Transcription
MD Anderson Cancer Center at CooperANNUAL REPORT2013
Two Cooper Plaza, 400 Haddon AvenueCamden, NJ 08103Dear Friend,Today, people use the word “groundbreaking” so frequently that its definition has beendiminished. But I can say without qualification that 2013 was truly a groundbreaking yearfor our cancer program.In 2013 we made meaningful advances in furthering our mission to conquer cancer. Early in the year, we began a major restructuring of our administrative leadership anddeveloped a new model for the organization and operations of our clinical services. We developed a strategic playbook that will help us grow stronger, smarter and moreefficiently – while keeping our patients at the forefront of all we do. We embarked on a new electronic medical records system and new treatmentinformation management systems. In September, we launched our partnership with The University of Texas MD AndersonCancer Center – the nation’s leading cancer hospital – and embraced a new name andbrand identity. In October, we opened a new, state-of-the-art cancer center on the Cooper Health SciencesCampus in Camden where we care for more than 100 patients a day. We renovated and enhanced cancer services at the Cooper Voorhees Campus with addeddiagnostic imaging capabilities and the addition of a second linear accelerator for thedelivery of radiation treatment. We welcomed new, exceptional physicians and surgeons to our team and broadened ouroffering of clinical programs and treatment options. We expanded our reach – opening more outpatient offices to provide easier access to carefor our patients. We unveiled an aggressive new marketing campaign to get the word out about ouroutstanding programs and services to the residents of South Jersey and beyond. And, as the year came to a close, we initiated our first Phase 1 Clinical Trial to study theefficacy of a new cancer treatment option.It has been an exciting year, one filled with great accomplishments as well as immensepersonal and professional satisfaction for the members of the MD Anderson Cancer Centerat Cooper team. But there is still much work to be done. In the year ahead we will build onthe new foundation that we created this year, and move ever forward.Sincerely,Generosa Grana, MDDirector, MD Anderson Cancer Center at CooperHead, Division of Hematology/Medical OncologyProfessor of MedicineCooper Medical School at Rowan University1
Cancer Registry ReportThe Cancer Registry is a component of thecancer program at MD Anderson CancerCenter at Cooper that is responsible for theaccurate, timely collection of cancer patient datawhich is used for evaluation of patient outcomes.The Cancer Registry participates as an AmericanCollege of Surgeon’s (ACoS) Commission onCancer (CoC) accredited program and theNational Accreditation Program for Breast Centers(NAPBC). The CoC is responsible for establishingstandards to ensure high quality, multidisciplinaryand comprehensive cancer care delivery inhospitals throughout the United States, grantingaccreditation to only those facilities that havevoluntarily committed to provide the best incancer diagnosis and treatment and are able tocomply with the rigorous standards.The Registry reports specifics of diagnosis, stageof disease, medical history, patient demographics,laboratory data, tissue diagnosis, and medical,radiation, and surgical methods of treatment foreach cancer diagnosed at their facility. The data isused to observe cancer trends and provide aresearch base for studies into the possible causes ofcancer with the goal of reducing cancer incidenceand death.Registry data also serves as an ongoing resourceto the Cancer Committee in determining the mosteffective allocation of resources, in determiningcommunity education and outreach initiatives andin monitoring program quality.The Registry provides vital statistics andinformation to clinicians and researchers as wellas local, state and national cancer databases andcancer-related organizations. This contribution ofinformation advances the body of knowledge in thefield of cancer and ultimately has a positive impacton cancer patient care.For Cooper’s data to be comparable to thosecollected at other programs around the country, theregistrars adhere to data rules established by thecollecting and credentialing organizations.Cancer Registry Department StaffMargaret Carnuccio, CTR, ManagerBrian Palidar, RHIT, CTR, Cancer RegistrarJacqueline Ellis-Riffle, CTR, Cancer RegistrarKaren Staller, RHIT, Cancer RegistrarAnnette Harley, CTR, Cancer RegistrarCooper University Hospital Cancer Committee*REQUIREDPhysician MembersUmar M. Atabek, MDCancer Liaison-Surgeon,Surgery Dept.Raymond L. Baraldi, MDDiagnostic Radiology /Nuclear Medicine Dept.Generosa Grana, MDHem/Onc - Cancer Chair,Cancer Conf CoordinatorTamara A. LaCouture, MDRadiation Oncology Dept.Roland Schwarting, MDChief of PathologyREQUIREDNon-Physician MembersFrancis DelRossi, CSWSocial Worker & PsychosocialServices CoordinatorKristin L. Brill, MDNAPBC Representative/Breast SurgeonCori McMahan, PsyDDirector, Behavorial Medicine,Hem/Onc Dept.Dianne Hyman, MSN, RN, OCNQuality Improvement Coordinator/PI RepresentativeTondalya DeShields, RNClinical Educator,Oncology Outreach TeamDianne Moore, RN, MSNClinical Nurse Manager, 9N/9SEvelyn Robles-Rodriguez, APN-CCommunity Outreach CoordinatorAngela Frantz, RNBreast RN, NavigatorBarbara Sproge, MSNPalliative Care EducatorAnnette Harley, CTRCancer RegistryAmy Starling, MHSA, BBAAdministrator of Cancer ProgramLesley A. Hughes, MDRadiation Oncology DeptCarol Stratton, MSPT, ATC, CLTDirector, Rehabilitation ServicesSusan Hunter, AP-NAdvanced Practice Nurse,Hem/Onc Dept.Wendy Topeka, MSNClinical Director Outpatient InfusionMichael Kalfin, MPHDirector of Business OperationsOther AttendeesMargaret Carnuccio, CTRManager, Cancer RegistryColleen Thornton, ACS rep.American Cancer SocietyDana F. Clark, MS, MSGenetics CounselorJaime Austino, MSNGU & Head/Neck Nurse NavigatorJackie Ellis-Mullin, CTRCancer Registry QA CoordinatorLindsay Bagell DeLucaSocial WorkerBob LumpePastoral CareLisa McLaughlin, MSW, LSWSocial WorkerAlicia Michaux, RDOutpatient Nutritionist,Food & NutritionAlice O'Brien, RNLeuk/Lymph Nurse NavigatorBrian Palidar, CTRCancer RegistryArthur Schantz, MDPathology Dept.Karen Staller, RHITCancer RegistryAnn Steffney, MSN, RN, OCNClinical Director Patient ServicesPat Stienes, RTRadiology DirectorLeslie Tarr, MSWSocial WorkerColleen Tegeler, RNRadiation OncologyJackie Tubens, MSNGI Nurse NavigatorCharu Vora, MSNLung Nurse NavigatorKim Krieger, BA, CCRPHem-Onc Research Dept.*Committee members at time of publication.2
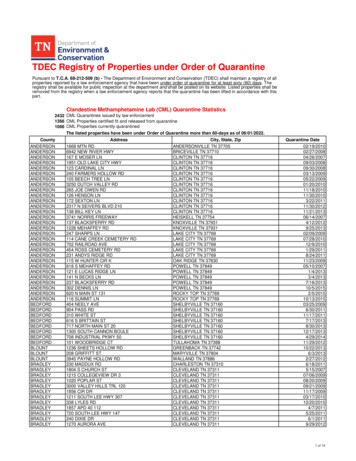
CANCER REGISTRY REPORTTop Five Cancer Sites TOTAL ANALYTICAL CASES 2001-2012450400350300Breast250Lung200Corpus UterusColon/Rectum150Prostate1005002001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 20122001 2002 2003 2004 2005Breast201219268313286Lung11010897122154Corpus 108861441282006 2007 2008 2009 2715411714212116817411882902011 201238542118820218216113012611479Patient’s County of Residence at Diagnosis 2012 ANALYTICAL %3{Cape May . . . . . .2.23%Cumberland . . . .3.83%Hudson . . . . . . .0.06%Hunterdon . . . . .0.11%Mercer . . . . . . . .1.72%Middlesex . . . . . .0.11%Monmouth . . . . .0.17%Ocean . . . . . . . .2.12%Salem . . . . . . . . .2.63%Out of State . . . .4.30%Unknown . . . . . .0.11%
CANCER REGISTRY REPORTMD Anderson Cancer Center at Cooper2012 ANALYTIC CASE DISTRIBUTION – BY SITE, SEX, AJCC STAGEPrimary SiteTotalCasesSexAJCC StageMaleFemaleStage 0Stage IStage IIStage IIIStage IV88UnkORAL CAVITY & PHARYNX28141401071901Tongue5230002300Salivary Glands2110000101Floor of Mouth1100000100Gum & Other VE tomach251780647404Small Intestine11740430301Colon Excluding Rectum84384642221131707Rectum & Rectosigmoid422418413710404Anus, Anal Canal & Anorectum9361042110Liver & Intrahepatic Bile Duct181620632403Gallbladder10551015300Other toneum1100010000Peritoneum, Omentum & Mesentery100100008200Other Digestive Organs3120000030RESPIRATORY SYSTEM20910410535464881017Nose, Nasal Cavity & Middle Ear1100001000Larynx6510102300Lung & Bronchus2029810435364578017BONES & JOINTS15960660102Bones & Joints15960660102SOFT TISSUE2211110648211Soft Tissue (including Heart)2211110648211SKIN Excluding Basal & Squamous351718013108310Melanoma – Skin301614010107300Other Non-Epithelial 42796174984012094
CANCER REGISTRY REPORTMD Anderson Cancer Center at Cooper2012 ANALYTIC CASE DISTRIBUTION – BY SITE, SEX, AJCC STAGE (continued)Primary SiteTotalCasesSexAJCC StageMaleFemaleStage 0Stage IStage IIStage IIIStage IV88UnkFEMALE GENITAL SYSTEM2640264115824551826Cervix Uteri37037015612400Corpus & Uterus, 0111011Vulva1501511021100Other Female Genital Organs1010100000MALE GENITAL 00400001URINARY SYSTEM8556291736155912Urinary Bladder36288157110210Kidney & Renal Pelvis47272022835702Ureter2110110000BRAIN & OTHER NERVOUS SYSTEM52203200000520Brain2011900000200Cranial Nerves Other Nervous System3292300000320ENDOCRINE SYSTEM792158048486103Thyroid69195004848603Other Endocrine including Thymus102800000100LYMPHOMA6027330191268015Hodgkin Lymphoma12660134103Non-Hodgkin 49500000140LEUKEMIA28141400000280Lymphocytic Leukemia127500000120Myeloid & Monocytic Leukemia157800000150Other ma3210101100KAPOSI SARCOMA1100000010Kaposi 4198Total5
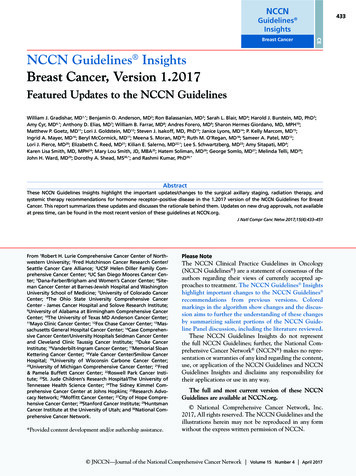
Measuring QualityHow do patients know if theyare receiving good qualityhealthcare?How do physicians andnurses identify the steps thatneed to be taken for betterpatient outcomes?And how do insurers andemployers determine whetherthey are paying for the bestcare that science, skill, andcompassion can provide?Performance measuresPerformance measures give the health care community a way to assessquality of care provided against recognized standards. While qualitymeasures come from many sources, those endorsed by the NationalQuality Forum (NQF) have become established as among the best.A NQF endorsement reflects rigorous scientific and evidence-basedreview, input from patients and their families, and the perspectives ofpeople throughout the health care industry.One of the ways Cooper University Health Care assesses the quality ofthe care we give to our cancer patients is to compare our performancein NQF standards to those of other hospitals in New Jersey and theUnited States.NQF has established six measures for quality care in breast, colon andrectal cancer. Below you will find how Cooper compares to otherhospitals in New Jersey and across the U.S. in these criticalperformance measures.Cooper performed significantly above both the statewide and theU.S. norms.Performance for NQF Breast Care ERNJNational Standard for Breast Conserving Surgeryand Radiation TherapyRadiation therapy is administered within one year (365 days) ofdiagnosis for women under the age of 70 receiving breast conservingsurgery for breast cancer. Cooper’s compliance with this standardwas at 91%, compared to the state norm of 88.8% and the nationalnorm of 90.7%.National Standard for Chemotherapy in hormonereceptor negative breast cancer patientsCombination chemotherapy is considered or administered within4 months (120 days) of diagnosis for women under the age of 70with AJCC T1cN0M0, or stage II or III hormone receptor negativebreast cancer. Cooper’s compliance with this standard was at 95.8%,compared to the state average of 84.3% and national norm of 91.4%.US6
91.9%87.6%83%COOPERNJNational Standard for Tamoxifen or third generation aromataseinhibitor in hormone receptor positive breast cancer patientsTamoxifen or third generation aromatase inhibitor is considered oradministered within one year (365 days) of diagnosis for women withAJCC T1cN0M0, or stage I hormone receptor positive breast cancer.Cooper’s compliance with this standard was at 91.9%, compared tothe state norm of 83% and the national norm of 87.6%.USPerformance for Colon and Rectal Cancer NQF .3%NJUS92.9%92.6%NJUS100%COOPERNational Standard for Regional Lymph Nodesin Surgically Resected PatientsAt least 12 regional lymph nodes are removed and pathologicallyexamined for resected colon cancer. The compliance rate for Cooperwas at 87.2%, compared to the state norm or 88.6% and the nationalnorm of 87.8%.National Standard for Adjuvant Chemotherapyfor Node Positive PatientsAdjuvant chemotherapy is considered or administered within fourmonths (120 days) of diagnosis for patients under the age of 80 withAJCC stage III (lymph node positive) colon cancer. The compliancerate for Cooper was at 100% compared to the state norm of 85.7%and the national norm of 88.3%.National Standard for Radiation Therapyof Stage III Rectal CancerRadiation therapy is considered or administered within six months(180 days) of diagnosis for patients under the age of 80 with clinicalor pathologic AJCC T4N0Mo or stage III receiving surgical resectionfor rectal cancer. The compliance rate for Cooper was at 100%,compared to the state norm of 92.9% and the national norm 92.6%.7
Lung Cancer ReportANNUAL REPORT 2011EpidemiologyLung cancer remains the leading cause of cancer related mortality both in the United States and worldwide and in both men andwomen. It is estimated that 228,190 new cases of lung cancer (118,080in men and 110,110 in women) were diagnosed in 2013 and 159,480will die of lung cancer. More men than women will die from lungcancer; 87,260 and 72,220 respectively. In the state of New Jerseythere are 5,960 estimated new cases of lung cancer and 4,060 deathsestimated in 2013.Risk FactorsPriya C. Singh, MDHematologist/Medical OncologistLung Cancer ProgramMD Anderson Cancer Center at CooperAssistant Professor of MedicineCooper Medical School of Rowan UniversityThe primary risk factor for lung cancer is tobacco smoke, and therisk of lung cancer increases with the number of packs of cigarettessmoked per day and the number of years spent smoking. Exposureto second hand tobacco smoke, radon gas and asbestos also increases the relative risk of developing lung cancer. In rare cases,chronic lung inflammation, lung scarring from tuberculosis, and exposure to carcinogenic chemicals such as arsenic, bis (chloromethyl)ether, polycyclic aromatic hydrocarbons, chromium, nickel, cadmium, beryllium, and silica can cause lung cancer.SurvivalThe overall five-year survival for all stages of lung cancer is 15%.This number has remained constant over the past three decades.Surgery is the only curative modality for lung cancer, although asmall percentage of patients with late stage disease will survivemore than 5 years with treatment. Five-year survival for pathologicstage I A/B patients is 75/71%, stage II A/B is 58/49%, stage IIIA23%, and stage IIIB/IV 5%.2012 Analytic NSCLC by CountyCamdenBurlingtonGloucesterAll Other8
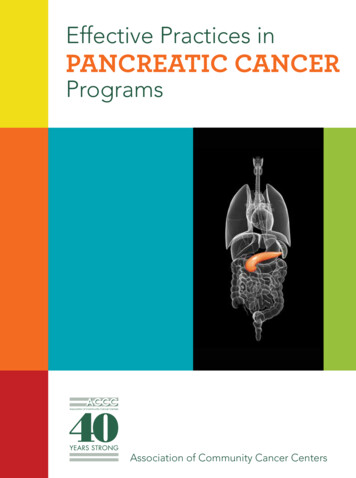
Age at Diagnosisfor NSCLC at Cooper University Health Care vs NCDB, National Cancer Data Base (2011 most current year available)35%30%Percentage25%20%15%CUH 201210%CUH 2001–20115%NCDB 2011NCDB ��7980–8990 Age at DiagnosisAJCC Stage at Diagnosisfor NCSLC at Cooper University Health Care vs NCDB, National Cancer Database (2011 most current year available)50%40%Percentage30%20%CUH 201210%CUH 2001–2011NCDB 2011NCDB 2001–20110%0IIIIIIIVUnkStageScreeningCooper Tumor RegistryLate diagnosis has been a major obstacle in improving lung cancer outcomes; however, in 2010, theNational Lung Screening Trial (NLST) showed survival benefit for low dose CAT scans as a screeningstudy for lung cancer. This large randomized controlled trial showed a 20% decrease in lung cancermortality in high risk individuals screened with lowdose CAT scans compared to those screened withchest x-rays. High risk individuals in the trial wereaged 55-74 years with a 30-pack year of current orformer tobacco use. To prevent one death from lungcancer, 320 high risk individuals must be screened.In 2012, 182 patients received all or a portion oftheir treatment for lung cancer at Cooper. A little over50% of those were from Camden County and the majority of the other patients were from Burlington andGloucester counties. These figures have remained relatively unchanged over the past decade.At Cooper, the average age at diagnosis of lungcancer was slightly younger in the 6th decade of life,compared to the national average age at diagnosis inthe 7th decade. The age at diagnosis in different agegroups was consistent with that nationally reportedby the National Cancer Data Base (NCDB).9
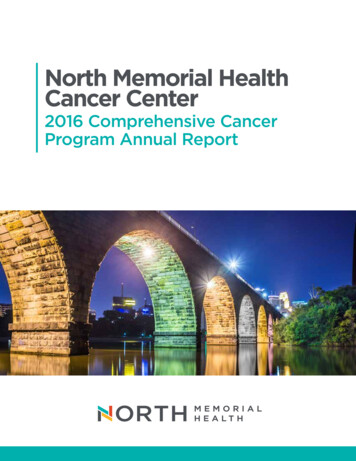
11.3% were black and 3% were Hispanic. AtCooper in 2012, 71% were white, 22% were blackand less than 5% were classified as Hispanic. Thisis not surprising since a significant portion of theCooper patient base is drawn from the city ofCamden, which has a largely black and Hispanicpopulation.The staging at diagnosis at Cooper was similarto national data with most lung cancer patients presenting at stage III and IV from 2000-2011, howeverin 2012 more patients were diagnosed at stage I.There may be a shift in stage at diagnosis with agreater number of patients diagnosed in stage I sincelow dose CAT scan screening is being increasinglyused. The NCDB has not published data for 2012 toassess if this change in staging is occurring nationwide.Cooper patients by Ethnicity - erPatient demographics were fairly similar except for the higher percentage of blacks treated atCooper. Nationwide in 2011, 82% of those diagnosed with non small cell lung cancer were white,Cooper 2001-2011 NSCLC TreatmentCooper 2012 NSCLS TreatmentTotal CasesTotal iativeChemoChemoRadiationRadiationSurgery OnlySurgery OnlyDiagnostic OnlyDiagnostic OnlyRadiation/ChemoRadiation/Chemo0501000150 200 250 300510152025Number of CasesNumber of CasesNationwide Data — NCDB1st Course of Treatment — ChemoRadiationSurgery OnlyRadiation/Chemo0Other 637154,20156,77540,60846,4001030 3540
Treatmentfew cases at Cooper to be analyzed; stage III 12.6%(versus 11.2% NCDB) and stage IV 5.1% (versus2.7% NCDB).Also of note is the difference in patients receiving surgery as their initial therapy for lung cancer:5% fewer patients at Cooper had surgery. Multiplepublications have documented that blacks (especially black males) are significantly less likely tohave surgery for lung cancer than other racial/ethnic groups, however in spite of this, survival wasslightly better at Cooper than national averages.Surgery has increased as the sole treatment modality from 14% to 18% and this may be the case withincreasing use of CT screening.Surgical resection was performed in 259 of the1423 Cooper lung cancer patients from 20012011(17%) and surgery was the only form of therapy in 14%. 41% received radiotherapy as part oftheir treatment and 34% received chemotherapy. Fifteen percent of Cooper patients received no therapyfor their lung cancer from 2001-2011.In 2012, surgical resection was performed in 37 ofthe 182 Cooper lung cancer patients (20%) and surgerywas the only form of therapy in 18%. 40% received radiotherapy as part of their treatment and 47% receivedchemotherapy. Fourteen percent of Cooper patientsreceived no therapy for their lung cancer in 2012.Nationwide data 2001-2011 showed that surgicalresection was performed in 25% of patients and surgerywas the only form of therapy in 20%. 38% receivedradiotherapy as part of their treatment and 42% received chemotherapy.Survival statistics from the NCDB for non-smallcell lung cancer patients are presented in Figure 7,while survival for all Cooper patients seen in 20032006 is shown in Figure 8. When Cooper survivaldata was compared to NCDB data from 2003-2006,5-year survival was slightly higher for all stages oflung cancer treated at Cooper as follows: stage I53.3% (versus 46.8% NCDB); stage II there were tooComprehensive Lung Cancer CareMD Anderson at Cooper is South Jersey’s leading provider in the detection, diagnosis and treatment of lung cancer. MD Anderson at Cooper’sLung Cancer Center combines state-of-the-art, compassionate medical care with innovative science toprovide the best possible outcomes for patients.MD Anderson at Cooper’s reputation for excellence can be attributed to our multidisciplinary approach to lung cancer care. Each of our patients isunder the care of an entire team of experts, consisting of:Figure 7: Five-Year Survival Rate 2003—2006 Analytic NCSLC Cases: NATIONAL CANCER DATABASE100Occult90Stage 0Stage I80Cumulative Survival RateStage IIStage III70Stage IV60504030201000.01.02.03.0Years From Diagnosis114.05.0
Figure 8: Five-Year Survival Rate 2003—2006 Analytic NCSLC Cases: COOPER UNIVERSITY HOSPITALObserved Survival for Lung, Bronchus — Non-Small Cell Carcinoma“C340,” “C341,” “C342,” “C343,” “C348,” “C349”100Stage I90Stage IIIStage IVCumulative Survival Rate807060504030201000.01.02.03.04.05.0Years From DiagnosisCases Diagnosed in 2003—2006Data from 1 ProgramsWARNING: The information within this graphic is not to be used for clinical decision making. Thoracic surgeons Medical oncologists Radiation oncologists Pulmonary medicine specialists Interventional pulmonologists Pathologists Radiologists Nurse navigator Nurse practitioner Clinical research coordinators Social workers Palliative care teamabnormalities.When appropriate, MD Anderson at Cooperthoracic surgeons offer minimally-invasive surgicalprocedures, including robotic-assisted lobectomy aswell as thorascopic lobectomy (Video-Assisted Thoracic Surgery or VATS). MD Anderson at Cooperlung surgeons have performed more lung cancer surgeries using the da Vinci robot than any other hospital in South Jersey.MD Anderson at Cooper offers a full spectrum ofradiation oncology treatment options including external beam radiation therapy and CyberKnife radiosurgery. The CyberKnife system is designed topinpoint and destroy tumors using high doses ofradiation with sub-millimeter accuracy.Our medical oncologists offer patients the mostadvanced chemotherapy treatments and access togroundbreaking clinical trials that give patientsoptions that may not be available elsewhere in theregion. In 2012, four patients who met eligibility criteria were enrolled in clinical trials.The center is seeing a shift in more stage I lung cancers diagnosed and this may be from the implementation of low dose CT screening for lung cancer. MDAnderson at Cooper has a high risk lung cancerscreening program and has screened approximately20 patients since its inception.Our multidisciplinary lung cancer team meetsonce weekly to review cases to provide each patientwith a comprehensive evaluation and an individualized treatment plan.More recently MD Anderson at Cooper has committed to the improvement in lung cancer care inSouth Jersey through developing an interventionaldiagnostic program with fellowship trained interventional pulmonologists. MD Anderson at Cooperis the only South Jersey hospital performing endobronchial ultrasound (EBUS)-guided bronchoscopy.This minimally invasive procedure enables physicians to safely, accurately, and quickly biopsy previously difficult-to-access lymph nodes and chest12
MD Anderson Cancer Center at CooperTwo Cooper Plaza, 400 Haddon AvenueCamden, NJ 081031.855.MDA.COOPER (1.855.632.2667) MDAndersonCooper.org
Susan Hunter, AP-N Advanced Practice Nurse, Hem/Onc Dept. Michael Kalfin, MPH Director of Business Operations Bob Lumpe P asto rlC e Lisa McLaughlin, MSW, LSW ocialW rke Alicia Michaux, RD O u tpa ie nN r o s, od&Nu trin Cori Mc ahn,PsyD D ir ect o ,Bh av lMd n Hem/Onc Dept. Dianne Moore, RN, MSN Clinical Nurse Manager, 9N/9S Alice O'Brien, RN