Transcription
SportsPhysical TherapyDescription ofSpecialty PracticeN BOARDICAOERMLIASICALTIEP HYSFASpecialty Council onSports Physical TherapyT HE R A P Y S P ECAmeric an Board of Physica l Ther a p y Sp ecia lties
SportsPhysical TherapyDescription ofSpecialty PracticeN BOARDICAOERMLIASICALTIEP HYSFASpecialty Council onSports Physical TherapyT HE R A P Y S P ECAmeric an Board of Physica l Ther a p y Sp ecia lties
Sports Physical TherapyAcknowledgementsThe Sports Physical Therapy Description of Specialty Practice was prepared by the members of a subject matter expert (SME) group and members of the Sports PhysicalTherapy Specialty Council and approved by the American Board of Physical TherapySpecialties (ABPTS), American Physical Therapy Association.Specialty CouncilChairs: E dward Mulligan, PT, DPT, OCS, SCS, ATC, andMichael Rosenthal, PT, DSc, ECS, SCSTeresa Schuemann, PT, DPT, SCS, ATC, CSCSBarbara Springer, PT, PhD, OCS, SCSPatrick Pabian, PT, DPT, SCS, OCSSubject Matter ExpertsMichael Fink, PT, DSc, OCS, SCSMatthew Briggs, PT, DPT, ATC, SCSMark Weber, PT, PhD, SCS, ATCProject CoordinatorEdward Mulligan, PT, DPT, OCS, SCS, ATCConsultantMark Reinking, PT, PhD, ATC, SCSThroughout this document, the editors have attempted to use language consistent withthe Guide to Physical Therapist Practice and universally accepted concepts and terminology, without bias to any particular philosophy or school of thought. The referencescited with the case scenarios are given only to help the reader understand the specificexamples and are not intended to bias any particular school of thought or philosophy.In addition, these references are not intended to be inclusive.American Board of Physical Therapy Specialties Specialty Council on SportsPhysical Therapy (ABPTS LOGO)N BOARDICAOERMP HYSFAThe Specialty Council on Sports Physical Therapy encourages your suggestions forimprovement of this document. Your input and suggestions will be considered in thedevelopment of the next revision. This is a working document and will be modified asnecessary.LIASILTIE 2013, 2002, 1997, 1993 by the American Physical TherapyAssociation. All rights reserved. No part of this document may be reproduced in any form or by any electronic or mechanical means, including informationstorage and retrieval systems, without written permission of the publisher.CAT HE R A P Y S P ECFor more information about this or any other APTA publication, contact the AmericanPhysical Therapy Association, 1111 North Fairfax Street, Alexandria, VA 22314-1488,800/999-APTA (2782), or www.apta.org. [Order No. E-28]ii
Table of ContentsIntroduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2Chapter 1: escription of Sports Physical TherapyDBoard-Certified Specialist Respondents. . . . . . . . . . . . . . . . . . . . . . . . 4Chapter 2:Description of Board-Certified Specialty Practice in Sports . . . . . . . . 8Chapter 3: Case Scenarios. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Chapter 4:Examination Content. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23Chapter 5:Executive Summary . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 241
Sports Physical TherapyIntroductionSpecialist certification was established to provide formal recognition for physical therapists with advanced clinical knowledge,experience, and skills in a defined area of practice. Certificationis achieved through the successful completion of a standardizedapplication and examination process.History of Specialization in Physical Therapy1975, the House of Delegates of the American PhysicalTherapy Association (APTA) approved the concept of specialization and created the Task Force on Clinical Specialization.The task force was charged with identifying and definingphysical therapy specialty practice areas and with developingthe structure for and function of a board-certified process.Specialist certification was established to provide formalrecognition for physical therapists with advanced clinicalknowledge, experience, and skills in a defined area of practice.Certification is achieved through the successful completion ofa standardized application and examination process.The document developed by the task force, Essentials forCertification of Advanced Clinical Competence in PhysicalTherapy, was adopted by the House of Delegates in 1978. Atthat time, the House recognized 4 specialty areas: cardiovascular/pulmonary, neurology, orthopedics, and pediatrics. In 1979, theHouse appointed the Commission for Certification of AdvancedClinical Competence. Specialty councils for each of the 4 specialty areas were appointed and charged with the development ofcompetencies unique to each area of advanced clinical practice.In 1980, the commission became the Board of Certificationof Advanced Clinical Competencies (BCACC). The Houseof Delegates recognized 2 additional specialty areas in thesame year: sports and clinical electrophysiology. The Houseof Delegates revised Essentials for Certification of AdvancedClinical Competence in Physical Therapy in 1985, and thename was changed to Essentials for Certification of PhysicalTherapist Specialists. The BCACC was renamed the AmericanBoard of Physical Therapy Specialists (ABPTS), and the first specialty examination was administered in cardiovascular/pulmonaryphysical therapy that same year. The specialty area of geriatricswas approved in 1989. In June 2006, the House of Delegatesapproved women’s health as the newest area of physical therapistspecialist practice.2History of Specialization in Sports Physical TherapyThe Sports Physical Therapy Section began work on the development of the initial advanced competencies in the mid 1970s. Acompetency committee performed a task analysis between 1978and 1979 in order to identify the clinical task(s) in which competency is essential to practice sports physical therapy and to determine to what extent Sports Physical Therapy Section memberswere practicing those tasks. The results of the initial task analysiswere published by Skovly in 1980.1 From this study, 18 competency statements were developed. Fifteen of those statementsconcerned clinical skills; the other 3 concerned administration,education, and research.The Sports Physical Therapy Section initially petitioned theBoard for Certification of Advanced Clinical Competence forrecognition as a specialty area in 1981. The American PhysicalTherapy Association House of Delegates approved sports physicaltherapy as an area of specialization that same year.2Following approval as an area of specialization, a second majorstudy was conducted to clarify initial task analysis results. Thepurpose of this second study was to validate the original competency statements. The validation study completed by Krugh3determined the level of preparation at entry into the profession to perform the advanced competencies and the level ofimportance of each of these statements to the practice of sportsphysical therapy.The American Board of Physical Therapy Specialties requires thateach specialty area revalidate its competencies at least every 10years to assess if there is any change in the scope of practice. In1991, a revalidation study was initiated. Completed in 1992, thisstudy identified 30 different competency statements in 9 different areas. The new Sports Physical Therapy Description of AdvancedClinical Practice was developed and approved by ABPTS in 1994.The first edition of the Guide to Physical Therapist Practice waspublished in 1997.4 This document was designed to describephysical therapy practice in the context of the Nagi disablement model. The Guide describes the patient/client management model as including patient/client examination, evaluation,diagnosis, prognosis, intervention, and outcomes. The Guidealso standardizes terminology used in physical therapy practice,and describes preferred practice patterns in four categories ofconditions: musculoskeletal, neuromuscular, cardiovascular/pulmonary, and integumentary. A second edition of the Guide waspublished in 2001.5
Description of Specialty PracticeIn 2001, a third revalidation study of specialty practice in sportsphysical therapy was initiated. The purposes of this study were toassess the currency of the competency statements regarding thepractice of sports physical therapy and to ensure that the updatedSports Physical Therapy Description of Specialty Practice (DSP) wasconsistent with the Guide to Physical Therapist Practice, 2ndEdition.5 A group of experts in sports physical therapy convenedin 2001 to create a survey instrument. This survey was pilot testedand revised, and the final survey was distributed in summer 2002.A second meeting of subject-matter experts occurred in the springof 2003 to discuss the results of the survey and to rewrite the DSP.This document is a result of a fourth revalidation study of thespecialty practice in sports physical therapy that was initiated in2010 and approved by ABPTS in 2013.References1. Skovly R, Davies G, Mangine R, Mansell R, Wallace L. Results of the task analysis study,Sports Physical Therapy Section, American Physical Therapy Association. J Ortho Sports PhysTher. 1980;1:229-238.2. American Physical Therapy Association House of Delegates. Sports Physical TherapySpecialization. HOD 06-81-15-54. Alexandria, VA: American Physical Therapy House ofDelegates; 1981.3. Krugh J. Advanced clinical competencies for the sports physical therapists. Chapel Hill, NC:University of North Carolina – Chapel Hill; 1984. Unpublished thesis.4. Guide to Physical Therapist Practice. Phys Ther. 1997;77:1163-1650.5. Guide to Physical Therapist Practice. 2nd ed. Phys Ther. 2001;81:9-744.3
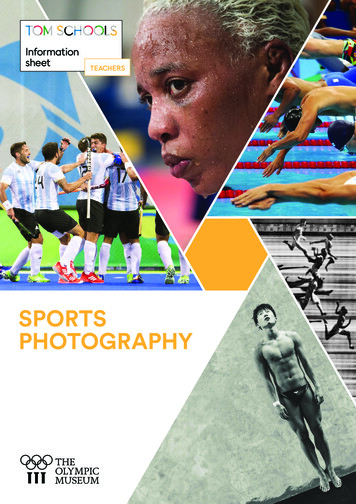
Sports Physical TherapyChapter 1: Description of Sports Physical Therapy Board-Certified Specialist RespondentsThe following figures contain the descriptive demographic information of the 259 survey respondents who indicated they wereboard-certified sports clinical specialists. While the American Board of Physical Therapy Specialties collects similar data on all newlyboard-certified or recertified specialists, this demographic data represents those who responded to the practice analysis survey.Figure 1. Current AgeFigure 2. Sex4Figure 3. EthnicityFigure 4. Highest Earned Professional Degree
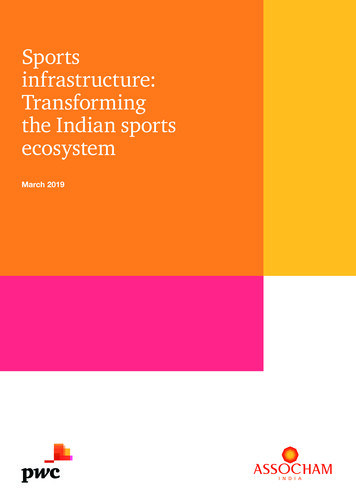
Description of Specialty PracticeFigure 5. Highest Earned Academic DegreeFigure 7. Type of Practice FacilityFigure 6. Years of Practice in Physical TherapyFigure 8. Median Percentage of Time Spent in ProfessionalActivities5
Sports Physical TherapyFigure 9. Provides Services in Athletic VenuesFigure 11. Respondents Who Completed a Credentialed SportsPhysical Therapy ResidencyFigure 10. Sport Category in Which Specialists Provide AthleticVenue ServicesFigure 12. Respondents Who Have Additional Certifications*65%20%10%6
Description of Specialty PracticeFigure 13. The 3 Most Common Additional CertificationsFigure 15. Referral SourcesFigure 14. Patients/Clients Treated Per DayFigure 16. Geographic Representation of Respondents7
Sports Physical TherapyChapter 2: Description of Board-Certified SpecialtyPractice in SportsThis Description of Specialty Practice (DSP) describes the practiceof board-certified sports physical therapy clinical specialists. It isbased on survey responses of 414 participants: 259 board-certifiedsports clinical specialists, 35 members of the Sports Physical TherapySection of APTA who are not specialists, and 120 physical therapistswho did not indicate their specialist status. The process of revalidationof the DSP is conducted every 10 years, and the last revision of theSports DSP was published in 2002.1 Weber et al2 described the detailof that practice analysis process.Specialty board certification is one mechanism to stimulate thedevelopment of expert practice in physical therapy. Expert cliniciansdemonstrate different reasoning processes from novices, based ontheir knowledge, experience, and reflective behaviors.3-7 This refinement in reasoning skills and patient management should result ingreater efficiency and effectiveness in providing patient care in theirarea of specialization. This has been shown to be the case in a groupof orthopedic clinical specialists.8The patient/client management model described in the Guide toPhysical Therapist Practice9 is the accepted standard for physical therapist practice, including sports physical therapy specialty practice. ThisDSP highlights the specific components of physical therapist practicethat sports clinical specialists use, based on the perceptions of thesurvey respondents and a group of subject matter experts. As sportsphysical therapy specialty practice is a subset of physical therapistpractice, this DSP does not include all of the practice areas coveredin the Guide.The foundation of sports physical therapy specialty practice requiresa comprehensive declarative and procedural knowledge for practice.This foundational knowledge and practice is critical to the development of advanced clinical competence. These knowledge and practicecontent areas include the following: Movement Science–– Biomechanics and kinesiology–– Motor learning and control–– Gait (walking and running) and locomotion Pathology and Pathophysiology–– Symptoms/signs of injury/disease–– Disease epidemiology–– Inflammation, tissue healing, and repair–– Pathomechanics Medical and Surgical Intervention–– Imaging studies (eg, plain radiographs, bone scan,MRI, US, CT)–– Ancillary tests (eg, EMG, EKG, lab studies)–– Pharmacology–– Surgical procedures Health and Wellness–– Nutrition–– Psychological issues relating to performanceand injury–– Basic parameters of fitness Critical Inquiry–– Research design and methods, includingstatistical concepts–– Research findings specific to sports physicaltherapy practiceFoundational Practice Ethical conduct in practice and researchFoundational Knowledge Human Anatomy and Physiology–– Musculoskeletal system–– Neuromuscular system–– Cardiovascular and pulmonary systems–– lntegumentary systems–– Other systems: endocrine, reproductive,and digestive–– Histology (eg, connective tissue, muscle,nerve, bone)–– Physiology of exercise and sport-specificphysiological demands8 Legal compliance, including scope of practice Administration and management principles in practiceAdvanced practice in sports physical therapy requires certainknowledge, skills, and behaviors. In this document, the term“athlete” should be understood to indicate physically active individuals who span the spectrum across age, race/ethnicity, illness orinjury condition, and level of ability/disability. Based on participant responses to the practice survey and the opinions of a panelof subject-matter experts, key competencies were modified andreorganized to reflect contemporary sports specialty practice. Thepractice expectations of a sports clinical specialist have been organized below into 6 competency areas. Each competency area isfurther subdivided into specific professional behavioral objectives.
Description of Specialty PracticeI. Rehabilitation/Return to SportsThese activities of the board-certified sports specialist areconcerned with the rehabilitation of athletes with impairments, activity limitations, or participation restrictionfocus on the return of athletes to their sport activities.Such activities include:A. Examination, Evaluation, and Diagnosis1. Examine, evaluate, and diagnose consideringsport-specific injury epidemiology (incidence/prevalence), sports-specific biomechanicaldemands, comorbidities, and other identifiedrisk factors2. Identify history of athlete’s major complaint(s)with regard to severity, chronicity, impairment,activity limitations, participation restrictions,level of irritability/severity, previous therapeuticinterventions, and emotional response to currentcondition3. Perform systems review to assess physiologic andanatomic status, cognition, and communicationskills4. Select functional outcome measures to determinebaseline status and assess response to intervention5. Select and perform tests and measures that arecomprehensive and consistent with history andsystems review to include but are not limited to:a) Aerobic capacity/endurance (eg, treadmill/ergometer submaximal and maximal stresstesting)b) Anthropometric characteristics (eg, bodycomposition, body dimensions—height,weight, girth, edema)c) Arousal, attention, and cognition (eg,assessment of factors that influence motivation level, levels of consciousness)d) Assistive and adaptive devices (eg, assessment of appropriateness, alignment andfit, safety)e) Circulation (eg, pulses, vertebral arteryexamination, screen for circulatoryabnormalities)f) Cranial nerve integrityg) Peripheral nerve integrityh) Environmental considerations (eg, weather,altitude, venue conditions)i)Assessment of sport-specific biomechanics(eg, kinetic, kinematic, task analysis)j)Gait and locomotion (eg, running andwalking analysis)k) Static and dynamic balance (eg, sportspecific movements)l)Integumentary integrity (eg, skin characteristics, wound assessment, characteristics ofinfectious agents)m) Joint integrity and mobility (eg, assessment of abnormal joint mobility includingpassive range of motion, joint play movements, response to manual provocation)n) Motor function (eg, motor control, motorlearning)o) Muscle performance (eg, instrumented andnon-instrumented strength, power, andendurance assessments, sport-specific functional muscle testing)p) Neural mobility (eg, neural limbtension tests)q) Orthotic, protective, and supportivedevices (eg, assessment of appropriateness,remediation of impairment, athletic equipment alignment and fit, safety)r)Pain, fear avoidance, and kinesiophobiaassessments)Posture (eg, body or body segment(s)structure, alignment, changes in differentpositions, body contours)t)Prosthetic devices (eg, assessment of appropriateness, compliance, remediation ofimpairment, alignment and fit, safety)u) Range of motion including muscle lengthv) Reflex integrity (eg, assessment of normaland pathological reflexes)w) Sensory integration (eg, assessment ofdexterity, coordination, and integration ofsomatosensory, audiovisual, and vestibularsystems)x) Ventilation and respiration/gas exchange(eg, breathing patterns, chest wallmobility, perceived exertion, pulmonaryfunction testing)6. Sequence tests and measures appropriately basedon athlete’s condition7. Recognize strengths or limitations of tests andmeasures based on measurement propertiesof sensitivity, specificity, likelihood ratio, validity,and reliability8. Evaluate and interpret all examination data9. Organize data into recognized clusters, syndromes, or pathoanatomical categories, basedon the examination9
Sports Physical Therapy10. Establish a physical therapy diagnosis includingnature of complaint, probable cause, anatomicalstructures involved and stage of the condition11. Identify possible conditions that requireconsultation with or referral to another healthcare provider12. Recognize appropriate imaging and laboratorytests for the injured athlete; recommend appropriate tests in consultation with other healthcare professionals; understand limitations, indications, and contraindications of these tests; andinterpret these tests in consultation with otherhealth care professionalsB. Prognosis, Intervention, and Outcomes1. Prognosisa) Determine appropriateness of physicaltherapy intervention, including need forreferral to other health care professionalf) Select and apply appropriate orthotic orsupportive devices to minimize acuity ofinjury and facilitate recovery and returnto sportg) Adapt/adjust sports participation andrehabilitation based on disability considerations including prosthetic and adaptiveequipment use3. Procedural Interventionsa) Therapeutic exercise instruction toimprove muscle performance, jointmobility, muscle length, and aerobiccapacity/enduranceb) Establish a prognosis including theexpected level of improvement in functionand the amount of time needed to reachthat levelb) Motor function training (eg, balance,coordination and agility training, bodymechanics and postural stabilization, gait,locomotion training)c) Respond to emerging data from reexamination and response to interventions bymodification and redirection of intervention as neededc) Muscle performance training (eg,strength, power, and endurance training)d) Select validated functional outcome tools,when available, to determine initial andlong-term responses to interventione) Manual therapy techniques, includingjoint mobilization and manipulatione) Determine the extent of injury and possible sequelae to appropriately determinewhether the athlete has the ability tocontinue participation without incurringfurther injury2. Intervention Planninga) Design comprehensive intervention program to safely return the athlete whileminimizing the risk of reinjuryd) Aerobic capacity/endurance conditioningand reconditioningf) Passive range of motiong) Soft tissue mobilization (eg, therapeuticmassage, connective tissue massage, deepfriction, cross friction) and manual therapy (eg, manual traction, mobilization/manipulation, passive range of motion)h) Electrotherapeutic modalities (eg, biofeedback, high-volt stimulation, interferentialcurrent, TENS, iontophoresis, functionaland neuromuscular electrical stimulation)b) Select and prioritize specific interventionsbased on impairments, activity limitations, and participation restrictionsi)Physical agents (eg, ultrasound, cryotherapy, deep thermal, hydrotherapy, superficialthermal)c) Develop and implement sport-specific,performance-based functional progressionprogramsj)Functional training in sport activityd) Implement functional tests to determineathlete’s ability and readiness to return tosports activitiese) Perform appropriate measurements of themusculoskeletal, cardiovascular/pulmo10nary, integumentary, and neuromuscularsystems to determine the athlete’s status,progress, and required modifications inthe rehabilitative programk) Prescription, application, and/or fabrication of prosthetic, orthotic, protective,and supportive devices and adaptiveequipmentl)Integumentary repair and protection
Description of Specialty Practice4. Educational Interventionsa) Counsel athletes, parents, coaches, andadministration regarding safe return tosportb) Patient/client education on diagnosis,prognosis, intervention, responsibility, andself-management within plan of care5. Outcomesa) Determine and implement sport-specificcriteria and recommendations regardingthe athlete’s readiness to return to sportb) Recommend level of athlete’s sports participation based on results of sport-specifictestingc) Remediate athlete’s sports and daily living limitations based on best availableevidence and athletic variables (eg, history,diagnosis, complications, sporting activity)i)Integumentary injuries (eg, lacerations,abrasions, nail bed injuries)j)Genitourinary injuries (eg, testicular torsion, direct trauma)2. Knowledge of venue-specific emergency actionplanB. Prognosis, Intervention, and Outcomes1. Use published criteria for return to sport, whenavailable, to make return-to-sport decisions2. Determine if the athlete can return to sportbased on information obtained during theinitial and subsequent evaluations and onlegal standards3. Provide emergency care, management of injury,and transport as necessary4. Advise parents, coaches, and administrationas to the signs and symptoms of a worseningcondition if athlete is not referred for medicalor psychological evaluation5. Inform athletes, parents, coaches, and administration of the return-to-sport criteriaII. Management of Acute Injury/IllnessThese activities of the board-certified sports specialist areconcerned with the immediate management of acute injury or illness associated with athletic activity. Such activitiesinclude:A. Examination, Evaluation, and Diagnosis1. Recognize acute injuries and illnesses thatrequire immediate medical intervention, andmake appropriate decisions regarding emergencycare for the following conditions:a) Cervical, thoracic, and lumbarspine injuriesb) Head and facial injuries (eg, concussion,eye, maxillofacial, ear)c) Environmental injuries (eg, cold, heat,altitude, lightning)d) Musculoskeletal injuries(eg, fractures,dislocations)e) Abdominal organ injuries (eg, spleenrupture, liver laceration)f) Pulmonary conditions (eg, pneumothorax, hemothorax, status asthmaticus)III. Medical/Surgical ConsiderationsThese activities of the board-certified sports specialist areconcerned with the medical and surgical management ofathletes. Such activities, performed in concert with otherhealth care professionals, include:A. Examination, Evaluation, and Diagnosis1. Correlate clinical findings with imaging studiesand ancillary tests (eg, lab tests, EMG, NCV,EKG) performed2. Evaluate an athlete’s metabolic and physiologicresponses to viral and bacteriological diseases,including gastrointestinal, cardiovascular andpulmonary, endocrine, genitourinary, and dermatological conditions3. Evaluate an athlete with consideration of existing injury/illnesses (eg, asthma, diabetes, femaletriad, GI disorders, hypertension)4. Design and evaluate rehabilitation programsbased on the goals and principles of surgicaltechniques for athletic injuries within the indications and contraindications of the surgicaltechniquesg) Cardiovascular conditions (eg, dysrhythmias, sickle cell traits, hypertrophic cardiomyopathy, myocardial infarction, commotio cordis)h) Anaphylaxis11
Sports Physical TherapyB. Prognosis, Intervention, and Outcomes1. Provide management and, as needed, return-tosport recommendations for athletes presentingwith existing medical conditions (eg, asthma,diabetes, hypertension, infectious disease, integumentary, female triad, GI disorders)2. Assess athlete’s adherence to established illnessmanagement plan3. Refer to other health care professionalsas needed for reassessment of establishedmanagement plan4. Counsel athletes, parents, coaches, and administrators as to the impact of pharmacokinetics andpharmacodynamics on the athlete and his/herparticipation in athletics5. Counsel athletes, parents, and coaches as to themedical/surgical considerations and the impacton the athlete’s current and future participationin athletics6. Counsel athletes, parents, and coaches regardingthe interventions for various infectious diseases,including interventions for preventing the spreadof disease among team members3.4.5.6.7.other areas that affect the health and well-beingof athletesProvide recommendations on lifestyle andactivity modifications for athletes with chronicconditions (eg, female athlete triad, diabetes,asthma, hypertension)Design and conduct preventive conditioningprograms for in-season and off-season based onthe individual athlete’s needs and sport demandsImplement measures to maximize participant/spectator safety in environmentally stressfulconditions (eg, lightning risk, acclimatization,appropriate clothing, hydration, nutritionalstrategies to avoid heat or cold injuries)Educate athletes, parents, coaches, and administrators on injury prevention and potentialsafety risksSelect, fit, and maintain appropriate sportspecific equipment in recognition and acceptance of National Operating Committee onStandards for Athletic Equipment (NOCSAE)V. Sports Performance EnhancementIV. Injury PreventionThese activities of the board-certified sports specialist areconcerned with injury/disease prevention for athletes. Suchactivities include:A. Examination, Evaluation, and Diagnosis1. Plan, coordinate, and/or administer preparticipation physical examinations for the purpose ofscreening for and recognizing medical conditionsor injuries that might affect or preclude the athlete’s participation2. Perform systems review and screening examination for possible medical conditions includingbut not limited to cardiac, metabolic, pulmonary, and female triad issues3. Assess sport-specific fitness status (eg, aerobic oranaerobic capacity, endurance, acceleration andpower, muscle performance, range of motion,balance/proprioception, movement analysis)4. Monitor environmental conditions and promptly determine the impact of the conditions on theparticipant and spectator safetyB. Prognosis, Intervention, and Outcomes1. Design and implement sport-specifictraining programs2. Educate athletes, parents, coaches, and administrators regarding appropriate training principles,participation, physical limitations, equipment, or12These activities of the board-certified sports specialist areconcerned with maximizing the athlete’s sport performance, including training considerations and the effect ofsuch factors as nutrition and environment on performance.Such activities include:A. Examination, Evaluation, and Diagnosis1. Assess human performance (eg, testing and measuring speed, acceleration, VO2max, power, andother performance indicators)2. Interpret human performance assessment todesign an appropriate conditioning program3. Develop and implement rehabilitation programsdesigned to enhance overall human performanceand sports specificity4. Evaluate environmental conditions, determinethe effect the conditions will have on performance, and modify athletic performanceaccordinglyB. Prognosis, Intervention, and Outcomes1. Develop rehabilitation and performanceenhancement guidelines and timelines basedon the science supported within the literature2. Educate and counsel athletes, parents, coaches,and administrators on sports nutrition issuesincluding:a) Macro and micronutrients and dietarysupplements
b) Appropriate hydration strategies for pre-,during, and post-training or competition3. Identify the administrative oversight necessaryfor assessment of equipment and facility safety(eg, protective gear, field and venue safety)4. Develop departmental policies and procedures(eg,
Sports Physical Therapy Section, American Physical Therapy Association. J Ortho Sports Phys Ther. 1980;1:229-238. 2.American Physical Therapy Association House of Delegates. Sports Physical Therapy Specialization. HOD 06-81-15-54. Alexandria, VA: American Physical Therapy House of Delegates; 1981. 3.