Transcription
REIMAGING COMMUNITYHEALTH WITH TRIBES: ANEMPOWERMENT-BASED,EQUITABLE MODELBillie Jo Kipp, Ph.D.Center for Native American Youth at the AspenInstitute9/14/2106.027.15 SEA
The changing demographics in theUnited States point to an increasinglyethnically and racially diversepopulation. By the year 2050, it isexpected that racial and ethnic minoritygroups will constitute half of the totalU.S. population (U.S. Bureau of theCensus, 2001).06.027.15 SEA
Health disparities refer to differencesbetween groups of people. These differencescan affect how frequently a disease affects agroup, how many people get sick, or howoften the disease causes death. One definition of Health Disparities is adifference in health care quality not due todifferences in health care need or patientpreferences.06.027.15 SEA
60% of Native Americans relyon IHS for health care06.027.15 SEA
What is the“Healthy Community”Model? The model was conceived by the World HealthOrganization (WHO) as a method of putting intoaction global concepts of health promotion. Goal; To promote the well-being and health ofcommunities by collaborative action at the locallevel.06.027.15 SEA
Healthy Community modeldoesn’t acknowledge: “Onesize fits all?” Relationship-based communities Impact of Inter-generational trauma Healing intergenerational trauma Impact of diverse levels of Acculturation (withinTribal communities) Cultural protocols not recognized Unique Tribal service delivery systems06.027.15 SEA
The Filtering Process:RelationshipsAll relationships(individuals/group) arefiltered through: Impact of Trauma Acculturation, Core psLevel ofAcculturationInter-GenerationalTrauma06.027.15 SEA
All Tribal Systemsare filteredthrough:a) Impact of Traumab) Acculturation,c) Core values,beliefs.Level ofAcculturationTribal rauma06.027.15 SEA
Factors which increase communityparticipation (Joffres, et. al., 2002)Feelings of achievement: Efforts are perceived as being worthwhile, Identified participation as a valuablelearning experience, exciting or rewarding, Increased knowledge in communitymobilization processes, Satisfaction with collaboration with otherparticipants (trust & bonding)06.027.15 SEA
Factors that inhibit participation:(Joffres, et. al., 2002) Feelings of inadequacy (or lack of expertise),shyness (or social fears), Organizational processes (no prior experiencewith the issue or action planning process), Interacting with “expert” group members(overwhelmed with language being used andmeeting procedures, heavier work loads and timeconstraints) Inter-group conflict (role ambiguity)06.027.15 SEA
Paradigm Shift Tribal communities have begun to see their worldviews, values and beliefs not as outdated, but asinvaluable cultural survival mechanisms. Today historical spiritual beliefs and traditionalhealing practices of Tribes are now being recognizedas culturally specific community interventions. Since the establishment of IHS the use of westernbased medical protocols all but eliminated traditionalTribal healing practices. U.S. funding of IHS remains superficial: federalprisoners and Medicaid recipients receive twice theamount of federal funding than American Indiancommunities (U.S. DHHS, 2004).06.027.15 SEA
Diabetes and AmericanIndians/Alaska Natives American Indians/Alaska Natives are twice as likelyto be told by a physician that they have diabetes astheir non-Hispanic white counterparts. They are alsoalmost twice as likely to die from diabetes as nonHispanic whites. Data is limited for this population. American Indian/Alaska Native adults were 2.7 timesas likely as white adults to be diagnosed withdiabetes.06.027.15 SEA
American Indians/Alaska Natives were almosttwice as likely as non-Hispanic whites to diefrom diabetes in 2006. American Indian/Alaska Native adults were1.6 times as likely as White adults to beobese. American Indian/Alaska Native adults were1.3 times as likely as White adults to havehigh blood pressure.06.027.15 SEA
3 Key Aspects of the ECHOModel1) rural diabetes teams will have access to acentralized multidisciplinary diabetes team ona weekly basis to discuss and co-managepatients2) community health workers will have theopportunity to gain expertise andcertifications as community diabetes healthaids3) all members of the newly establisheddiabetes team will have the opportunity tolearn new skills in changing patient behaviorthrough motivational interviewing training06.027.15 SEA
Collaboration for effective changein diabetes management Collaborative will be designed to establish a rollingenrollment with mentorship by current collaborativemembers. develop and institute a diabetes education certificatefor Para professionals including Promatoras,Community Health Representatives and MedicalAssistants to increase the pool of persons qualified topromote diabetes education and self monitoring. train members of diabetes teams to bettercommunicate with patients in a patient centeredcultural appropriate manner.06.027.15 SEA
We expect to address amedical system that has: Resulted in patients do not understand whatis being asked of them Have confidence in what they are beinginstructed to do, nor feel that they areinvolved in their care. Poor adherence to treatment plans and lackof confidence in the health care system is theend result of these deficiencies.06.027.15 SEA
Top down model (unidirectional)Ongoing Training Lectures going Training Lectures Literature Case 15 SEA
Positive Self EfficacyNow I understand the disease. When I firststarted as a CHR I was lost. I knew aboutdialysis, but not diabetes. I was scared to dohome visits. Now I’m more at ease, I can answertheir [patients] questions. I feel good now.NegativeThe same barrier. As far as now, some of IHSstaff, they didn't want to work with us. We wantedto work with them, but they wouldn't give ussupplies. That needs to be clarified. We weretold to cease all case management.No matter how long we’ve done this we alwayslearned something new from ECHO. It’sincreased my confidence you know you’resaying the right thing to patients. Role Expansion[the training] taught me things that I had no clueof before – like foot screens. Previously I wasjust a translator for elderly patients – this openedup so much more that I can do. Our hospital isunder a new CEO who wants to use promotoresas part of this new community outreach. I thinkECHO training helps with this potential new role.I wondered how this would work with the diabetesprogram we have here. My concern – we’d bestepping on their feet?Wondering how much this would add to my workload. Can I handle it.06.027.15 SEA
Positive Organization supportThe Indian Health Service diabetesprogram; we’ve been going around on that,getting glucometers’. We had beenworking with case management with them;it’s kind of up in the air. I’m not sure of HISgave us the round around on gettingglucometers supplies. Right now casemanagement is at a halt. Support and ValidationYes! We have Support! It was clear that theECHO staff acknowledged the importanceof CHWs/Promotores. I looked forward tohearing what other CHRs/Promoteres were Opportunity to learndoing.For me ECHO was basic to a level we could understand. Ifthere was a big word you would explain it better so wecould understand. At conferences sometimes they talk uphere. The hands on helped it was to my level where Iunderstood.NegativeThe nurse used to give us referrals and Iwould see them at home right away Iwould tell them to go to theclinic sometimes they won’t go.Now shewon’t give me any referralsI thought the teleconference was good, except when we hadwork06.027.15 SEA
Complexity of the diseaseIt’s helped getting moreinformation/knowledge on that[diabetes]. Withthe tribe’s diabetes program we’re pused tothe side. I told the CHRs to keep doing homevisits. We can make suggestions, you know,“have you thought about losing weight?”They can distribute the information we give.Like the genetics, how some families havemore diabetes, more knowledge to share withpatients. So it helped out, the elders comingexpressed they were glad. With our tribe alcohol abuse goes hand in hand withdiabetesI think it’s the clients. I have one that’s going to bestarting dialysis. I went over that’s why we come outwith our education so you don’t have to go that far.She was mad at the world. Sometimes it’s like “I feelfine, I can eat what I like” then they end up needingdialysis. “No I’m not diabetic. I get mad at thedoctors for saying that because I’m not.” Trying tohelp them out, but they refuse.ResourcesECHO gave me somewhere other than theprovider to go with my question – I feelmore comfortable asking them [ECHO] thanasking medical providers. I know if I’mstuck on something or a patient asks mesomething I don’t have an answer for I canrely on getting the right answer from ECHONot only the ECHO staff, but the networkingwith other CHWs has really helped. Wesometimes email each other, sometimes wecall, it’s a lot of help.06.027.15 SEA
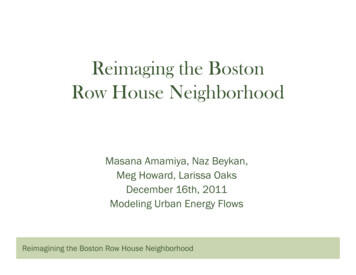
Participants completed threesurveys at baseline:Diabetes Attitude Survey (DAS-3)a modified version of the Diabetes KnowledgeSurvey (mDKT), and aDiabetes Confidence Survey for CommunityHealth Paraprofessionals (DCS-1)06.027.15 SEA
mDKT% correctCCS(scale 1-5)CNS(scale 1-5)DASBaselineCompletion ofSignificance (p6- month 024.104.390.04modified Diabetes Knowledge TestDiabetes Confidence Survey Clinical SkillsDiabetes Confidence Survey Non Clinical skillsDiabetes Attitude Survey06.027.15 SEA
Culture perceived as a“Reziliency Factor” Today Tribal communities are calling for theintegration of traditional medicine as a criticalfacet of health care delivery systems(Belcourt-Dittloff, & Belcourt G.M., 2007).06.027.15 SEA
Practical Implications Achieving good health for American Indians requiresmore than symptom-focused, clinic-based care. Itrequires an informed consideration of tribal history,an awareness of demographic influences and socialdeterminants, and a complementary system ofwisdom-based knowledge, cultural practices, andculturally sensitive Western medicine approaches. Health is not the sole responsibility of a tribal healthdepartment. In tribal communities the Western notionof integrated care must be indigenized to includehealth-related linkages across ALL programs(community caring), e.g., every program mustdemonstrate how its mission and vision contributesto the health and well being of the People.06.027.15 SEA
The persistence and revival ofindigenous American Indianhealing is due not to a lack ofmodern treatment services,but to a need for culturecongenial and holistictherapeutic approaches.(Jilek,1978)06.027.15 SEA
Ultimately, it is thecommunity thatcures.To cure thewounded, oneneed only returnthem to theircommunity orconstruct a newone.--Philip Rieff, 198706.027.15 SEA
06.027.15 SEA
06.027.15 SEA
06.027.15 SEA REIMAGING COMMUNITY HEALTH WITH TRIBES: AN EMPOWERMENT-BASED, EQUITABLE MODEL Billie Jo Kipp, Ph.D. Center for Native American Youth at the Aspen