Transcription
CLINICAL PRACTICE GUIDEEye care of thecritically illDECEMBER 2021Intensive Care NSW
The information is not a substitute for healthcare providers’ professional judgement.Agency for Clinical Innovation1 Reserve Road St Leonards NSW 2065Locked Bag 2030, St Leonards NSW 1590T 61 2 9464 4666E aci‑info@health.nsw.gov.au www.aci.health.nsw.gov.auProduced by: Intensive Care NSWFurther copies of this publication can be obtained from the Agency for Clinical Innovationwebsite at www.aci.health.nsw.gov.auDisclaimer: Content within this publication was accurate at the time of publication.This work is copyright. It may be reproduced in whole or part for study or training purposessubject to the inclusion of an acknowledgment of the source. It may not be reproduced forcommercial usage or sale. Reproduction for purposes other than those indicated above,requires written permission from the Agency for Clinical Innovation.Preferred citation: NSW Agency for Clinical Innovation . Eye care of the critically ill: ClinicalPractice Guide. Sydney: ACI; 2021SHPN (ACI) 210611ISBN 978‑1‑76081‑832‑6Version: V1; ACI 3042 [12/21]Trim: ACI/D21/1046 State of New South Wales (NSW Agency for Clinical Innovation) 2021.Creative Commons Attribution No derivatives 4.0 licence.
Eye care of the critically ill: Clinical practice guide December 2021ContentsEye care of the critically ill – at a glance1Summary2Introduction3Anatomy of the eye4Eye care of the critically ill6Patient assessment7Interventions9Infection prevention13Clinical governance13Appendix 1: Identifying Lagopthalmos and Opthalmology Abnormalities14Appendix 2: Evidence review15Appendix 3: Evidence summary ncy for Clinical Innovation www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Eye care of the critically illAgency for Clinical Innovationd www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Eye care of the critically ill – at a glanceEye care is important for the effective clinical management of critically ill patients in intensivecare. Regular eye care can prevent dryness, damage to the eye, complications and infection.Delivering eye care for critically ill patientsComplete eye health assessment onadmission and at the beginning of each shift.Clinical governanceand infection controlprocesses apply acrossall clinical eye care.Intensive care medical staff should assess patient if there are signs of:Assessment infection red eye or general sepsis cornea is dull and cloudy or cornea haswhite lines or spots visible.If red eye is identified, with or without exudate: take bilateral swabs for culture refer to an ophalmologist.Document eye health assessment and eye care interventionsat least once per shift.Documentation Clean eyes regularly. Deliver eye drops. Administer eye ointment (lubricant) asrequired.If eyelid closure isn’t possible (lagopthalmos), eyelids should bemechanically closed.InterventionsMedical officers assess patient for iatrogenic opthalmic complications(minimum weekly in ICU patients admitted 7 days).Patient referred for specialist opthalmological consultation if: eyelid closure unsuccessful within 24 hours iatrogenic ophthalmic complicationsidentifiedAgency for Clinical Innovation1 patient response to treatmentis limited.www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021SummaryEye care is important for the effective clinicalmanagement of critically ill patients in intensive care.Clinical management of eye care forcritically ill patientsCritically ill patients may have compromised ocularmechanisms.1, 2 This can result in:Clinical assessment and intervention on admissionand at regular intervals is necessary for effectiveeye care for patients in ICU. dryness of the corneaRecommendations for delivering evidence-basedclinical eye care are outlined in this guide andsummarised in ‘Eye care of the critically ill – at aglance’. disruption to the corneal epithelial surface lining complications of corneal abrasion, erosion,infection, ulceration, scarring, rupture orblindness. 2, 3Infection preventionRegular eye care can reduce the risk of eyecomplications and infection.Clinicians should follow infection preventionprocesses when performing eye care, including:This clinical practice guide provides guidance toclinicians about how to maintain the eye health ofadults and children in intensive care units (ICUs)in NSW. donning appropriate personal protectiveequipment (PPE) adhering to the five moments of hand hygieneThe guide is a revision of Eye Care Clinical PracticeGuidelines, first released in 2014. 4 storing eye care equipment separately fromother patient hygiene equipment. Containersshould be cleaned regularly.Potential for eye complications incritically ill patientsClinical governanceCritically ill patients are at increased risk ofexperiencing eye complications due to:Clinical governance related to eye care shouldinclude: compromised immune response documentation processes for eye health andinterventions environmental factors exposure to pathogens competency assessment for ICU staff in thedelivery of eye care incomplete eye closure (lagophthalmos),leading to dryness, infection and damage tothe eyes.1, 5, 6Agency for Clinical Innovation review of adverse events and ICU consults andaudits of practice to monitor delivery of eye care.2 www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021IntroductionDevelopment of this guideEye care is important for the effective clinicalmanagement of critically ill patients in intensivecare, especially for those whose ocular protectivemechanisms may be compromised.1, 2The guide is a revision of the Eye Care ClinicalPractice Guidelines, published by the Agency forClinical Innovation (ACI) in 2014. 4 A GuidelineDevelopment Network (GDN) was formed inOctober 2020 to review the original guideline, withthe primary author undertaking a current literaturereview.Dryness of the cornea and disruption to the cornealepithelial surface lining may result in complicationsof corneal abrasion, erosion, infection, ulceration,scarring, rupture or blindness. 2, 3Critically ill patients are at increased risk forcomplications due to having a compromisedimmune response and being exposed toenvironmental factors and pathogens.1, 5, 6Additionally, for intensive care patients, incompleteeye closure (lagophthalmos) may make it moredifficult to determine if a patient has developediatrogenic ocular surface disease (OSD).7Provisional recommendations based on theavailable evidence were developed and revised bymembers of the GDN. The revised clinical practiceguide was sent to the GDN members for review.The guide narrative was revised based on groupfeedback.Recommendation agreement was achieved by GDNmembers assigning their level of agreement witheach recommendation statement. The level ofagreement is indicated in this guide for eachrecommendation. Further detail about this processis provided in Appendix 2.PurposeThis clinical practice guide was developed toprovide guidance to clinicians about the proceduresused to maintain and optimise the eye health ofpaediatric and adult critically ill patients in ICUsin NSW.More information about the author andmembership of the GDN can be found in theacknowledgements section of this guide.The recommendations are most relevant forpatients at increased risk for iatrogenicophthalmological complications due to acompromise in the level of consciousness orimpaired ability to control eye opening and closure.It is assumed that readers possess a workingknowledge of anatomy and physiology of the eye.How to use this guideThis guide includes recommendations and asummary of relevant literature. The detailedevidence used to support statements can be foundin the integrated evidence review (Appendix 3).Clinical judgement should be exercised whenapplying the principles and procedures outlined inthe guide. Where ophthalmic complications haveoccurred, the directions of the ophthalmologistshould be adhered to over the recommendationsoutlined in this document.Target cliniciansThis guide is for all intensive care clinicians who areresponsible for the care of patients where theprotection of the ocular surface cannot be achievedby independent complete eyelid closure. This guideis not intended to include the intensive care ofneonatal patients.Agency for Clinical Innovation3 www.aci.health.nsw.gov.au
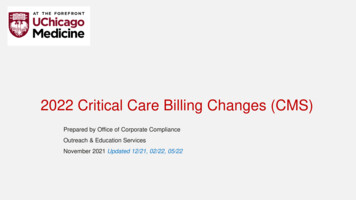
Eye care of the critically ill: Clinical practice guide December 2021Anatomy of the eyeSummary of normal anatomy and physiology of the anterior ocular surfaceThe ocular surface is protected from injury andinfection by several structures, including thefollowing (refer to Figure 1):The conjunctival epithelium extends from the eyelidmargins anteriorly, sharply turning on itself to coverthe sclera, creating a moist sac. This sac iscontinuous with the epithelium that lines the tearducts and plays a central role in the defence ofocular surface microbial injury. The conjunctiva hasa rich blood supply and, if damaged, redness andswelling may be present. Tissues may protrudebetween the eyelids, exacerbating the effects oflagophthalmos and resulting in corneal opacity andvision loss. 6 Retractable eyelids have a mucous membranecovering that is continuous with the eyeball, andepithelium of the sclera, cornea and conjunctiva.Eyelids mechanically protect the eyes fromdehydration and injury. 3 An opaque sclera ensures that light transmittedto the globe enters only through the transparentcorneal covering of the pupil. 3Functioning of the above structures and transparencyof the cornea are essential requirements for eyesurface protection and are vital for vision.2 Undernormal physiology, closure of the eyelids occurs,which is protective of the ocular surface – the blinkreflex and tear production are present and the scleraand cornea appear bright and clear.3 An avascular cornea functions to admit and refractlight. If injured, it may be slow to heal. Five layersof corneal tissue (superficially epithelium, changingto deeper endothelial tissue) provide a protectivebarrier against abrasion and erosion, and providea permeable barrier against eye pathogens.6Figure 1: Horizontal section of a schematic eyeSuperior rectus muscleVitreaous gel (body)IrisSceleraChoroidAnterior chamberOptic nerveCorneaPupilLensMaculaFoveaCiliary body and muscleRetinaRetinal arteries and veinsAgency for Clinical InnovationInferior rectus muscle4 www.aci.health.nsw.gov.au
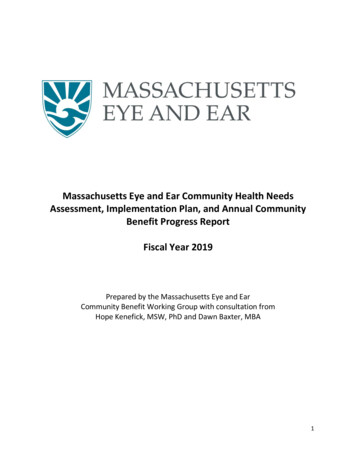
Eye care of the critically ill: Clinical practice guide December 2021Function of tears, blinking mechanism and frequencyEyelid closure and blinking provide a mechanicalbarrier to ocular injury. This prevents drying out anddesiccation of the corneal epithelium by distributingtear film across the exposed surface of the eye. 3, 6Normal blink frequency in the daytime is typically9-13 blinks per minute, increasing to 20-30 blinksper minute with abnormal sleep patterns(tiredness). This equates to typical interblinkintervals of between 4-6 seconds and 2-3 seconds,respectively.11Lacrimal gland production of tear film is needed forhealthy eye function. 8 Tear film containsbactericidal enzymes (lysozyme, lactoferrin) andproteins (IgA). 8 Tears help to provide a defenceagainst microbial colonisation by providing amedium for transport of leukocytes in the event ofeye injury or infection. 8 Any increase in irritationfrom the cornea or conjunctiva will trigger alacrimal reflex, resulting in an increased tearvolume for the eye. 9During cataract surgery, the eyelids are held apartby an eyelid speculum. Surface drying is visible andevident from a change in the normal light reflectionfrom the cornea where it becomes slightly hazy.Within about 20 seconds, the eye can be damagedwhen exposed or uncovered to air (refer to Figure 2).Blinking and tear production helps: smooth out corneal irregularities protect the air-corneal interface and refractivesurface of the cornea clear metabolic waste via nasolacrimal drainagemechanisms enable oxygen delivery to the cellsof an avascular cornea.10Figure 2: Visible corneal surface drying during cataract surgeryImage source: Taken by Dr Michael Hennessy, Ophthalmologist. Produced with his permission.Agency for Clinical Innovation5 www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Eye care of the critically illEpidemiology of ocular complications inthe critically illThe ICU is a pathogen-rich environment. This maycontribute to the increased exposure of the ocularsurface to microorganisms.12 Multi-resistantorganisms associated with microbial keratitisinclude pseudomonas aeruginosa, acinetobacter,staphylococcus epidermis, enterococcus,enterobacter proteus mirabilis and klebsiellapneumonae.1, 3Iatrogenic eye complications cover a range of OSDthat involve structures such as the cornea, scleraand conjunctiva. Pathologies may range frommicroepithelial corneal punctures (often associatedwith dry eye syndrome), to corneal abrasion,erosion, ulceration, infection and scarring. 3Eye care clinical practiceSuperficial keratopathy (any breach of the ocularsurface) in the ICU population has been found topredispose the patient to infection of the cornealepithelium (keratitis). 2, 3, 6 This infection may bemicrobial, bacterial or fungal in origin. 3 Keratitis inthe presence of corneal exposure is a key factor inthe development of OSD and has resulted in seriouscomplications, such as vision loss, corneal ruptureand the need for corneal transplantation.1, 3The provision of regular eye care as part of a carebundle has been found to prevent cornealabnormality, exposure keratopathy and infection inthe critically ill population.13-17 This has been found tobe true in both the adult and paediatric populations.When clinicians have received focused clinicaleducation on eye care in the critically ill and areincreasingly compliant with eye care guidelines, thishas led to reduced exposure to keratopathy forpatients.14, 15, 17Why critically ill patients are atincreased risk of ocular surfacedisordersAnecdotally, however, it has been reported thatpractice varies greatly between ICUs regarding thefrequency and method of eye care undertaken.Specific eye care practice has included the following:There are several causes of impaired ocular defencemechanisms in critically ill patients. These include: An alteration in the level of consciousness,impacting on the blink reflex and incomplete eyeclosure (lagopthalmos) (see Appendix 1) Regimens of cleaning the eyes with sterile wateror normal saline every two to four hours, twicedaily or daily16, 18, 19 Metabolic derangements Installation of a lubricating liquid, such asmethylcellulose eye drops18, 20 Immunosuppression Applying eye ointment for high-risk patients, orwhere evidence of eye injury may be apparent, suchas when conjunctival oedema is present5, 16, 19, 21-25 Mechanical ventilation Medications, such as sedatives and musclerelaxants Polyethylene film with artificial tear drops hasbeen shown to be more effective thanpolyethylene film on its own. 26 Paralysis Respiratory pathogens from open suctiontechniqueFor conditions of conjunctival or corneal exposure,methods such as passive eye closure, eye taping,padding with gel membranes, and creation ofmoisture closed chambers using polyethylene filmor goggles have been described.19, 21, 22, 25 16, 18, 19, 21-24 Systemic disease Prone positioning1, 3, 6Agency for Clinical Innovation6 www.aci.health.nsw.gov.au
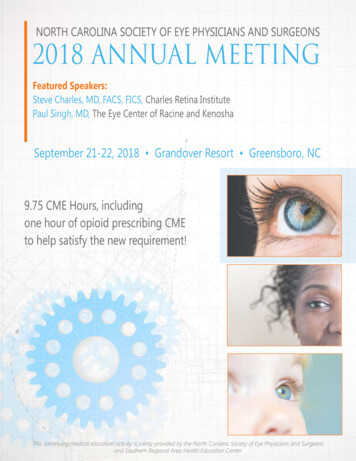
Eye care of the critically ill: Clinical practice guide December 2021Patient assessmentA comprehensive patient history and assessmentshould be completed on admission, and at regularintervals, such as at shift handover. 27, 28 Cliniciansshould be aware that critical illness, pre-existingconditions and intensive care treatment allcontribute to an increased risk of iatrogenic eyecomplications.Figure 3: Dry eye closedClinicians can do a corneal epithelial assessmentusing readily available practical methods. Thesemethods can include: a magnified view using fluorescein stain and ablue light (see Figure 3 and 4) using a direct ophthalmoscope (blue light andmagnification).Clinicians should approach family members forinformation regarding the patient’s medical andsurgical history. This history should include ocularconditions and treatment in order to assess therisks and assist with early recognition of OSD. 27The history should include:Figure 4: Dry eye open any previous eye injury or surgery the presence of an artificial lens a history of cataracts, glaucoma and otherpre-existing eye treatment and medications,such as anticholinergic drops whether the patient is known to wear contactlenses, in which case a thorough eyeexamination to locate and remove lenses shouldbe done to prevent corneal damage. 29, 30Source: Eye Care Emergency Manual, Agency for ClinicalInnovation [2009]12Early recognition of the signs and symptoms ofOSD, as well as the early treatment, improvesresolution of this condition. 3Agency for Clinical Innovation7 www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Table 1: Recommendation summary table –patient assessmentThe following steps should take place as part ofregular eye care for each critically ill patient:1. Patient assessed for risk factors for OSDand the ability to maintain eyelid closure onadmission, and routinely thereafter, such asat shift handover.Recommendation2. A bright light (using a pen torch) should be usedfor eye examination, looking for signs of infectionor disease, conjunctival swelling, dullness,cloudiness, whiteness or spotting of the cornea.Signs of infection may include redness, pain ordischarge, lid and conjunctival swelling withhyperaemia, lid margin crusting or cornealclouding.1, 3 Any new findings or suspicion ofinfection should trigger a medical review.Eye health assessment should be part ofroutine patient assessment practice andperformed on admission, as well as atthe beginning of each shift.GDNconsensusAdmission and ongoing assessmentshould include, but is not limited to thefollowing:GDNconsensus Risk factors for OSD Ability for patient to maintain completeeyelid closure Evaluation of eye and eyelidcleanliness3. If there is suspicion of infection, bilateral eyeswabs should be obtained for culture, as well asmedical consideration for ophthalmologicreferral. The use of a broad-spectrum antibiotic,in addition to chloramphenicol, should beconsidered until the result of the swabs becomeavailable. 3 Corneal dryness or discolouration Eye care interventions Effectiveness of eye care interventionsAn assessment by intensive care medicalstaff should be undertaken when thefollowing are found:4. If signs of infection do not improve within 48hours, intensive care medical staff must bealerted, and ophthalmic opinion must be sought. 3GDNconsensus Signs of infection Red eye or general sepsis5. Frequency of ocular assessment and eye careinterventions should be documented in a careplan that is regularly reviewed and updated.Results of patient assessment andeffectiveness of interventions should bedocumented at least once per shift. Cornea that is dull and cloudy, or withwhite lines or spots visibleWhere red eye is identified, with orwithout exudate, bilateral swabs forculture should be taken and anophthalmologist referral completed.Development of a red eye in a septic patient shouldbe addressed as an ocular emergency. Thepatient’s visual capacity may deteriorate withinhours, and may depend on rapid intervention.1, 3Where red eye is found, with or without exudate, aswab and culture of both eyes should routinely beundertaken and a medical review completed.Examples of abnormal findings during eyeassessment can be found in Appendix 1.Agency for Clinical InnovationSource8 GDNconsensuswww.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021InterventionsFigure 5: Grading lagopthalmosPatients with incomplete eye closure(lagopthalmos) are more likely to develop iatrogenicOSD.7, 15, 22, 28, 29, 31, 32 Critically ill patients maydevelop lagopthalmos due to:Grade 1: Eyes completely closed reduced level of consciousness tracheal intubation prolonged sedation paralysis prolonged mechanical ventilation positive end expiratory pressure (PEEP) medical conditions with significant metabolicderangement and positive fluid balances. 5, 6, 18, 22,Grade 2: Eyes open – Sclera or conjunctiva visible33-35Lagopthalmos exposes a patient’s eyes which canlead to: drying of the conjunctival and corneal epithelium infection corneal erosion permanent corneal scarring vision loss.1, 3Medical staff should identify and treat the causesof lagopthalmos early through regular eyelidassessment (Figure 5). If the eyes are unable to beclosed passively, then mechanically close theeyelids to protect the eyes.Grade 3: Eyes open – Cornea visibleSource: Eye Emergency Manual12Agency for Clinical Innovation9 www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Covering the eye to maintain cornealmoisturePolyethylene Eye CoversAs with tape, polyethylene eye covers should beplaced over eyelids that are correctly opposed(Figure 6b).Interventions to cover the eye and maintain cornealmoisture appear to reduce the incidence of eyecomplications in the adult population. 2, 5, 16, 19 Theseinterventions include the use of either passive ormechanical means to obtain complete lid closure. 2, 7,36There is limited evidence of effectiveness of theseinterventions in the paediatric population.Figure 6a Method of eyelid tapingMechanical eye covers have been advocated as astrategy to minimise the risk of eye infection in casesof respiratory infection where open tracheal suctiontechniques may be in use, and when patients requireprone positioning.6 These covers have beenadvocated for use in combination with eye ointment,paraffin gauze, dressing and tape.16, 26, 36TapeFigure 6b Polyethylene eye coversIt is important to ensure that the eyelids areopposed correctly so that the eye lashes are notable to scratch the eye (Figure 6a). 3 Note that whenremoving the tape placed on the eye, it is importantto pull the tape off medial to lateral, as the medialligaments are the strongest and are likely to sufferless lid trauma than pulling lateral to medially orsuperiorly to inferiorly. There is a risk of causinglevator aponeurosis dehiscence and subsequentptosis from pulling the tape off superior to inferior,particularly if the tape is being applied andremoved on a regular basis.Source: Figure 6a image courtesy Opthalmic services guidanceeye care in the intensive care unit . 3 Figure 6b image courtesy ofAmy Parkinson.Agency for Clinical Innovation10 www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Cleaning and treatment of the eyesProtective barriers and moisture for thecorneal surfaceAvailable evidence supports routine eye hygiene forall patients and eyelid cleansing if lids are unclean.1, 3, 6Eye cleaning with saline-soaked gauze every twoto four hours to remove exudate, debris or driedocular medications should occur in the critically illpopulation.7, 24, 37Various methods have been used to provideprotective barriers and moisture to the cornealsurface. However, evidence supporting practice hasbeen inconsistent due to variations in thedefinitions and methodologies used and should beviewed with caution.The use of normal saline over sterile water isdebated.7, 16, 19 However, agreement exists on theneed to promote patient comfort and healing byfrequently cleaning the eyes.The use of lubricants is supported in all unconsciousor heavily sedated patients, as lubricants decreasethe risk of corneal dehydration.7, 37 The use oflubricants in the adult population has beensupported to provide longer lasting eye moistureand require less frequent installation. 8, 25 Lubricantsare recommended for use in the paediatricpopulation for sedated ventilated children.13, 15When delivering treatment, if more than oneproduct is required, they should be applied in thefollowing order:1. Provide eye hygiene.2. Deliver eye drops.Lubricants are more effective than passive eyelidclosure in reducing the incidence of cornealerosion. 23, 25 However, lubricants are less effectivethan mechanical eye covers (except hydrogel eyepads) in reducing corneal breakdown. 21, 22Polyethylene cover moisture chambers have shownto be effective in reducing the incidence of exposurekeratopathy.16, 19, 233. Administer eye ointment (lubricant), if required,as it is water repellent and will prevent dropsfrom being absorbed. If lagopthalmos ispresent, gently close the eyes manually tospread treatment over the eye surface.1If administration of more than one type of eye dropis required, it is recommended these are spaced outas one drop may wash out another. Ideally, fiveminutes should be allowed between drops.1Agency for Clinical InnovationCombination use of 1.27cm lubricant ointment withpolyethylene covers has been shown to result in alow incidence of OSD (5.3%-6.8%).16, 25 A softadherent tape edging has also been used withpolyethylene covers to create a better seal in theadult population.16, 19 Extreme care should be takento prevent injury because the tissues surroundingthe eyes are delicate and inadvertent application oftape to the cornea may cause damage.111 www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Table 2: Recommendation summary table – interventionsRecommendationSourceEyelid closure should be used to protect the eyesof critically ill patients who are unable toindependently maintain complete lid closure.GDNconsensusAll patients should receive regular eye cleaning toremove debris, secretions, dried ointment and otherocular medications.GDNconsensusFor all patients with, or at risk of, lagopthalmos,second hourly eye care must be undertaken toprevent drying of ocular epithelial surfaces andreduce the risk of infection.GDNconsensusIf eyelid closure cannot be maintained passivelythen mechanical taping methods should be used toclose the eye.GDNconsensusIf eye infection is suspected, consideration shouldbe given to commencing broad-spectrum topicalantibiotic treatment until the result of swabs areavailable.GDNconsensusClinicians should ensure that patient’s eyes are notexposed to aerosols generated during tracheal ororopharyngeal suction procedures.GDNconsensusMedical officers should assess the patient foriatrogenic ophthalmologic complications (at themicroepithelial level) at least weekly in intensivecare patients with a length of stay greater thanseven days, using readily available practicalmethods.GDNconsensusPatients should be referred for specialistophthalmological consultation when any of thebelow occur:GDNconsensus Clinical practices fail to achieve sustained eyelidclosure within 24 hours Iatrogenic ophthalmologic complications areidentified Patient response to treatment is limitedAgency for Clinical Innovation12 www.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Infection preventionClinical governanceThe Australian Guidelines for the Prevention andControl of Infection in Health Care and the NSWInfection Control Policy (PD2017 013) state that allprocedures which generate, or have the potential togenerate, secretions require either a face shield or amask with protective goggles to be worn. 38-39Eye care interventions should be included in acomprehensive patient care plan that is regularlyreviewed and updated. This approach facilitatesawareness of changes to the patient’s condition, eyecare treatment and recorded outcomes.7 Standingorders may be useful in ensuring timely intervention,such as the initiation of ocular antibiotics whereinfection is suspected.The use of personal protective equipment (PPE) toprevent mucosal or conjunctival splash injury ismandatory while using open or closed suction of apatient. This must include goggles or face shield,gloves, and gown or apron.Contemporaneous documentation of patient eyestatus (and treatment) – recorded each shift as aminimum – may be aided by using a tick boxchecklist tool for attachment to either a paper flowchart or electronic medical record entry.Eye care equipment should be kept in containersseparate from other hygiene equipment. Additionally,medications including eye lubricants must be forsingle patient use only and be stored and disposed ofas indicated by the manufacturer.Table 4: Recommendation summary table –clinical governanceRecommendationTable 3: Recommendation summary table –infection preventionRecommendationSourceClinicians caring for a patient shoulddon appropriate PPE, as per NSWInfection Control ns are to adhere to the fivemoments of hand nt for eye care must be keptin its own container separate fromother patient hygiene equipment.These containers should be passedthrough ward cleaning procedureson a regular basis.Agency for Clinical InnovationGDNconsensus13 SourceAll clinical staff should maintaincontemporaneous documentation ofeye health and interventions.GDNconsensusAll ICUs should ensure clinical staffare competent in the delivery ofappropriate eye care.GDNconsensusAll ICUs should monitor theeffectiveness of eye care deliveredby monitoring for iatrogenicophthalmological complications,through review of adverse events,audit of practice and review of ICUeye consults attended.GDNconsensuswww.aci.health.nsw.gov.au
Eye care of the critically ill: Clinical practice guide December 2021Appendix 1: Identifying ophthalmicabnormalitiesOphthalmic abnormalitiesa. Chemosisb. Co
Clinical governance related to eye care should include: documentation processes for eye health and interventions competency assessment for ICU staff in the delivery of eye care review of adverse events and ICU consults and audits of practice to monitor delivery of eye care.