospital in Kingston referred her to London Health Sciences Centre(LHSC) because, as Barbara puts it, there are only a few doctors and hospitals inCanada who do the type of surgery she needed and LHSC is one of them.Tests showed that Barbara had a massive complex aortic aneurysm thatstretched from her heart to her mid-back, impeding her breathing and causingthe shortness of breath.The aorta is the largest artery in the human body and is connected to theleft ventricle of the heart. It sends the blood pumped by the heart to all ofthe organs of the body.If the wall of the aorta becomes weakened it may become enlargedand, like a balloon, become thin and tear when it is stretched. This isknown as a thoracic aortic aneurysm.Dr. Michael Chu, LHSC cardiovascular surgeon, and Dr. AudraDuncan, LHSC vascular surgeon, headed the team of surgeons whooperated on Barbara.The thoraflex hybrid device(in white) enables a completeaortic arch replacement using amuch less invasive procedurewith quicker recovery thanopen heart and endovascularsurgery techniques.The team performed a less-invasive reconstruction byinserting a device called the Thoraflex Hybrid prosthesis.“Barbara had an aortic aneurysm in an area that istraditionally hard to access but this novel approach usesa much less invasive incision than traditionally required,allowing the patient to still receive extensive aortic repairwith a much quicker recovery,” says Dr. Chu.Complex aortic arch aneurysm surgery typicallyrequires one of two types of openings in order for thesurgeons to access the area.It may require a large section of the chest to be cutvertically with an additional section opened from themid-chest to the back of the patient.Or, it requires a full horizontal cut opening the chestfrom one side of the patient to the other, called aclamshell incision.For most patients it can take about a year to be fullywell again.“The thoraflex graft is a revolutionary designcombining the best of open heart surgery techniquesand endovascular techniques. This novel hybrid surgeryenables a complete aortic arch replacement using amuch less invasive technique with quicker recovery andperhaps better outcomes,” says Dr. Chu.Indeed, Barbara had a remarkable recovery andreturned home after six days in hospital.“I felt better in about a month and resumed all myactivities,” says Barbara. “And you’re darned right that Iam swimming again. I’ve got to stay in shape.”Barbara is one of close to 50 patients who have had athoraflex graft at LHSC since 2014.LHSC is a North American leader in the hybrid archtechnique, treating patients from across Canada.“We were fortunate enough to be an early adopterof this novel approach for patients and have developedthe largest patient experience with this graft in Canada,”says Dr. Chu, who is seen as a pioneer in this field.“Early results have been really fabulous.”Dr. Chu and his team, meanwhile, have been trainingsurgeons from other hospitals around North America.Many have travelled to London to learn about theprocedure, while other surgeons have asked for consultson their cases.Not every patient with an aortic aneurysm is ableto have a thoraflex graft. It depends on the type ofaneurysm and its location within the aortic arch.LHSC has a world class team of cardiac and vascularsurgeons with expertise in advanced aortic surgery whoare able to provide patients with all the surgical options,including novel, cutting-edge techniques such as thethoraflex hybrid.Three years after her surgery, Barbara now has anannual appointment with Dr. Chu. Of her experienceshe recalls the calm way he laid out the informationabout her surgery and recovery.“Dr. Chu and his staff are very knowledgeable, verykind and very understanding,” says Barbara.Indeed she is back to her busy lifestyle, maintainingher own home, baking bread, doing yoga, keeping a biggarden, and canning what she has grown. She also playsbridge with her friends, helps around the farm, andmakes time to go to the cottage.“I didn’t change my life, I resumed everything Idid before but sometimes it takes a little longer,” saysBarbara. “My philosophy is, be thankful you survivedand move on.”Fast FactsAn aortic aneurysm is a balloon-like bulge in theaorta, the large artery that carries blood from theheart through the chest and torso.SymptomsMost people with aortic aneurysms do not showsigns or feel an aortic aneurysm. Usually, theaneurysms are found when tests, such as a CT scanor echocardiogram, are done for other reasons.In the rare cases people do report symptoms, theissues are often related to the aneurysm pushingagainst the: windpipe (trachea) causing trouble breathing,wheezing coughing or recurrent pneumonia nerve to the vocal cord (laryngeal nerve) causinga hoarse voice esophagus making it difficult to swallowThe symptoms may occur once in a while or stayconstant. Belly, chest or back pain is less commonbut may indicate an emergency. The feared result isa tear in the aortic wall or rupture, which can causesevere pain and internal bleeding, and can leadquickly to death.Risk FactorsDiseases that damage your heart and blood vesselsalso increase your risk for aortic aneurysm. Thesediseases include high blood pressure high cholesterol atherosclerosis (hardened arteries) smokingA family history of aortic aneurysms can also increaseyour risk.Sources: National Center for Chronic DiseasePrevention and Health Promotion and American Collegeof Cardiology.ONLINE EXCLUSIVELHSCsurgeonsexplainprocedureLHSC cardiovascular and thoracic surgeonDr. Michael Chu and his team are leaders inthe use of the thoraflex graft for complex surgeryand have been training surgeons from otherhospitals around North America.Visit us at inside.lhsc.on.caBarbara Palmateer had a remarkable recovery from complex aortic surgery and returned home after six days in hospital.0607
IN dAArichFortyyearsStillera teamof arsago,ago,Dr. Dr.CalCalStillerandanda teamof t atUniversityHospitalwereof thein theworldto conducta reoneoneof thefirstfirstin theworldto conducta losporinetrialsbegan,physiciansfounda significantdecreasein organJustJust14 ansfounda significantdecreasein organrejection.successin kidneytransplantsjumpedfromcentto 80centsurvivalyearrejection.TheThesuccessin kidneytransplantsjumpedfrom50 50perpercentto recipientssurvivedandandthrived.forwardto 2019LHSCcelebratedits 6,000thtransplant.FastFastforwardto 2019andandLHSChashascelebratedits 6,000thtransplant.landscapeof wableto transplantsomeTheThelandscapeof ��renowableto transplantsomeorgansor partialorgansfromlivingdonors.definitionof deathdonationevolved.And,organsor partialorgansfromlivingdonors.TheThedefinitionof deathandanddonationhashasevolved.And,researchis leadinga is leadingus usto atofuturewhereorgandonationmaybecomeobsolete.Mahms Mohamed is a transplant donor specialist with the LHSC Multi-Organ Transplant Program.080909
IN FOCUSSurgeons Dr. Alp Sener and Dr. Patrick Luke are able to remove a healthy kidney from a living donor through a single, tiny incision using a robotic surgical system.Where we are nowThe past years have seen the continuation of significantadvancements in transplantation including organs from aliving donor.The ability to transplant kidneys and partial livers from livingdonors has led to an increase in the number of transplantsat LHSC.“The laparoscopic retrieval of kidney donor organs has beena tremendous benefit for living donors. We are able to removekidneys from living donors through a small incision,” says Dr.Anthony Jevnikar, Co-director of the LHSC Multi-OrganTransplant Program. “It is an altruistic decision to donate akidney. In the past it sometimes took longer for the donorthan the recipient to get back on their feet after surgery, so thelaparoscopic process has provided for an easier healing process.”There was a time when living donors had to be familymembers who were an appropriate match to donate a kidney orpartial liver. But this is no longer a restriction.Canadian Blood Services offers a Kidney Paired DonationProgram for potential donors who are not compatible with theintended recipient, says explains Corinne Weernink, a longtimetransplant donor coordinator with LHSC and now the qualityand safety specialist with the transplant team.The national program provides individuals an opportunity tobecome a living donor and donate a kidney to someone in needand, in doing so, provide transplant candidates an increasedopportunity to receive a transplant.“Five years ago our living donor kidney program had about20 transplants. Last year we had more than 40 living donortransplants,” says Weernink.Before donating, the potential donor must undergo anassessment, which usually takes about three to six months for allthe test results to become available.Because there is the potential risk of disease transmissionfrom the donor to the recipient, the assessment includesa detailed questionnaire, medical history, physical exam,and blood tests.Potential donors need to meet with the Living DonationTeam including a donation coordinator, social worker, surgeon,and nephrologist. The team wants to ensure that the livingdonor's own health is protected.The process is similar for living donors giving a portion oftheir liver for transplant but includes more rigorous testing. Thebest candidates for living liver donation are family membersand close personal friends of the recipient. Anonymous livingdonors may also be considered.Living donors should meet these criteria: be in excellent physical and psychological health be between the ages of 18-55 years old have a compatible blood type with the recipient come forward to donate voluntarily be a healthy weight and about the same physical size (orlarger) have no history of long-term (chronic) illness such ascancer, diabetes or heart diseaseThe potential donor will undergo a series of complextests to ensure that the liver is working well. These include anultrasound, echocardiogram, stress test, and different typesof scans to determine the liver's size and shape as well as thecondition of the bile ducts.Throughout the process potential donors are informed aboutthe risks and can choose to decline at any point before surgery.For some patients, receiving a new organ transplant has towait because they are just too sick to undergo transplant surgery.Patients waiting for a new heart may need a device that canhelp support them until they are well enough for surgery.Short-term ventricular assist devices (VADs) can be atemporary ‘bridge’ to maintain the heart and improve thefunction of other organs.“The device is used in two different scenarios. First, it maybe used as a bridge to transplant or secondly, as a destination,an external support for the heart,” says Weernink.These bridge devices enable patients to recover and waituntil a donated heart becomes available. And while some havereceived a heart transplant, others have recovered enough to nolonger need a transplant.With more than 700 transplants over the past 30-plus yearsLHSC has performed among the highest number of hearttransplants in Canada.First liver transplantin Ontario10101979UH chosen as oneof the first centresworldwide to begin aclinical study on newanti-rejection drug,cyclosporine1981First heart transplantin Ontarioare at the forefront of studying different molecules to protectorgans during the storage period, adding molecules to thepreservation solution to prolong organ storage without risk oftissue injury. For details on this groundbreaking research see theSummer 2018 edition of Inside LHSC at inside.lhsc.on.ca.Other research ahead will address ways to influence thebody’s immune system so that there is less likelihood of organrejection. While cyclosporine and similar drugs are highlyeffective in reducing acute rejection in the short term, there canbe potential adverse side effects over the long term.“We are looking at clinical research strategies where patientsare temporarily on anti-rejection drugs, and then weanedoff. We are currently looking at the best approach to applythis research to patients,” says Dr. Jevnikar. “We recognizethat patients are the real pioneers in achieving what we do intransplantation. It is their bravery and trust in us that keepsadvancements in patient care going.”Another area of research in the coming years, one that couldrevolutionize the entire focus of transplantation, will be therepair and regeneration of organs.However far into the future this seems, Dr. Jevnikarpredicts that in 40 years or so the word transplantation willgo into disuse.“So when we explain to our great-great-grandchildrenwhy we did organ transplants, we’ll say we didn’t have anyother options at the time,” says Dr. Jevnikar. “Instead we’ll berehabilitating and refurbishing damaged organs, or perhaps evencreating new organs, so they’ll work in patients in need.”“We have always thought beyond transplantation. Our goalis to cure patients and transplantation is the tool we have athand now. In the future I hope we will be able to do betterthan transplantation.”Donation after deathDonation after circulatory death (DCD) is arecent approach to increase the number oforgans available for transplantation.Some patients who cannot survive willhave life support withdrawn as part ofcompassionate, end-of-life care, and in somecircumstances their organs can be donatedafter death.LHSC is one of the leaders in North Americain donation after circulatory death andthe results of the transplants have beenvery good with recipient survival ratesapproaching 90 per cent.The families of the donors have consistentlyexpressed gratitude that donation waspossible and the wishes of the deceasedwere honoured.Since our first kidney transplant in 1973,more than 6,000 transplants have beendone at LHSC: kidney – 2,905(includes deceased and living donors) liver – 2,133(includes deceased and living donors) heart – 698 kidney-pancreas – 103 pantas – 7 liver-kidney – 36 liver-heart – 2 liver-bowel – 12 bowel – 11 lung – 48 heart-lung – 47 multi-visceral – 4Forward thinking, future thinkingPreviously, the Multi-Organ TransplantProgram performed lung, heart-lung, andbowel transplants. Although LHSC no longerprovides these types of transplants,the information is provided here as acumulative list of the total transplants done.At a Canadian National Transplant Research workshop,Dr. Jevnikar recalls a donor mother and recipient son talkingabout their experience.Dr. Patrick Luke, left, and Dr. Anthony Jevnikar, Co-directors of the Multi-Organ Transplant Program at LHSC.Historical Highlights1977After their talk, they were asked what they thought should bedone to improve transplantation. The mother suggested thatclinicians and researchers figure out what caused the disease inthe first place in order to avoid transplantation altogether.“That was a great moment that turned on lights for many.Patients spend a lot of time thinking about their conditionobviously, and often provide us with forward thinking futurethinking on how we might make transplantation better,” saysDr. Jevnikar.This kind of forward thinking is apparent in the recent abilityto use the organs of donors with hepatitis C.“If someone with hepatitis C received a liver transplant,they’d often end up with hepatitis C recurring in the liver. Nowwe have very effective anti-viral drugs that patients can takefor hepatitis C that can cure those patients. Amazing to seehow this has changed the face of liver transplantation,” saysDr. Patrick Luke, Co-director of the Multi-Organ TransplantProgram.“This has also opened up an opportunity for us to use donororgans with hepatitis C for transplant as the recipient canreceive a lifesaving and excellent organ and then can have thehepatitis C eradicated. LHSC was among the first in Canada todo this with kidneys, and it has certainly increased the numberof donor organs.”Giving patients the best chance of living with a new organ isalso about providing the best functioning organ. Eliminating theimpact of storage time between donation and transplantation isan important component of that.“With new preservation techniques we can transfer organssuch as liver, heart and kidney, to transplant centres in otherparts of the country. However, there are limitations in terms oftime between donation and transplantation,” says Dr. Luke.Researchers at Lawson Health Research Institute in London1983Canada's first heartlung transplant1983First pediatric hearttransplant in Ontario1984First pediatric liver
LHSC's Bariatric Centre of Excellence offers a rigorous, full-service bariatric surgery program. 06Treating deadly aneurysms with thoraflex graft leads to quicker recovery Barbara Palmateer had a remarkable recovery from complex aortic surgery and was back to her routine after one month. Recovery from conventional complex aortic surgery can take