Transcription
Physical Therapy Guidelines for Peroneal Tendon RepairFor the Clinician: The intent of this protocol is to provide the clinician with a guideline of the post-operative rehabilitation for the patients whoundergo a Peroneal Tendon Repair. It is not intended to be a substitute for clinical decision making regarding the progression of a patient’spost-operative course based on their examination/findings, individual progress, and/or the presence of post-operative complications. If aclinician requires assistance in the progression of a post-operative patient, they should consult with the referring surgeon.For the Patient: The timeframes for expected outcomes contained within this guideline may vary from patient to patient based on individualdifferences, surgical techniques, surgeon’s preference, additional procedures performed, and/or complications. Compliance with all therecommendations provided by your physician and physical therapist as well as your active participation in all parts of the rehabilitation process,are essential to optimizing the success of this procedure.Introduction:The peroneal tendons are extensions of the peroneus longus (fibularis longus), peroneus brevis (fibularis brevis),and in some the peroneus tertius, which function primarily to turn the foot outward (evert) and point the footdown (plantar flex). The peroneal tendons run behind the prominent bone on the outside of the ankle. Thesetendons help to control the position of the foot and ankle during walking.Peroneal tendon disorders are a common cause of ankle pain in active patients. Commonly associated with lateralankle sprains, other causes of pain along these tendons can also be due to functional ankle instability, subluxationof the peroneal tendons, insufficiency behind the prominent bone on the outside of the ankle, low lying fibularisbrevis muscle, cavus foot (high arch) posture, and/or tearing along the tendons. As there are many factorsassociated with peroneal tendon disorders, when conservative management fails to improve symptoms, surgeryoften becomes an option which, ideally, is followed by an appropriately tailored rehabilitation program for optimalrecovery and (early) return to sports.Peroneal surgery is followed by both Non-Weight-Bearing (NWB) immobilization and Weight-Bearing (WB)immobilization to facilitate optimal healing while preventing re-injury. Early range of motion (ROM) is commonlyrecommended based on the concept that tendons tend to form adhesions between the repaired tissue andsurrounding scar tissue after surgical repair. In peroneal tendon injuries, timing and progression to full weightbearing depends on both the nature of the pathology as well as the type of treatment (conservative, tendoscopic, oropen—with or without repair of the superior peroneal retinaculum).This was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospitaland should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.
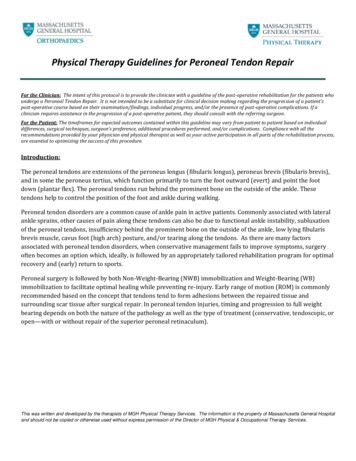
Physical Therapy Guidelines for Peroneal Tendon RepairFigure 1: Anatomy of Peroneal TendonsTreatment:Acute peroneal tendon injuries have been reported to occur up to 95% in patients with lateral ankle sprains.Tendinosis of the peroneal tendons due to a high arch (cavus) foot posture, separate from ankle sprains, is also acommon cause of injury and dysfunction. Due to these injuries, tears frequently occur longitudinally, resulting fromsubluxation or movement along the lateral malleoli, mainly due to repetitive damage or acute trauma. Conservativemanagement focusing on impairment-based treatments may improve function. It should be noted that currenttreatment guidelines are primarily based on expert opinion due to the lack of clinical trials. In the case of tendonsubluxation, surgery is usually recommended as casting and immobilization has not been shown to improvestability of the tendons.Non-operative Treatment:Treatment for peroneal tendinopathy, include but are not limited to, targeting ankle eversion and plantarflexionstrength while maintaining appropriate foot and ankle mobility with concurrent gastroc-soleus stretching, ankleand lower extremity mobilizations and manipulations, and balance/proprioceptive training. It is common practiceto incorporate non-weight bearing and full weight bearing exercise as pain allows, while progressing from stable tounstable surface training. The use of orthotics to improve loading of the peroneal tendons to reduce strain andstress through the tendons may also be helpful. The goal is to reduce excessive peroneal stress while maximizingtotal ankle range of motion, strength, and sensorimotor functionOperative Treatment:Surgical treatment and repair of the peroneal tendons vary based on the nature of the pathology, particularly, thestatus of the superior peroneal retinaculum (SPR). Surgical treatment may include tendoscopic or open - with orwithout repair of the superior peroneal retinaculum. When the SPR is not repaired, rehabilitation initially focuseson early mobilizations and ROM in all planes given the lack of opening of the peroneal tendons proximal to the tipof the fibula. Non-weight bearing immobilization is about 2 weeks and immobilization period no longer than 4weeks is recommended when the SPR remains undisturbed. When the SPR is repaired, immobilization includesnon-weight bearing in a lower leg cast for 2 weeks, followed by 4-6 weeks of progressive weight bearing in awalker boot to ensure that the tendons do not dislocate and the SPR repair can heal.This was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospitaland should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.
Physical Therapy Guidelines for Peroneal Tendon RepairTendoscopic or open repair with or without repair of the superior peroneal retinaculumPhasePre-operativePost-operative:Days 0-2 weeksRestrictions and PrecautionsN/ANWB in lower leg splint for 2 daysfollowed by NWB in lower leg castfor 12 daysPhysical Therapy TreatmentGoals-Instruct with use of assistive devicebased on gait assessment, non-weightbearing (NWB) on affected side-Demonstrate safe ambulationwith assistive device NWB-Edema management-Manage pain and swelling-Gait training and safety (emphasizeprecautions with weight bearing)-Demonstrate safe ambulationwith assistive device NWB-Education/modifications for ADLs-Able to maintain NWB withtransfers and stairs-Able to maintain NWB withtransfers and stairs-Perform activities of daily living(ADLs) in a modifiedindependent manner or withminimal assistance2-4 weeksPrecautions based on SPRrepaired vs. non-repaired, seebelow-Modalities and patient education tocontrol swelling-Electric stimulation can be used toprevent muscle atrophy and for painmanagement (low intensity, highfrequency)-Once incision healed, scarmobilization/massage, modified asnecessary to avoid strain on thehealing SPR-Intrinsic foot strengthening-Manage pain and swelling-Increase range of motion of footand ankle- Demonstrate safe use ofassistive device and begin partialWB-Minimize the loss of strength inthe core, hips, and knees-Independence with homeexercise program to beperformed daily- Strengthening for core, hips, knees(maintain precautions)-NWB fitness/cardiovascular exercises(i.e. bicycle with one leg)-Use Alter-G treadmill, if available, toinitiate walking with partial WBThis was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospitaland should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.
Physical Therapy Guidelines for Peroneal Tendon RepairTendoscopic or open repair with or without repair of the superior peroneal retinaculumPhaseRestrictions and PrecautionsPhysical Therapy TreatmentGoalsrestriction-Begin partial progressive WB in awalker boot or lower leg cast withassistive device if SPR is NOTrepairedIf SPR is NOT repaired:-Begin AROM Exercises and hands-ontechniques (by the PT) for foot andankle range of motion into plantarflexion (PF), dorsiflexion (DF),inversion, eversion in NWB- Begin partial progressive WB in awalker boot or lower leg cast withassistive device (as recommended bythe surgeon)4-8 weeks-If repair of the superiorperoneal retinaculum (SPR) isperformed, immobilizationshould consist of 2 weeks NWB ina lower leg cast, followed by 4-6weeks of progressive partial WBimmobilization in a walker bootwith NO inversion/eversion for6 weeksIf SPR is repaired:-begin AROM as above, avoidinginversion/eversion for 6 weekspost-op-4-6 weeks: Full WB (based onsurgeon recommendation) by 4-6weeks with assistive device asneeded if SPR is NOT repairedIf SPR is NOT repaired:-Begin isometric, concentric andeccentric exercise (may begin use oflight resistance with eversion againsttherapist) with isotonics, andproprioceptive training seated or on 2legs- Begin partial progressive WB in awalker boot or lower leg cast withassistive device (if recommended bythe surgeon)-Gradually progress from partial WB tofull WB (as recommended by thesurgeon), consider walking inswimming pool if available-Increase ROM of ankle and foot-Improve calf strength and footintrinsic strength-Minimize loss of strength incore, hips and knees-Facilitate gradual return to WB-Restore gait with use of assistivedevice as needed-Continue use Alter-G trainer,progressing to full WB-Can begin use of stationary bike-Wean from boot (6-8 weeks/ asrecommended by the surgeon)This was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospitaland should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.
Physical Therapy Guidelines for Peroneal Tendon RepairTendoscopic or open repair with or without repair of the superior peroneal retinaculumPhaseRestrictions and PrecautionsPhysical Therapy TreatmentGoals-Manual therapy for joint mobilizationsas indicated for the talocrural, subtalarjoint, forefoot and metatarsals-6-8 weeks: If SPR is repaired,continue progressive partial WBgradually progressing to FWB(only if recommended by thesurgeon) with assistive device asneededIf SPR is repaired:-Continue ankle AROM exercise andseated foot/ankle exercise whilemaintaining motion and weightbearing precautions (noinversion/eversion until after postop week 6; no standing exercisewithout boot)-Begin isometric, concentric, andeccentric exercise (may begin use oflight resistance with eversion againsttherapist) after 6 weeks-Progress WB from Progressive PWB toFWB (6-8 weeks) as recommended bythe surgeon-Wean from boot, if appropriate8-12 weeks- If SPR is repaired: Attain FWB ifnot already achieved-Continue all concentric/eccentric,isotonic exercises-Full range of motion foot andankle in all planes-Avoid high impact/pivoting – norunning-Wean from the boot in 8-10 weeks (asrecommended by the surgeon) if notalready weaned off, if SPR is repaired-Restore proximalstrength/control of the core, hipand knee where applicable-Initiate eccentric gastrocnemiusstrengthening off step/ledge-Proprioceptive exercises once fullweight bearing without boot: unstablesurfaces including foam, wobble board,BOSU ball, trampoline, and Dyna Discs-Gradually return to regularfunctional activities (exceptsports and sport relatedactivities) if ROM, strength, andgait goals have been met-Progress activity from double leg tosingle leg (only if pain-free and able todemonstrate good stability on doubleleg stable and unstable surfaces) onstable surfaces to unstable surfacesThis was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospitaland should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.
Physical Therapy Guidelines for Peroneal Tendon RepairTendoscopic or open repair with or without repair of the superior peroneal retinaculumPhase12-24 weeksRestrictions and Precautions-Can begin return to run with awalk/jog interval program if fullAROM and strength has beenachieved (once cleared by thesurgeon)-If able to run and perform allactivity without pain, may beginsport specific training, otherwisehold off until above is achievedPhysical Therapy TreatmentGoals- Continue proprioceptive exercise onsingle leg on stable surfaces to unstablesurfaces-Full strength of lower extremitymuscles-Progress dynamic WB exercise toinclude lateral mobility to engageperoneal tendons including speedskaters, use of slide board, lateral stepups/downs-Begin with bilateral plyometricsworking towards unilateralplyometrics as tolerated 24 weeks-Running-Sport Specific Training-Provocation of peroneal tendons-Progress unilateral plyometrics intosport specific drills-Sport specific training andconditioning (progress to high impactif applicable as tolerated once clearedby surgeon)-Gradually return to regularfunctional activities-Encourage activation alongperoneal tendons to facilitateappropriate healing-Improve endurance andperformance to minimize risk ofre-injury-Gradual return to activities withmulti-planar movements onuneven outdoor surfaces-Gradual return to high impactsports that include jogging,running, and jumpingFunctional Screening Tests:-Side-hop-6-meter Crossover Hop-Square Hop-Figure-of-8 hopFunctional Tests for Return to Sport:1. Timed lateral step-down2. Timed leap and catch hop sequence3. Single-leg hop for distance4. Single-leg timed hop5. Single-leg triple hop for distance6. Crossover hop for distanceendurance sequence7. Square hop test8. Lower Extremity Functional Test(LEFT)This was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospitaland should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.
Physical Therapy Guidelines for Peroneal Tendon RepairIf you have any questions or concerns related to the content of these rehabilitation guidelines, please contact:MGH Physical and Occupational Therapy Services (Mass General Waltham)781-487-3800Website: ical-and-occupational-therapyMGH Orthopedics Foot and Ankle617-724-9338Website: eReferences : Van Dijk PAD, Lubberts B, Verheul C, DiGiovanni CW, Kerkhoffs GMMJ. Rehabilitation after surgical treatmentof peroneal tendon tears and ruptures. Knee Surg Sports Trumatol Arthrsoc. January 2016:1165-1174.doi:10.1007/s00167-015-3944-6. Van Dijk PAD, Tanriover A M.D, DiGiovanni CW M.D., Waryasz GR M.D. Immobilization and Rehabilitation afterSurgical Treatment of the Peroneal Tendons https://footeducation.com/peroneal-tendonitis/ van Dijk PA, Miller D, Calder J, et al. The ESSKA-AFAS international consensus statement on peronealtendon pathologies. Knee Surg Sports Traumatol Arthrosc. 2018;epub ahead of print e/conditions-and-treatments/peroneal-tearsThis was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospitaland should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.
Physical Therapy Guidelines for Peroneal Tendon Repair This was written and developed by the therapists of MGH Physical Therapy Services. The information is the property of Massachusetts General Hospital and should not be copied or otherwise used without express permission of the Director of MGH Physical & Occupational Therapy Services.











