Transcription
AMERICAN HEALTH NETWORKEYE SPECIALISTerfnfDerenuLa
In acknowledgement of Sandy Dilts, the executivedirector of the Muncie Eye Center for her time,consideration, and guidance through this design.1
TABLE OF CONTENTSECTION ONE: IntroductionAHN Philosophy Overview Design Solution.3Methodology End Users .4Survey Analysis.5Issues Goals Performance Requirements.6SECTION TWO: Historical, Observational, Interactive ResearchIntroduction: Research of the topic.7Observational Research Behavioral Mapping One.8-9Observational Research Behavioral Mapping Two.10-11Literature Reviews Summary of the Finding.12-14SECTION THREE: Building Site AnalysisOverview of the State and City.15Site Orientation Exterior Building Relationship to Interior.16Space Allocation Analysis of Site Space.17SECTION FOUR: Precedent StudiesEye Center Precedent Studies.18-21Analysis of Precedent Findings.22SECTION FIVE: The ProgramCriteria Matrix.23-25Existing Square Footages.26Bubble Diagrams.27Prototype Drawings.28-35SECTION SIX: ConclusionLimitations Material Proposal.36Finding Budget.37Solution Analysis.38Summary of Dates.39APPENDIX A: Bibliography.40APPENDIX B: Floor Plan Reflected Ceiling Plan.41-42APPENDIX C: Surveys - Administration.43-46APPENDIX D: Surveys - Nurses Doctors.47-49APPENDIX E: Surveys - Patients.50-52APPENDIX F: Photos.53-542
AHN MISSION STATEMENTAmerican Health Network eye specialists are a group ofdedicated professionals working together to provide thehighest level of care to enhance your quality of life. We takepride in placing great value on our patient’s overall healthand wellbeing. We have established a solid foundation withinour eye care professional community and by working inconjunction with primary care physicians. This allows us toprovide our patients with comprehensive medical eye carewhile still maintaining a focus on your entire systemic health.OVERVIEWAmerican Health Network is a health care system of physician and medicalpractices in both Indiana and Ohio. Within their many specialties, eye care isthe focus of the center. American Heath Network eye specialists offer threeconvenient locations in Muncie, Marion, and Kokomo, Indiana. Sandy Dilts is theexecutive director that heads each one of the three American Health Networkeye care centers. 200 North Tillotson Muncie, IN is the eye care center in whichwas chosen to be reevaluated and retrofitted to benefit its current users. Theseclients are served by a number of different doctors, specialists, and nurses. Tothe right are the eye care physicians. The importance of evaluating and supplyinga eye center that meets the community needs and citizens that will use the center.DESIGN MISSION STATEMENTMy vision as lead designer is to redesign the Muncie locationEye center inexpensively through sustainable design solutions.Providing a clean and comfortable place for both clientsand staff to work effectively and efficiently through flexiblespaces that are navigated through proper way finding tosatisfy the needs and safety of the end users. The aestheticdesign will be updated to reflect a clear contemporary visionthat will not hinder the patients’ current visual condition.DOCTORSDr. Thomas J. ChowattukunnelSPECIALTY: Cataract Surgery, General OphthalmologyLOCATION: MarionDr. Michael J. HodkinSPECIALTY: Cataract, Cornea, and Refractive SurgeryLOCATION Kokomo, MuncieDr. Michael J. ScanameoSPEICALTY: Cataract, Glaucoma and Refractive Surgery,Refractive Cataract SurgeryLOCATION: Kokomo, Marion, MuncieDr. Rita K. SinghSPECIALTY: Retina, Macula and Vitreous Diseases &Surgery, Macular Degeneration, Diabetic Retinopathy,Retinal SurgeryLOCATION: Kokomo, Marion, MuncieDr. Karen S. SkurnerSPECIALTY: Glaucoma, Eye Diseases, Pre- and Post-opCare, Elderly Patient CareLOCATION: Kokomo, MarionDr. James B. StewartSPECIALTY: Ocular Disease, Glaucoma, MedicalGlaucoma ManagementLOCATION: MuncieDr. Sewit AmdeSPECIALTY: Breast Reconstruction, Reduction,Augmentation; Microsurgery. Hand and lower extremityreconstruction; carpal tunnel and other basic handsurgery, Facial reconstructive and aesthetic surgery.Facial reconstructive and aesthetic surgery. Facialreconstructive and aesthetic surgery; Abdominoplasty,liposuction, body contouring; Skin cancer; complexwound coverageLOCATION: Kokomo, Marion, Muncie3
METHODOLOGYThere are several different types of people that use the Muncie Eye center from week to week. Each one of these users mustbe shown as a client having separate needs for this space. It is hard to say who is the most important end user of the facilitytherefore all of them need to be evaluated and accounted for. Surveys shown in the appendices were given out to each one of thethree end users to evaluated their opinions on the issues and needs of the new facility. Information provided in Appendix 1. The mostimportant need that was translated to us by Sandy Dilts was speeding up the amount of time clients spend in the eye center. Thefast the clients get in and out of the eye center, the sooner their doctors and nurses can attend to another patient. Inefficiency ofthe facility and also way finding makes this an issue in the upcoming design process. September 2012 was the first time in which wevisited the Muncie location in order to access the building layout. A second trip in September was made to the Marion location whichwas more recently designed in order to access their functions and aesthetic value in comparison to the Muncie location. It has beenexpressed that they want the center to look aesthetically like the Marion location. Two observational studies in October were conductedto watch the interaction between the staff and patients as well as their role in the center. Below is the three types of end usersthat have been researched and observed to adapt to their needs within the space to better design an adaptable space for all three.END USERS1Doctors are an important aspect of thiscenter because without them, there wouldbe no patients or need for people to enterthe Eye care Center. There are two types ofdoctors, ones who work specificallyto the Muncie location, and those who workat several AHN locations. These two types ofdoctor end users spend a different amountof time in the Muncie facility and will haveNursesdifferent needs of the space.also fall into the category of end usersand some work more hours then others.Differentiating the needs that doctors versusnurses will have is something that needs tobe researched to make a space where bothcoincide.2 administrative staff 3Thealso play a significant role as another enduser of this space. From the reception desk,to accounting, and secretarial position allfall under this category. And even thoughthese workers are not always meeting withthe clients the efficiency of everyone’sstay at the eye center relies on theirability to do their job correctly and ina timely manner. Therefore organizationand easy access is important to theseusers.The ultimate end users are the AHNclients that come to the Muncie locationfor eye care treatment. This includes firstclientsand revisiting or activetimeclients. This age range and demographicsof this client base is wide and will servea number of wants and needs that theMuncie Eye Center must meet to keeptheir sales client base at the same rateor efficiently higher.Clients and theirfriends and family must have a place thatis welcoming to enter and easy to navigatethrough making their experience not onlybeneficial but also enjoyable.4
administrative staffAccording to Appendix C surveys, it seems that all the recipients agreed that privacy is the main issue within the center and during their scheduled hours. Computer screen visibility is open for many to view and should be private patient information. Phoneconversations tend to be heard or disrupted by the lack of acoustics within their areas of work. However, all of the answers weregeneral and there were some issues that they do not realize what designers can do such as evaluate adequate lighting levels.I propose different layouts of work stations to ensure that there is no visual availablity to anyone other than thestaff at their computer desik.Also, acoustical paneling systems and other forms need to be researched to muffle sounds of conversation between staff and patients in person and also over the phone to provide efficiency.doctors/nursesDue to the fact that only one doctor/nurse staff replied to the survey doesn’t give a proper and adequate means of evaluation.Most of the answers were left unanswered on the surveys in Appendix D. However, carpeting and lighting issues were two thingsthat were stated as current design issues. The idea of an updated dilating room as well as a purpose for the centerpiece structurewas mentioned as needed area that I have already decided to achieve with this project, so the reassurance is good feedback.Lighting levels and the type of lighting must be changed within all parts of the center. Dimmers can be incorporatedwith more white light used for reading and work areas for the staff. I have kept in mind that the patients eyes will beextremely sensitives to the lighting levels. I plan to convert the centerpiece in the waiting room into a coffe/vending machine area to bring in more revenue for the eye center as well as privude interaction which the customers are waiting.patientsThere was a great range of answers from the patients which made the survey worthwhile but in also more difficult to evaluatedue to the fact that some of the answers were contradictory. Television and magazine material was not adequate according tothe clients, which does not apply to my position as a designer. The lighting levels, and interior design was shown as adequateas well as being less than adequate. Privacy seems to be an issue for patients as well staff voiced through Appendix E, statedthat the waiting chairs were too close to other patients.Some of their issues do not relate to interior design, or problems that I can fix, however lighting levels, and updated designasthetic, and color scheme can and will be implemented. Privacy is a clear issue throughout the space and will be taken careof to fit the comfortability and need of admin. staff and patients. Seating needs to be rearranged in another layout for traveling andwayfinding as well as accessible areas for patients in wheelchairs to make them feel comfortable among the other patients waiting.SURVEY ANALYSIS5
ISSUEEFFICIENCYCIRCULATIONCOMFORTGOALTime within the center needs to be cut down for patients anddoctorswhich can be achieved by reaching efficiency within the centerWith the clients disadvantge with seeing, wayfinding must be easilydeteremined in traffic flow to allow for a stress‐free and enjoyableenviornmentProviding a comforatable waiting area will allow the clients to feel athome and enjoy their time spent in the centerIt is important to keep the clients safe for legal reasons and to makethem feel secure in their surrounding especially while they are at adisadvantge with their eyesite.PERFORMANCE REQUIREMENTtime efficency wil improve with wayfinding,orientation of layout, and multi‐functionalspaceswayfinding and clear traffic flow, as well ascarpet distinction and signagethe new image will be comfortable modernand clean. Furniture and aesthetic featuresMinimizing obstructions in walkways, meetingSAFETYADA and IBC codesmulti‐functional desk systems as well asAllowing spaces and rooms to be flexible for several doctors and nurses storage and location of equipment. Find a usefor the center structure in the waiting area.to useFLEXIBILITYAllowing for an open floor plan while keeping the staff and patientsPartition walls, layout of desk space in relationpersonal information private from other cleints.to travel pathsPRIVACYMaking sure the clients are able to read the signage as well as hear thenurses when their name is called will benefit efficiency within thecenter. With the lack of sight, the other four senses will be heightened,lighting levels minimum, wayfinding throughconscious awareness of making them comfortable and notsignage, speaker system for name callingSENSORYoverwhelmed.DURABILITY/allowing the materials used within the space to hold up in quality andusing long lasting materials, life cycle costSUSTAINABILITY durability for many years to comeEnhancing the outdated image of the eye center will draw newEliminate 80's color scheme andcustomers and provide a new aestheticfurniture,eliminate some glass block,IMAGEECONOMYMinimal construction and material costReuse6
Historical Observation was found through literature reviews and internetsources through the study of Eye Centers and building codes that will meetthe requirements of the future design. Observations were made throughvisiting the site on several occasions to watch the users of the spaceinteract between each other and wayfind through the interior. This was donetwice through observational notes and behavioral mapping. Surveys weregiven out to the three groups of end users; doctors/nurses, administrativestaff, and patients. This information was also considered by indirectobservation of open ended survey questions to a random selection of users.7
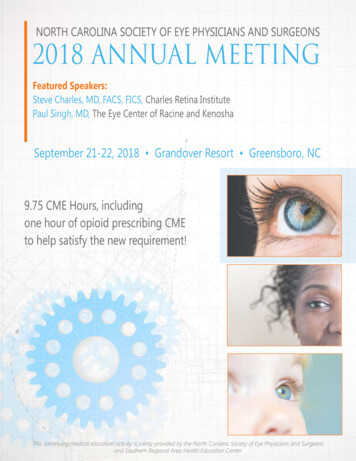
SEPTEMBER 25TH: 4 PM- 5PMCRITERIA1 SIGHT2 SOUND3 SMELL4 TOUCHCOMFORT5 ISSUE6 CIRCULATIONAVAILABLE7 SEATINGAVAILABLE8 WATER9 RESTROOMSOBSERVATIONdoctors office was open, his work and computer screen wasfacing the waiting room, due to the bad lighting inside theoffice. Also gloomy evening made for adequate everydaylighting. Lighting was yellow/orange tint in offices. Small 81/2 x 11 piece of paper with 14pt font to direct customersupstairs for dermotology does not show good wayfindingthe space is very open therefore you can hear people in thepods, on the phone, and in the checkout area. Also heardconversations of the patients and the nurses gossiping inbetween lanes.Couldn’t tell if smell was bad or good, however it wasn’tsmelling fresh or clean which I had hoped forwaiting chairs material is sufficient, bench seating wasslouching structure, chairs in lanes were more comfortable totouch. When leaving the doors are hard to open but then areon an automatic open, which is confusing.chairs, color of skylights has the appearance of dirty andunclean. Temperature was warm, fans were not on. Thebland colors are not welcoming nor having a sense ofcleaninessnurses were walking straight through patient waiting areas tocross pods, no direct path of travelSUGGESTED CHANGESpartitions need to beconstructed throughout thespace to close off private topublic zones. Lighting fixturesmust be replaces with clearnwhite lighting with highefficency bulbsREASON FOR CHANGEinefficent lightinglevels, privacy invadedaccoustical properties need tobe installed in finishes andstructural elementsnatural cleaning products andexamine toxin levels, add greenwallenhance indoor airqualityupdate textures/materialsoutdatedbuy new chairs, provideergonomic lumbar supportredesign layout of lobby andprovide signageelimate seating and rearrangeSince the center was near closing, plenty of seating was open. layoutprovide a café station that ismore accessible and distinct forWater jug as well as coffee counter was available.use of clients.Not ADA compliant. Clean and fresh smelling. Soapremove a stall to expland onedispensers‐ one automatic, one push?into ADA stallprivacy invaded,distraction occursuncomfortablebadwayfinding/circulationtoo many seatsADA code8
9
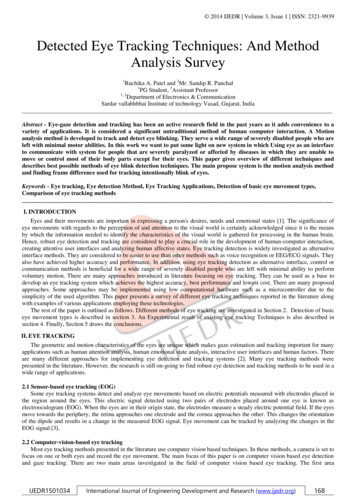
SEPTEMBER 26TH: 12AM-1PMCRITERIA1 SIGHT2 SOUND3 SMELL4 TOUCHCOMFORT5 ISSUE6 CIRCULATIONAVAILABLE7 SEATINGAVAILABLE8 WATER9 RESTROOMSOBSERVATION TWO1. small outdoor signage! 2.random placement of brochuresthat are used by nurses spread throughout the lobby. 3.Dilated patient was walking around the lobby. 4. Lobby wasoverly lit. 5.centers of the two lobby areas were virtuallyuntouched1. could potentially be very loud for the dilated patients. 2.Could hear sales rep talking to the doctor in the open lanesn/an/aSUGGESTED CHANGESplace a larger sign for the facilityoutside, put all brochures in asingle area, provide a dilatingroom, change the material ofthe glass wall.provide a dilating room, use ofconference roomREASON FOR CHANGEto allow for easywayfinding, control ofpatients, andsensitivity to theireyes.1. door entrance difficulty with entering patients.1. Patient was walking around the lobby for 10 minutes lost,nurse had to come out of one of the lanes to see what sheneeded1. Morning session still had plent of available seating forpatients and their guests.1. small sign on the coffe/water station that pateitntspreparing for surgery are not allowed to have liquidsn/afully automatic sensorsto eliminate confusionprovide distinct lobby areasto eliminate confusionto provide more spacein other areaseliminate some lobby seatingseclude this section, or havesomeone monitor itprivacysafety of patients10
11
1literature reviewsCama, R. (2009). Evidence-based healthcare design. Hoboken, N.J.: John Wiley & Sons.Understanding the shift toward evidence-based design in healthcare -- Step 1 : gather qualitative and quantitative intelligence-- Step 2 : mapping strategic, cultural, and research goals -- Step 3 : hypothesize outcomes, innovate, and implementtranslational design -- Step 4 : measure and share outcomes -- Evidence-based design in practice -- Growth opportunitiesfor the design professional. I hope to use these steps to support my design decisions by referencing how to support myevidence to the client to fit her needs in the best way.2Kachur, M., Bruck, D., & Hesedahi, J. (2010). Acoustical materials for a green world: The sustainable designtransformation of the architectural acoustics industry. Journal of the Acoustical Society of America, 127(3), 17231723. Retrieved September 23, 2012, from 723 s1?bypassSSO 1The focus on sustainable and healthy building materials has intensified over the last few years. This is true particularly inhealthcare, educational, and environmentally friendly or “green,” facilities, where an increasing awareness of acoustics hasresulted in a higher demand for innovative products. As the healthcare industry pushes for greater patient comfort, increasedspeech privacy, and green design, new acoustical products must satisfy multiple requirements. In educational facilities, the U.S.Green Building Council’s Leadership in Energy and Environmental Design (LEED) for Schools rating system promotes the useof green products, which extends to acoustical materials. Additionally, some educational facility owners are hesitant to allowtraditional types of sound absorbers such as fiberglass duct liner for fear of health issues. Consequently, acoustical materialsmanufacturers have responded with new and repurposed materials to suit these needs. Because many of these materialshave been recently introduced, a significant amount of project time can be expended on research to select an appropriatematerial to suit the new requirements. In an attempt to streamline the selection process, this overview will identify a numberof these new and repurposed materials and provide feedback on their use from architects, engineers, and owners.3ADA Home Page - ada.gov - Information and Technical Assistance on the Americans with Disabilities Act. (n.d.).ADA Home Page - ada.gov - Information and Technical Assistance on the Americans with Disabilities Act. RetrievedSeptember 25, 2012, from http://www.ada.gov/Updated American Disability Act rules and regulations related to users within the space.Susan, S. (2011, May 10). Point of View.Metropolis, --, --. Retrieved September 25, 2012, from stions and Answers about several Healthcare facilities12
4Sweets catalog file 2010: architects, engineers & contractors. (2010). New York: McGraw-Hill.v. 1. General requirements, Concrete, Masonry, Metals, Wood, Plastics, and composites, Thermal and moisture protection --v.2. Thermal and moisture protection, Openings --v. 3. Finishes, Specialties --v. 4. Equipment, Furnishings, Special construction,Conveying equpment, Plumbing, Heating, ventilating and air conditionsing (HVAC), Electrical, Communications, Electronic safetyand security, Exterior improvements --v.5 Directory --v. 6. Desktop index.5Harmon, S. K., & Kennon, K. E. (2011). Study guide for The codes guidebook for interiors, fifth edition. Hoboken,N.J.: Wiley.The Codes Guidebook for Interiors, Fifth Edition features jargon-free explanations of all the codes and standards of concern todesigners and architects, including performance codes, fire codes, building and finish standards, energy codes, and Americanswith Disabilities standards6Healthcare Design Magazine: Architecture and Interior Design Trends for Healthcare Facilities . Designing for Morethen Meets the Eye. Healthcare Design Magazine: Architecture and Interior Design Trends for Healthcare Facilities. Retrieved September 25, 2012, from signing-more-meets-eyeAtlanta-based LeVino Jones Medical Interiors, Inc., was commissioned by separate clients to design three new eye centerswithin the last year. While each client was expectedly unique in their program and services, these established practicesall shared three of the same reasons for building new centers: expansion of services and product, advanced technology/equipment integration, and an interest in exceeding patient experience expectations. This article studies the impact of thesedrivers in three different clinics and the resulting design7Lockton, D. (2008). Making the user more efficient: Design for sustainable behavior. Academia Education, Thesis, 1-9.User behavior is a significant determinant of a product’s environmental impact; while engineering advances permit increasedefficiency of product operation, the user’s decisions and habits ultimately have a major effect on the energy or other resourcesused by the product. There is thus a need to change users’ behavior. Arrange of design techniques developed in diversecontexts suggest opportunities for engineers, designers and other stakeholders working in the field of sustainable innovationto affect users’ behavior at the point of interaction with the product or system, in effect ‘making the user more efficient’.Approaches to changing users’ behavior from a number of fields are reviewed and discussed, including: strategic design ofaffordances and behavior-shaping constraints to control or affect energy-or other resource-using interactions; the use ofdifferent kinds of feedback and persuasive technology techniques to encourage or guide users to reduce their environmentalimpact; and context-based systems which use feedback to adjust their behavior to run at optimum efficiency andreduce the opportunity for user-affected inefficiency. Ex: Sustainable engineering and Eco design field.13
8No, A. (2012). --. British Journal of Aesthetics, 52(4), 1000.Founded in 1960, the British Journal of Aesthetics is highly regarded as an international forum for debate in philosophicalaesthetics and the philosophy of art. The Journal is published to promote the study and discussion of philosophical questionsabout aesthetic experience and the arts.9Zachs, S. (2007, June 20). A Healthy Obsession. Metropolis, --, --. Retrieved September 24, 2012, from thy-obsessionWith its focus on the patient experience and fierce dedication to green materials, Guenther 5 looks to remake the hospitalparadigm.10Susan, S. (2011, May 10). Point of View.Metropolis, --, --. Retrieved September 25, 2012, from stions and Answers about several Healthcare facilities11Carol, T. (2008, March 1). Advances in Healthcare Design, Interiors & Sources. Retrieved September 24, 2012, ArticleID/5725/Default.aspxThe Scottish Rite and Egleston campuses of Children’s Healthcare of Atlanta offer prominent examples of another healthcareinstitution realizing the benefits of evidence-based design.12Rebecca, D. (May/June 2012). Demographically correct design. Medical Construction and Design Magazine. RetrievedSeptember 25, 2012, Healthcare Interiors, from http://modmag.comCreating the right ambiance is more than what meets the eye. Catering to all age group within a Healthcare facility, andthe importance directly related to Fairfax Surgery Center as well as competition among Healthcare. Culture, Age,experience and lifestyle demographics also effect the experience of the patient.14
statemuncie, indianaAs of 2011 more the 6,516,922 live within the Midwest city of Indiana, with the majority of the residents living inurban communities. Land area of the state stretching of 92 counties, is 45,867 square miles. The capital is Indianapolis,which is approximately 65 miles away from the design site of the Muncie Eye Center. Indiana’s 41 mile Lake Michiganwaterfront and means of iron, steel, oil, and agriculture was what made this state a booming area starting in the 19century. The state is the leader in agriculture with outputs in hogs, soybeans, wheat, oats, rye, tomatoes, onions, andpoultry. Most buildings limestone was quarried in Indiana. Indiana is recognized as the 19th state, 38th largest stateby area, and the 15th most populous of the 50 states. The state has a maximum dimension north to south of 250miles and a maximum east to west dimension of 145 miles. Located between Michigan by the north, Ohio on theeast, Illinois in the west, and the Ohio River separates Kentucky on the south. The typography of the land is flat dueto the effects of the glaciers. Lowland, and low plateau are the names of the two regions Indiana qualifies under.Indiana falls under the eastern time zone. Climate here is humid continental with cold winters, and hot summers. Thesouthern most part of the start is within the humid subtropical climate resulting in more rainfall then the rest, howeverdroughts do occur within the state. The majority of the state’s racial diversity is white with about 85%, followed by10% African American.The median age of Hoosiers is 37 years old. The largest ancestry reported within the stateis German reported through the U.S. National censuscityThe estimated population of Muncie, Indiana in 2011was 70,080 people. Most of the staff was femalewhich correlated with the ratio of male to femalecitizens within the city limits. Muncie is in the 10largest cities within the state, set in Delaware countyon the White River, around 1854.The city is in afertile agricultural area with dairying and soybean,fruit, corn, oat, and vegetable crops. Machinery,electronic equipment, plastics, glass, motor vehicleequipment, and metal goods are among the manymanufactures. Industrialization came after the discovery of natural gas 1886. 27 square miles makes up this city,while remaining the same averages in demographics as the state. In the past years the local economy has struggled,however the connection of growth is made through the relationship of hospitals, and the university, as well asthe closeness to major cities within the state.15
site orientationexterior buildingThe front entrance to the center is south facing witheasy access to the parking lot, staff parks in the rearof the building with a separated north entrance. Onthe west side of the structure these was the intendedentrance facing Tilliton Ave which has no pathway upto the doors, and has never been used as intendedby the architect. Entrances are not clearly markedfor
American Heath Network eye specialists offer three convenient locations in Muncie, Marion, and Kokomo, Indiana. Sandy Dilts is the executive director that heads each one of the three American Health Network eye care centers. 200 North Tillotson Muncie, IN is the eye care center in which