Transcription
COLLECTING SOCIAL DETERMINANTSOF HEALTH DATA USING PRAPAREThis project was madepossible with funding from:TO REDUCE DISPARITIES, IMPROVEOUTCOMES, AND TRANSFORM CARE1
BACKGROUND ON PRAPARE2
HEALTH, ACCOUNTABILITY & VALUE Under value-based pay environment, providers are heldaccountable for costs and outcomes Difficult to improve health & wellbeing and deliver valueunless we address barriers Current payment systems do not incentivize approachinghealth holistically and in an integrated fashion Providers serving complex patients often penalized without riskadjustment3
PRAPARE:PROTOCOL FOR RESPONDING TO & ASSESSING PATIENTS’ASSETS, RISKS, & EXPERIENCESProject Goal: To create, implement/pilot test, and promote anational standardized patient risk assessment protocol to assessand address patients’ social determinants of health (SDH).PRAPAREAssessment ToolTo Identify Needsin ElectronicHealth Record Protocol toRespond to Needs4
TIMELINE OF THE PROJECT Develop PRAPARE tool Pilot PRAPARE implementationYear 2in EHR and explore data utility2015 PRAPARE Implementation &Year 3Action ToolkitDisseminationYear 1201420165
DEVELOPING PRAPAREExperience of ExistingProtocolsStakeholder FeedbackLiterature ReviewAligned with NationalInitiatives:* Healthy People 2020* ICD-10* Meaningful Use Stage 3* NQF on Risk AdjustmentBurden entified 15 Core SocialDeterminants of Health6
PRAPARE DOMAINSCoreUDS SDH DomainsOptionalNon-UDS SDH Domains(MU-3)1. Race10. Education2. Ethnicity11. Employment3. Veteran Status12. Material Security4. Farmworker Status13. Social Isolation5. English Proficiency14. Stress6. Income15. Transportation7. Insurance8. Neighborhood1. IncarcerationHistory3. Domestic Violence2. Safety4. Refugee StatusOlder version in SpanishFind the tool at:www.nachc.org/prapare9. Housing Status and Stability7
UNIQUE ADVANTAGES OF PRAPARE TOOL Design All measures align with more than one national initiative (UDS, ICD -10,Meaningful Use, HP2020) Data can be captured in the Electronic Health Record for NextGen, GECentricity, eClinicalWorks, and Epic Conversation starter and patient-centered Able to make more granular / align with existing data collection efforts Focus on standardizing the need, not the question8
WHAT WE’VE LEARNED FROMIMPLEMENTATION10
PRAPARE PILOT TESTING IMPLEMENTATION TEAMS ANDELECTRONIC HEALTH RECORDSOther EHRs in Development or Interested: Greenway Allscripts Athena Cerner11
WHAT WE’VE LEARNED FROM PILOT TESTINGEasy to use:On average, takes 9minutes to completeformPatients appreciatebeing asked and feelcomfortable answeringquestionsStaff find value in thetool: Helps them betterunderstand patientsand build betterrelationships withpatientsIdentifies New Needs,Often Leading to NewCommunity PartnershipsEmotional Toll onStaff
SAMPLE WORKFLOWSHealthCenterWhoWhereWhenHowRationaleCHC #1Non-clinical staff(enrollmentassistance,community healthworkers)In waiting roomBefore provider visitAdministered PRAPARE withpatients who would bewaiting 30 mins forproviderProvided enough time to discuss SDHneedsCHCs #2Nursing staffand/or MAsIn exam roomBefore providerenters exam roomAdministered it after vitalsand reason for visit. Providerreviews PRAPARE data andrefers to case managerWanted trained staff to collect sensitiveinformation. Waiting area not privateenough to collect sensitive infoCHC #3Non-clinical staff(patient navigators,patient advocates)In patientadvocate’sofficeAfter clinical visitwhen provider referspatient to patientnavigatorPatient advocatesadminister it and then canrelay to provider in officenext door.Wanted same person to ask question andaddress need. Often administerPRAPARE with other data collection effort(Patient Activation Measure) to assesspatent’s ability and motivation to respondto their situation.CHC #4Care CoordinatorsIn office of carecoordinatorWhen Completingchart reviews andadministering HealthRisk AssessmentsAdministered PRAPARE inconjunction with Health RiskAssessmentsAllows care coordinators to addresssimilar issues in real time that may arisefrom both PRAPARE and HRACHC #5Any staff (fromFront Desk Staff toProviders)No wrong doorapproachNo wrong doorapproachAllows everyone to be part of largerprocess of “painting a fuller picture of thepatient” and taking part in helping thepatient
COMMON CHALLENGES ENCOUNTERED WHEN USINGPRAPARE AND SOLUTIONSChallenge: Staff and Patients Don’t Understand WhyDoing PRAPAREChallenge: Have too much going on now to addanother projectSolution: Use short script to explain to staff &patients why health center is collecting thisinformation. Message around better understandpatient and patient’s needs to provide better careSolution: Don’t market PRAPARE as new biginitiative but as project that aligns with other workalready doing (care management, ACO, enablingservices, etc)Challenge: How do weimplement this withoutincreasing visit time?Solution: Find “Value-Added”time, whether in waiting room,during rooming process, orafter clinic visitChallenge: Fitting PRAPARE intoWorkflowSolution: Incorporate into otherassessments to encouragecompletion (Health RiskAssessment, Depression Screening,Patient Activation Measure, etc)Challenge: Inability to Address SDHSolution: Message “Have to startsomewhere and do the best we canwith what we have. Collectinginformation will help us figure outwhat services to provide.”14
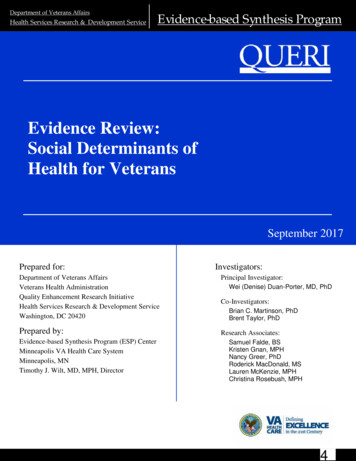
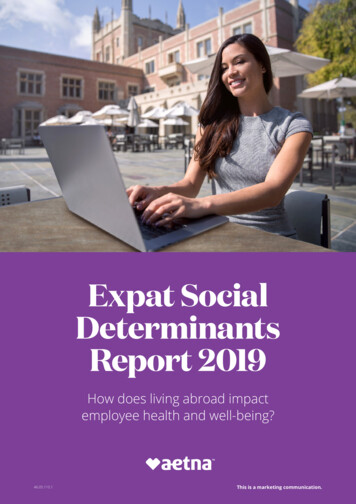
PERCENT OF PATIENTS WITH NUMBER OF SDH“TALLIES”35%N 2,694 patients forall teams30%25%20%15%10%5%0%0123456Alliance/Iowa3 CHCs789 10 11 12 13 14 15 16 17 18 19 20 21 22Tally ScoreWaianaeNew York1 CHC2 CHCsOregon1 CHCTotal7 CHCs
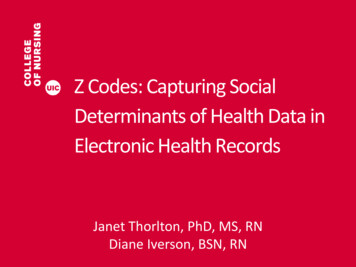
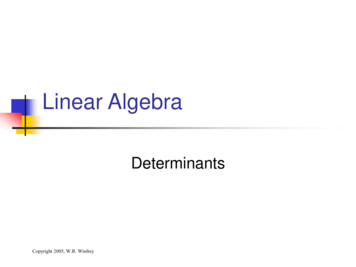
CORRELATION BET WEEN SDH FACTORS AND HYPERTENSION:ALL TEAMS50%r 0.6140%30%20%10%0%01234% of POF56789 10Tally Score111213% of the tally score with Hypertension14151617
HOW PRAPARE DATA HAS BEEN USED TO IMPROVE CAREDELIVERY AND HEALTH OUTCOMESBetter ionBuild services in-house for same-day useas clinic visit (children’s book corner, foodbanks, clothing closets, wellness center,transportation shuttle, etc)Better UnderstandNeeds of PatientPOPULATIONBuild partnerships with local communitybased organizations to offer bi-directionalreferrals and discounts on services (ex:Iowa transportation)Drive STATE andNATIONAL CareTransformationInform both Medicaid and Medicare ACOdiscussions (ex: Iowa, New York)Create risk score to inform risk adjustment(ex: Hawaii)Ensure prescriptions and treatment planmatch patient’s socioeconomic situationGuide work of local foundations (ex: NewYork housing)Streamline care management plans forbetter resource allocation (ex: Hawaii)Inform payment reform and APMdiscussions with state agencies (e.g.,Medicaid) on caring for complex patients(ex: Oregon, Hawaii)17
PRAPARE IMPLEMENTATION AND ACTION TOOLKITwww.nachc.org/prapare Chapter 1: Understand the PRAPARE Project Chapter 2: Engage Key Stakeholders Chapter 3: Strategize the Implementation Process ChapterChapterChapterChapter4:5:6:7:Technical Implementation with EHR TemplatesDevelop Workflow ModelsDevelop a Data StrategyUnderstand and Evaluate Your Data Chapter 8: Build Capacity to Respond to SDH Data Chapter 9: Respond to SDH Data with Interventions Chapter 10: Track Enabling Services18
HEALTH CENTER AND PCAEXPERIENCES WITH PRAPARE19
APCM IN OREGON: USING PRAPARE TO EXPLOREPATIENT SEGMENTATION WITH OREGON CHCS Group of advanced clinics that are participating in an APM whichallows them to create a patient- centric model of care to:Improve clinic population outcomes Improve patient and staff engagement Support open access Contain costs20
EXPERIMENTING WITH PRAPARE We invited clinics to pick a patient population and interview 10consumers using 3 questions from PRAPARE Afterwards, clinics met face-to-face to share their experiences How did you and the patient discuss these questions? What did you observe about the process (your experience, patient’sreaction)? Did asking these questions lead to conversations about other topics?21
APCM: THE BIG PICTUREAPCM Accountability PlanCare Transformation Strategies22 Oregon Primary Care Association
Population Segmentation: Our work NOWTRANSFORMATION STRATEGIES23
FROM GATHERING DATA TO ASSESSMENT TO EMPATHICINQUIRY Expand the medical mental model while enhancing the human connection Trust and understanding is fostered bi-directionally by interviewing with empathy andincorporation of SDoH This interaction, alone, can function as a healing intervention Deepen our understanding of the individuals and populations we ser ve while also releasinghealth care professionals from the entrenched cultural orientation of responsibility to fixother people’s lives Start from respect for patient autonomy and strength; collaborate to develop individual- andcommunity -level solutions Develop the trauma -informed care skills to learn about people’s dif ficult experienceswithout causing re-traumatization Provide a setting where provider teams get to do the work they care about – linked toretention and joy at work24
EMPATHIC INQUIRY DEMONSTRATIONSOPCA Demo: https://www.youtube.com/watch?v 9rfmfsMMeEUWaianae Demo:https://youtu.be/iQjJ QsDvmI25
WAIANAE AND IOWA PCA’S EXPERIENCES26
TRACKING INTERVENTIONS27
RESPONSE NEED Standardized data onpatient risk Standardized data oninterventionsBOTH are necessary to demonstrate health center value28
RESPONSE- DATA ON INTERVENTIONSReport by RCHN Foundation inNACHC Community Health Forum,HIT Connections, Fall/Winter 2014
LACK OF COMPREHENSIVE ENABLINGSERVICES DATAUDS TABLE 5 - STAFFING AND UTILIZATIONPersonnel by Major ServiceCategoryCase ManagersPatient/CommunityEducation SpecialistsOutreach WorkersTransportation StaffEligibility AssistanceWorkersInterpretation StaffOther Enabling ServicesFTEs(a)Clinic Visits(b)Patients(c)
AAPCHO DATA COLLECTION PROTOCOL:THE ENABLING SERVICES ACCOUNTABILIT Y PROJECTEnabling ServicesAccountability Project(ESAP)The ONLY standardizeddata system to trackand documentnon-clinical enablingservices that helppatients access care.CATEGORYCODECASE MANAGEMENT ASSESSMENTCM001CASE MANAGEMENT TREATMENT ANDFACILITATIONCM002CASE MANAGEMENT REFERRALCM003FINANCIAL COUNSELING/ELIGIBILITYASSISTANCEFC001HEALTH tes31
SAMPLE ENABLING SERVICES EMR TEMPLATE
CONCEPTUAL FRAMEWORKSocial Determinants ofHealth(PRAPARE Domains:Race/ethnicity, povertyemployment, Englishproficiency, etc.)Appropriate Care(For health condition in question,for example, # of doctor visits,exams/tests levels )Health Outcomes(For example, idealoutcomes, reducedcomplications, ED visits,etc.)Enabling Services & other non-clinical interventions33
WHAT YOU CAN DO NOW34
RESOURCES AVAILABLE NOW Visit www.nachc.org/prapare PRAPARE Tool PRAPARE Implementation and Action Toolkit Electronic Health Record PRAPARE Templates Readiness Assessment Webinars PRAPARE Overview EHR and Workflow -specific Frequently Asked Questions Visit http://enablingservices.aapcho.org AAPCHO’s Enabling Services AccountabilityProject protocol for data collection of non-clinicalenabling services Enabling Services Data CollectionImplementation Guide White Papers, Best Practices, StudiesContact Tuyen Tran at ttran@aapcho.org Contact: Michelle Jester at mjester@nachc.org35
PRAPAREREADINESS ASSESSMENT Culture of Organization Leadership and Management Workflow Process Improvement Technology Paper form: www.nachc.org/prapare Online form:https://www.surveymonkey.com/r/PRAPARE Readiness Assessment36
FUTURE OF PRAPARE37
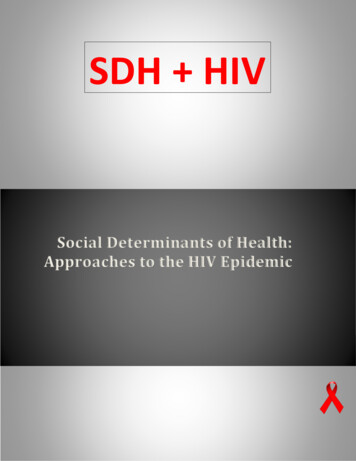
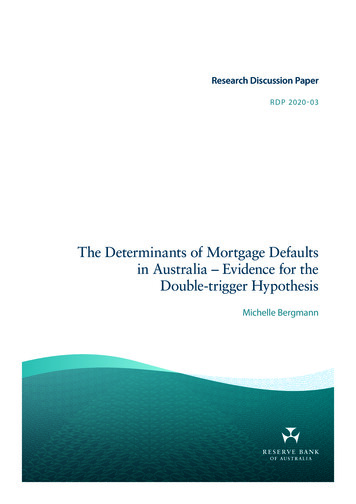
PRAPARE IS A NATIONAL MOVEMENT!Use and Interest in PRAPARE as of October 2016 States where healthcenters are alreadyusing PRAPARE (31states) States where healthcenters or PCAs haveexpressed an interest inPRAPARE (19 states)38
2016 – 2019: NATIONAL PRAPARE LEARNING NET WORK ( PLAN)SPREAD, REFINE, & AUGMENT STANDARDIZED DATA COLLECTION FOR ACTIONPCA/HCCNTrain the TrainerAcademy& Live UniversityValidationandAggregationPromote & SpreadDocument Impactand RiskEnhancementTrack Interventionsand RisksPartnershipsfor ProgressLeverage CollectiveImpact forPopulation Health
UPCOMING SDH FUNDING OPPORTUNIT Y Healthy Places for Healthy People is a new program to help communities partner withcommunity health centers, nonprofit hospitals, and other health care facilities tocreate walkable, healthy, economically vibrant places. Supported by Environmental Protection Agency and the Appalachian RegionalCommission. Communities receive planning assistance to develop action plans focusing on healthas an economic driver and catalyst for downtown and neighborhood revitalization. Learn how to apply for the Healthy Places for Healthy People Program:https://www.epa.gov/smartgrowth/healthy -places-healthy -people Deadline: November 6 th ! Short application40
QUESTIONS AND DISCUSSIONTo receive the latest updates on PRAPARE, join our listserv!Email Michelle Jester at mjester@nachc.org.41
Take Home Activities Complete Evaluation Complete the PRAPARE Readiness Assessment: Paper form available at: www.nachc.org/prapare Online form available at:https://www.surveymonkey.com/r/PRAPARE Readiness AssessmentReadings/Resources for November 17th Housing Webinar1. ASK & CODE: Documenting Homelessness Throughout the Health Care System2. Health and Housing Partnerships: Strategic Guidance for Health Centers andSupportive Housing Providers3. Public Housing Health Centers: 2014 UDS Findings
Next Webinar – November 17, 3:00 PM ESTHousing as a Social Determinant of HealthHousingNov 17th3:00 – 4:15EST Understand relationship between healthCSH,and housing (public, supportive, and lackCHPFS,of.) and role of health centers.NHCHCLearn how to identify and address barriersand challenges within your service areawhich adversely affecting your patientpopulation.Identify opportunities for health centers topartner with housing providers andstakeholders.1.2.3.Health and HousingPartnerships: StrategicGuidance for HealthCenters and SupportiveHousing ProvidersPublic Housing HealthCenters: 2014 UDSFindingsCounting Residents ofPublic Housing on the2015 UDS Report
Housing is a Social Determinant of Health FacultyKristine GonnellaCommunity Health Partners for Sustainabilitykristine@chpfs.orgDarlene M. Jenkins, DrPH, MPH, CHESSenior Director of ProgramsNational Healthcare for the Homeless
THANK YOU!!
UDS SDH Domains Non-UDS SDH Domains (MU-3) 1. Race 10. Education 2. Ethnicity 11. Employment 3. Veteran Status 12. Material Security 4. Farmworker Status 13. Social Isolation 5. English Proficiency 14. Stress 6. Income 15. Transportation 7. Insurance 8. Neighborhood 9. Housing Status and Stability Optional 1. Incarceration History 3. Domestic .