Transcription
FRANCISCAN CENTER FOR WEIGHT MANAGEMENTST. FRANCIS HOSPITAL, FEDERAL WAY, WASHINGTONPATIENT GUIDEFranciscanWeightLoss.org
TABLE OF CONTENTSWelcome.3About Morbid Obesity.55 What is Obesity?5 How Do You Know If You Are Morbidly Obese?Types of Procedures.77 Roux-en-Y Gastric Bypass8 Vertical Sleeve Gastrectomy9 Adjustable Gastric Banding10 Biliopancreatic Diversion with Duodenal SwitchPaying for Surgery.1112 Frequently Asked Questions: InsuranceCommon Questions About Weight Loss Surgery.1515 General Questions19 Weight Loss Surgery and Smoking20 Medications and Weight Loss SurgeryPostoperative Emergency Information can be found behind the orange divider.1
Nutrition.2324 Tips for Change: Start Now!27 What to Expect After Your Procedure28 Typical Bariatric Diet Progression29 The Four Stages54 Bariatric Pyramid55 Serving Sizes62 Learn About Dumping Syndrome65 Common Problems and Solutions70 Frequently Asked Questions: NutritionPost-Surgical Exercise.7373 General Precautions73 Exercise Recommendations75 Benefits of Physical Exercise75 Taking Your Heart RatePostoperative Care and Contact Numbers.7778 What Can I Do to Help Myself?Postoperative Emergency Information can be found behind the orange divider.
WelcomeWELCOME TO THEFranciscan Center forWeight ManagementCongratulations on taking your first step toward learning more about weight loss surgery. Oursurgeons Haroon Anwar, MD, Troy Houseworth, MD, and David Swedler, DO, along with theirstaff, would like to welcome you and thank you for choosing the Franciscan Center for WeightManagement at St. Francis Hospital.The decision to have weight loss surgery is life-changing. Our clinic’s staff will provide youwith guidance and support throughout your journey. We will help you obtain insuranceauthorization and schedule preoperative testing and procedures. We also have nutrition, nursingeducation, postoperative care and support. Weight loss surgeries are performed at St. FrancisHospital, which is accredited by the Metabolic and Bariatric Surgery Accreditation and QualityImprovement Program (MBSAQIP).Making the decision to have weight loss surgery is not an easy one. Don’t let anyone tell you thatthis is the “easy way out.” Weight loss surgery requires a lifetime commitment to healthy living, acommitment to a daily nutritional regimen and, most importantly, a commitment to utilize a toolthat will help you live a healthy, normal life.Once you have made the commitment to change your life, we are standing behind you in supportof each healthy step you take. We are excited to begin a new partnership with you and help youachieve, and perhaps even exceed, your healthy weight loss and wellness goals.Committed to your success,Haroon Anwar, MD, FACSTroy Houseworth, MD, FACSDavid Swedler, DOKimberly Smits, ARNP, FNP, CBNElizabeth Fujii, PA-CGretchen Hoffman, RDDeanna Eisele, RD3
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDE4
ABOUT MORBID OBESITYWhat is Obesity?Obesity is excessive body mass, and one is generally considered obese if the Body Mass Index(BMI) is greater than 30. “Morbid” means causing disease or injury. Morbid obesity, meaninga BMI of over 40, is a serious disease in which the accumulation of fatty tissue becomesexcessive and interferes with or injures other organs, causing serious and life-threatening healthproblems. These problems are called comorbidities.Morbid obesity is recognized by the consensus of medical opinion as a serious problem and adisease. In most cases, the underlying problem is genetic, meaning you inherit the tendency togain weight. Once the problem is established, there is very little that willpower can do about it, anymore than a person with diabetes can control his or her blood sugar by willpower.How Do You Know If You Are Morbidly Obese?There are three criteria:You are more than 100 pounds over your “ideal body weight.” Your ideal body weightrefers to a weight at which you are statistically likely to live the longest, not the weight youwish you could be (which is usually lower).Your BMI is greater than 40, or greater than 35 and accompanied by serious comorbidities.You have comorbidities from being seriously overweight. Some examples are high bloodpressure, edema, high blood sugar, shortness of breath, etc.5
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDE6
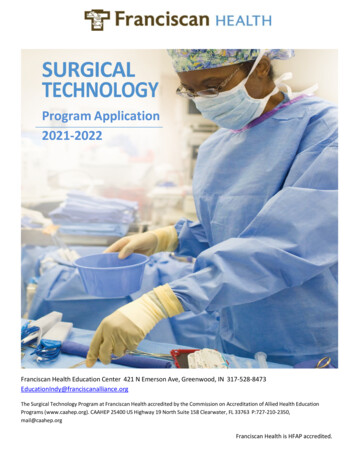
Types of ProceduresTYPES OF PROCEDURESRoux-en-Y Gastric BypassThe gastric bypass involves the creation of a smallstomach pouch, where the surgeon attachesa portion of the small intestine onto the newstomach (pouch). As food is taken in, it actuallybypasses the first section of the small intestine.This section is responsible for the absorptionof calories and nutrients. Creating a smallerstomach will allow patients to feel full quickerwhile eating less food. The patient absorbsfewer calories due to the food now bypassing apart of the small intestine.What are the benefits?Patients have a sense of fullness, which reduces the desire to eat more. Overall, patients whohave the gastric bypass procedure will typically lose more weight in less time than those whohave a restrictive-only procedure such as banding. Patients undergo preoperative training to learnbehavior modification so that they are fully prepared for the surgery.With gastric bypass, the food bypasses the first part of the small intestine, which decreases traveltime through the digestive system. This rapid movement of food through the system can initiatedumping syndrome. This syndrome is generally caused by ingesting too much sugar at one time.It can cause the patient to feel flushed, jittery and nauseated, and/or have diarrhea along with coldsweats. Although not something one would normally say is a benefit, in this case, it is a behaviormodification tool that tells you when you are taking in too much sugar, so that you know where andwhen to adjust what you are eating.What are the risks?Gastric bypass surgery risks can include anemia, bone calcium loss, anastomotic leaks, fistulas,internal hernias, small bowel obstructions, metabolic bone disease, iron deficiency, vitamin B12deficiency, dumping syndrome and the formation of ulcers.7
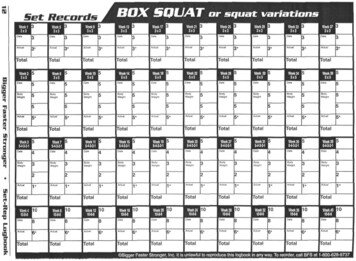
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDEVertical Sleeve GastrectomyA thin sleeve about the size of a smallbanana is created out of the side of thestomach. A stapling device is used todivide the stomach vertically. Whenthis is completed, the remainderof the stomach is removed fromthe abdomen, leaving only thenew smaller sleeve. Unlike gastricbypass, food will continue to passthrough the normal digestiveprocess, as there is no bypassingthe small intestine.What are the benefits?The new stomach sleeve is muchsmaller than the old stomach, therebyreducing the amount of food your stomachwill hold and giving you a feeling offullness with less food.What are the risks?Sleeve surgical risks can include gastric leaks or tissue separation, the formation of ulcers, fistulas,worsening reflux and indigestion.8
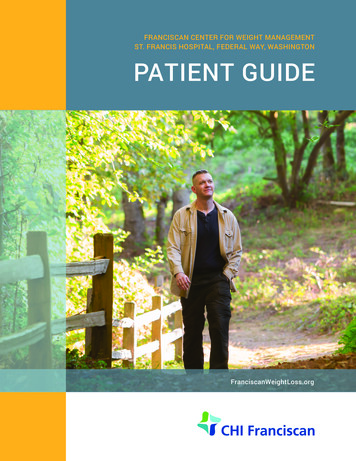
Types of ProceduresAdjustable Gastric BandingAdjustable gastric banding utilizes a silicone band that is placed around the upper portion of thestomach to create a small upper pouch and lower stomach. The banding is considered a restrictiveprocedure that limits food intake. Attached to the band is tubing that connects to a port, which liesunderneath the skin on the abdominal wall. This port is where the surgeon can fill or remove salinefrom the silicone bandas needed.What are the benefits?Gastric banding creates a smallerpouch and entry point into thestomach, which, in turn, limits theamount of food one can take in at anyone time, while still feeling full. Theport is located right under the skin foreasier access in the surgeon’s office toregulate the amount of fluid in the bandas needed.What are the risks?Gastric banding surgical riskscan include acid reflux, nauseaand vomiting, outlet obstruction,esophageal dilatation or dysmotility,gastric perforation, lack of feelingfull and pouch dilation. The siliconeband could also slip from its surgicalplacement or develop a leak, causingthe balloon to deflate.9
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDEBiliopancreatic Diversion with Duodenal SwitchThe duodenal switch is similar to a gastric bypass in that it bypasses a section of the smallintestine. Unlike the bypass, which forms a small pouch, the duodenal switch creates a sleeveshaped stomach and separates the small intestine. This process leaves a smaller stomach withseparate routes for the digestive juices; absorption bypasses the small intestine. Patients feel fullearlier and fewer calories are absorbed.What are the benefits?The duodenal switch is routed differentlythan the gastric bypass, and due to this, thepatient is not likely to have problems withdumping syndrome. There will also be fewerchances of forming ulcers, stoma closuresand blockages.What are the risks?Duodenal switch surgery requires lifelongmonitoring for protein absorption, vitaminsupplementation, chronic anemia andbone loss, and presents increased risk ofulcers and gallstone formation. In addition,especially in the first few months, thepatient may experience frequent liquid bowelmovements, abdominal bloating and strongsmelling stool or gas.10
Paying for SurgeryPAYING FOR SURGERYNavigating insurance policies and figuring out all of the charges surrounding weight loss surgerycan be daunting. We have put together some answers to the most common questions below. Ifyou have further questions, please contact the clinic at (253) 944-2080.Many insurance plans will cover the costs of weight loss surgery, but coverage varies according toyour medical history, insurance policy and benefits, or exclusions.If you would like to begin researching your options, you may call your insurance provider and askif weight loss surgery is a covered benefit under your specific policy. Ask for a description of yourbenefits related to weight loss surgery in general and if only specific procedures are covered.Also, your employer may offer different plans from different companies, some of which maycover surgery and some that may not. If your current insurance policy does not cover weight losssurgery, contact your Human Resources department to see if there is another policy option thatdoes. If another plan offers this option, you may have to wait until your company’s new enrollmentcomes around to change plans.How quickly you hear from us on whether or not you have been approved will depend on yourmedical history and insurance approval.All insurance companies have some type of criteria that you must meet before they will approveyou for surgery. Keep in mind that carriers vary in what they require, so not all the following willapply to all patients. Criteria MAY include:Proof that you have a BMI of 40 or moreProof that you have a BMI of 35-40 with comorbidities such as diabetes, sleep apnea,hypertension or high cholesterolDocumentation of weight history for the past two yearsRecord of a three-to-six month medically supervised weight loss programConsult with a registered dietitianConsult with a psychologistWe work closely with many insurance companies to improve our program, which results in betteroutcomes for our patients. We perform all our bariatric surgeries at St. Francis Hospital in FederalWay, Washington.11
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDEFrequently Asked Questions: InsuranceWhat can I do if my insurance doesn’t cover weight loss surgery?If your insurance company or specific company policy does not cover weight loss surgery, youmay opt to pay for it yourself. There are a few ways you can do this.We understand that bariatric surgery is something you care deeply about. Both you and yoursurgeon believe that you could greatly benefit from surgery, so we are providing additionalsuggestions for paying for your surgery if you are not covered by insurance.Obesity is recognized as a medical disease and the Internal Revenue Service has deemed thatout-of-pocket costs for physician-directed weight-loss programs are tax deductible. What does thismean to the patient? Patients may be able to take the cost of the surgery off their income tax. Thisis for any money that you had to pay out-of-pocket, NOT money that was paid by your insurance.Two websites that our patients have successfully used for medical loans are:Medical loans: www.medloanfinance.comSurgery loans: www.surgeryloans.comNote: We are not contracted with Care Credit.How long does it take to schedule surgery?We can usually schedule surgery immediately upon approval of insurance or after financialarrangements are made. When we obtain approval, we will contact you to determine if and whenyou are ready to schedule surgery. From that time, surgery can be within the next two months or atyour convenience.Why does it take so long to get insurance approval?Once all of the insurance requirements are met, it usually takes us one to two weeks to send aletter to your insurance carrier to start the approval process. The time it takes to receive an answerback can vary from about two to six weeks or even longer if the carrier is not prompted. There willbe times that it helps to have you, as the patient, call your insurance company and regularly inquireabout the status of your request.12
Paying for SurgeryHow can an insurance carrier deny coverage for alife-threatening disease?Coverage may be denied because there is a specific exclusion in your policy for obesity surgery ortreatment of obesity. If there is a written exclusion stated in your policy, ask your employer aboutother policies. There may even be a short-term policy that can be used. When there is only onepolicy, and a written exclusion is listed, it might be time to look for other options such as self-payand/or medical loan programs.You may be denied for a lack of “medical necessity.” In some cases, weight loss surgery is deemedmedically necessary only when it is used to treat a serious or life-threatening condition. Further,in the case of morbid obesity, some believe that dieting, exercise and medications are appropriatealternatives to surgery.Usually, medical necessity denials hinge on the insurance company’s requirement for some formof documentation, such as one to five years of physician-supervised diet and/or a psychiatricevaluation. The best approach is to try to produce reasonable documentation up front.What can I do to help the process?First, help us gather all the information so the carrier cannot deny for failure to provide necessaryinformation. Letters from your personal physician and any dietary consultants you may have seenattesting to the medical necessity of treatment are extremely valuable in proving your case to theinsurance company. When one or several physicians agree to the medical necessity of treatment,it will be hard for the carrier to contradict them. Once the letter is submitted, call your carrierregularly (once per week) to ask about your status.You can appeal a denial as long as it is not due to a written exclusion in your insurance policy. If allelse fails, we can walk you through the self-pay options.13
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDE14
Common Questions about Weight Loss SurgeryCOMMON QUESTIONS ABOUTWEIGHT LOSS SURGERYGeneral QuestionsHow successful is bariatric surgery?Weight loss surgery works successfully for any patient who is committed to change. Whencomparing methods of weight loss, patients who have undergone:Lifestyle changes and medication regimen only for weight loss overall have less than10 percent long-term success.Laparoscopic adjustable gastric banding for weight loss have a 40-50 percent chance oflong-term success.Sleeve gastrectomy for weight loss have a 55-65 percent chance of long-term success.Gastric bypass for weight loss have a 65-75 percent chance of long-term success.Success rates for bariatric surgery far exceed those for conventional dieting, especially whenpatients take advantage of the additional support and dietary and nursing education offeredto all patients. Weight loss surgery is not successful for every patient, as each patient must beultimately committed to the process from beginning to end, and then continue the new healthylifestyle behaviors throughout their lives. However, those who are well motivated and who receiveappropriate postoperative support can achieve significant, lasting weight loss.It is important to discuss risks and possible benefits with your doctor when considering weightloss surgery. Bariatric surgery has associated risks and long-term consequences and should beconsidered as only part of an approach to treating obesity. Our surgeons believe the operationswork best with lifelong behavioral and dietary changes. Long-term follow up with your bariatricteam, as well as lifelong vitamin supplementation, are essential to avoid life-threateningcomplications down the road.15
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDEWhat are the screening procedures for bariatric surgery?Although your physical condition may meet guidelines for bariatric surgery, this does notguarantee eligibility. At the Franciscan Center for Weight Management, we conduct a verycomprehensive screening program to ensure you are:Ready to make long-term changes in your eating, exercise and lifestyle habits.Committed to long-term medical follow-up.Without significant or unstable conditions that could make the surgery too dangerous,such as respiratory, cardiovascular, gastroenterologic or psychological conditions or bloodclotting disorders.Without recent cancer.A good candidate, as determined by our bariatric surgeons and the National Institutes ofHealth (NIH) Federal Guideline for Bariatric Surgery.The screening process is essential to eliminate candidates who are unlikely to benefit from weightloss surgery due to their inability to manage the psychosocial factors of weight loss surgery, or dueto their body’s inability to safely and effectively handle the demands of the surgical procedure.What are some complications and risks of weight loss surgery?Weight loss surgery is a serious procedure, during which complications can cause death in lessthan 1 percent of cases. To reduce the risk of complications, patients should carefully follow thedietary and exercise guidelines of their bariatric surgeon and dietitian. Additional risks includevomiting, which can occur when the small stomach pouch is stretched by food that has notbeen chewed well. Approximately 10-20 percent of patients require follow-up surgery to correctcomplications, commonly abdominal hernias. A hernia can be caused by vomiting or strainingafter surgery before the incision heals. Laparoscopy and robot-assisted surgery greatly reducehernia risk.Other possible health complications include: a 1 percent chance of blood clots occurring in thelegs after surgery; a 5 percent risk of infection in the incision area with open procedures, lesswith laparoscopy and robot-assisted; breakage of the gastric staple line after vertical sleeve;band slippage and saline leakage after adjustable gastric banding; and, on rare occasion, bowelobstruction as a result of adhesions caused by scar tissue.Staple Line LeaksStaple line leaks can occur with gastric bypass, sleeve gastrectomy or duodenal switch.More common 24-48 hours after surgery but can happen anytime.16
Common Questions about Weight Loss SurgeryLeaks are a very rare complication.Signs and symptoms: Abdominal pain that worsens and is not relieved by your pain medicationLeft shoulder painNausea/vomitingFeverHeart rate greater than 120 sustainedPrevention Your surgeon will check for leaks in the operating room.You will have an X-ray the morning after your procedure to check for a leak.Treatment You may need further surgery to repair the leak.Some leaks will heal without further surgery.Your surgeon will determine the best treatment for you.Adjustable BandsInfectionErosionBand slippage Mechanical complications:Port and/or tubing leakFlipped portEsophageal dilatation or dysmotilityAny of the above complications with the band could result in further surgery to replace or removethe band.Contact your surgeon for any questions or concerns you may have regarding surgicalcomplications at (253) 944-2080 during normal business hours.17
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDEHow do “restrictive” and “malabsorptive” procedures differ?Restrictive procedures limit the size and access to the stomach itself, whereas malabsorptiveprocedures are typically those that bypass portions of the intestinal tract. With malabsorptiveprocedures like gastric bypass, the patient no longer absorbs nutrients in the normal way.Examples of restrictive procedures are gastric banding and sleeve gastrectomy. Some bariatricprocedures, such as the gastric bypass and duodenal switch, are a combination of both restrictiveand malabsorptive methods.What do you mean by “bariatric surgery is a tool,” and how doesthat work?Bariatric surgery is not a cure for obesity but it can help by regulating eating behaviors. Weight losssurgery with a healthy diet and regular exercise will be essential to lifelong weight management.How do laparoscopic, open and robotic-assisted surgery differ?Laparoscopic surgery is performed through small incision ports in the abdomen where thesurgeon places instruments including a camera. The instruments are an extension of the surgeonand everything is completed with instrumentation through the ports. The surgeon does not havehis hands directly inside the patient’s abdomen. The patient will go home with approximately fourto five, 1-inch or smaller incisions. This makes it easier for the patient to get around after surgerywith less pain and less chance of infection or hernias.Open surgery is performed through an incision large enough for the surgeon to actually placehis hands on and visually see the area on which he is operating. The patient goes home with alarger incision, increasing the possibility of postoperative infections. This also makes it moredifficult for the patient to get around after surgery, as they may have more pain and additionalrestrictions than the patient who has laparoscopic surgery.The robot-assisted bariatric surgery is similar to laparoscopic in that the surgeon uses ports,but instead of standing over the patient during surgery, the surgeon is sitting at a stationmanipulating the robot. With the finite articulation of the robot extensions, the surgeon has theability to perform more precise techniques, and meticulous dissection and suturing for complexcases. The patient has smaller incisions with less pain and minimal chance for infection, thesame as laparoscopic surgery.How long will I be in the hospital?Bariatric patients are in the hospital for one to three nights, but most of our patients will stay onlyone night, going home the day after surgery. If there are additional health concerns, your surgeonmay have you stay more than one night.18
Common Questions about Weight Loss SurgeryI live a long way from St. Francis Hospital in Federal Way. Do I haveto stay in the area until my one week postoperative visit?If you live outside of the South Puget Sound area, you may want to consider staying with a friendor family member in the area just so you are close to St. Francis Hospital—but you are not requiredto do so. In case of emergency, you would go to the nearest emergency room, no matter whereyou are located.What will I do with my medications before surgery?Prior to surgery, you will stay on all your medications until either your surgeon or the preoperativenurse from St. Francis Hospital tells you differently. You will want to create a list of your currentmedications so that you have it ready when the preoperative nurse calls you and goes through eachmedication. If you have access to MyChart, you can print out your list of current medications fromthere. Go onto MyChart, click on My Medical Record, then click on Medications and print a copy.Weight Loss Surgery and SmokingDo I have to stop smoking prior to having the surgery?Yes, you will have to stop smoking three months prior to your surgery; this includes both cigarettesand e-cigarettes. This is a surgeon-preferred requirement, as smoking impairs your body’s ability toheal itself. Bariatric surgeries are complex procedures and your body will need all the help you cangive it before and after surgery. Smoking cessation will be a lifelong requirement after weight losssurgery to avoid ulcer formation and other gastrointestinal concerns.What are potential complications if I don’t stop before surgery?Complications from nicotine can include: restricted blood flow; increased blood pressure; poortissue perfusion and increased inflammation leading to a higher risk for wound infections andulcers; impaired healing and diminished cardiac and lung capacity. Your surgeon may delay orcancel your surgery if you have not stopped smoking within the specified time period. Any of thesecomplications can lead to a longer postoperative recovery stay. If you need help to stop smoking,please talk to your primary care physician, as he or she may prescribe something for you.Are you READY to quit smoking?For more information on quitting, please visit Tacoma-Pierce County Health Department’s TobaccoPrevention Program at tpchd.org or call (253) 798-6500 or (800) 992-2456. Most counties have aTobacco Prevention Program, so you can find one that is closer to you if desired.19
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDEMedications and Weight Loss SurgerySome medications can cause problems for the surgery itself, as they may delay healing, cause theblood to be too thin or interfere with other body systems. The following medications will need tobe stopped prior to surgery or changed after surgery. Your surgeon will let you know of any neededmedication changes at the time of discharge from the hospital.Aspirin/NSAIDs (both OTC and prescription)Examples: Aspirin, ibuprofen (Advil, Motrin), naproxen (Aleve, Naprosyn), Diclofenac(Voltaren), Celebrex, mobic, piroxicam, Nabumetone, EtodolacStop one week prior to surgery. If you are taking one of these medications it is important totalk to your prescriber prior to surgery to find an alternate plan of care for any chronic painissues after surgery. Alternatives may be Celebrex, Flector Patches or Diclofenac Gel (VoltarenGel), which are less irritating to the new stomach. (See the “Medications to Avoid AfterSurgery” section on the next page for more detail.)Diabetes medication and insulin therapyMetformin: Stop two days prior to surgery.If you are on insulin, continue to take your blood sugar readings and take your insulinas needed.You should know: If you are on insulin therapy for diabetes, your insulin dosage will changeafter surgery, as your diet will be very different. Some patients notice large reductions in theirinsulin dose within a few days of surgery. It is very important that you monitor your bloodsugars closely and adjust your dose to avoid developing hypoglycemia. Be sure to discuss yoursurgery with your diabetes care provider and have a plan to manage your sugars after surgery.Hormone replacement therapy or oral birth control pillsExamples: Premarin, testosterone, estrogen, Estradiol, Enjuvia, Cenestin, Striant, Testopelor Depo-TestosteroneStop two weeks prior to surgery.You should know: Oral birth control medications may not work effectively after gastric bypasssurgery, as it is no longer absorbed in the same way. Patients are advised to consider changingtheir birth control method to Depo-Provera injections, Nuva Ring, Ortho Evra Patch or an IUD/implant. Because these options do not rely on intestinal absorption they can be fully effective.Inquire with the surgery clinic about when to restart these medications; they may be held aftersurgery due to increased risk of blood clots.Blood thinners/anticoagulants (Coumadin)Examples: Heparin, Warfarin, Coumadin, Eliquis, Plavix, XareltoContact your PCP or anticoagulation unit to obtain a different therapy leading up tosurgery no more than five days prior to surgery.20
Common Questions about Weight Loss SurgeryYou should know: If you take a blood thinner/anticoagulant, your dosage may change quicklyafter surgery. You will need to have your INR checked every three or four days as your dietchanges after surgery until you are on a stable regimen. Make sure your anticoagulation provideris aware you are having surgery so they can schedule you appropriately.SteroidsExample: Prednisone tabletsInhalers containing Prednisone are OK.Talk to the prescribing physician to obtain a step-down dose. Prednisone needs to bestopped no later than 1 week prior to surgery.If you are on long-term steroid use, discuss this with your surgeon.DiureticsExamples: Lasix, Hydrocholorthiazide (HCTZ), Furosemide, Spironolactone or ThiazideStop the day before surgery.These may be withheld after surgery to avoid the risk of dehydration. Your surgeon willinstruct you on use prior to discharge from the hospital.Cholesterol medicationsExamples: Simvastatin, Lovastatin, Fenobibrate, Gemfibrozil, Pravastatin, Zetia or TricorStop the day before surgery.Medications to avoid after surgeryLiquid medications that are not sugar-free may cause dumping syndrome after surgery. Be sureto check with the pharmacist if the label does not say sugar-free.After gastric bypass surgery, you will need to find an alte
FRANCISCAN CENTER FOR WEIGHT MANAGEMENT PATIENT GUIDE 10 Biliopancreatic Diversion with Duodenal Switch The duodenal switch is similar to a gastric bypass in that it bypasses a section of the small intestine. Unlike the bypass, which forms a small pouch, the duodenal switch creates a sleeve-shaped stomach and separates the small intestine.