Transcription
Carle Cancer Center PublicReporting of Outcomes2017 ANNUAL REPORT
Table of ContentsCarle Foundation Hospital 3Chairman’s Message 4Carle Research and Cancer Conferences52017 Cancer Committee Members and their Alternates6Clinical Trial Accruals: 7Lung Cancer in Our Community — A Report by Dr. Suparna Mantha8Non-Small Cell Lung Cancer Benchmarks8Outreach Activities 10Cancer Registry 11Quality Studies: 12Quality Improvements: 12Who We Serve 13Summary of Body Systems 142 Carle Cancer Center Public Reporting of Outcomes
Carle Foundation HospitalOur MissionOur VisionOur ValuesWe serve people through high qualitycare, medical research and education.Improve the health of the peoplewe serve by providing world-class,accessible care through and integrateddelivery system.ICARE—Integrity, Collaboration,Accountability, Respect, Excellence.NOTABLE HEALTHGRADES AWARDS IN 2017: America’s 50 Best Hospitals Award (2 yrs. in a row) America’s 100 Best Hospitals for Critical Care (6 yrs. in a row) Top 1% in the nation for consistent clinical quality Distinguished Hospital Award for Clinical Excellence Most Wired health system by Hospitals & Health Networks(6 yrs. in a row for Carle; 5 yrs. in a row for Hoopeston Regional Health Center) Top 34 Hospitals for Hip Replacement by Consumer Reports (reported by Becker’s Orthopedic Review) 100 Great Healthcare Leaders to Know, CEO/President Dr. Leonard by Becker’s Hospital Review3 Carle Cancer Center Public Reporting of Outcomes
Chairman’s MessageNovember 15, 2017Carle Cancer Center continues its mission of providing high quality cancer care through education,continuous quality improvement, research and technology.Our cancer program is accredited by the Commission on Cancer /American College of Surgeonson Cancer as an Academic Comprehensive Cancer Program. The Mills Breast Cancer Institute isalso accredited by the National Accreditation Program for Breast Centers (NAPBC). Both of thesere-accreditation surveys were completed this year; both are good for a three (3) year period, with our next survey to bescheduled in 2020. In addition to CoC and NAPBC accreditations, we also have various specialty accreditations includingthe American College of Radiology (ACR) for our Radiation Oncology services and the American Society of ClinicalOncology’s Quality Oncology Practice Initiative (QOPI) for Medical Oncology services.Our newest relationship is with the University of Illinois Carle College of Medicine. This formalizes and strengthens ourcommitment to education and research.Cancer Research is an integral part of our cancer care system. We have been involved in national clinical research since1976. Carle Cancer Center was first recognized as a Comprehensive Community Oncology Center by The NationalCancer Institute (NCI) in 1983. In 2014, Carle Cancer center was designated as a National Community Oncology ResearchProgram. As one of only 34 such NCORP sites in the nation, Carle Cancer Center participates in cancer treatment,prevention, and control studies, as well as academic-based and investigator-initiated studies.Any Carle physician may ask for data (with IRB approval) or sponsor research using our database. Interested individuals,including medical and nursing students, resident physicians, nurses, U of I facility may obtain sponsorship.The Cancer Registry is the information backbone of our cancer clinical research efforts. It provides feasibility data toallow U of I basic science. Starting in 1934, the data collected by our Cancer Registry department was originally kept todetermine patterns of disease with outcomes and to adjust strategies to detect cancer. It is now used not only to identifypatterns and outcomes, but to support research activities at Carle and across the nation. Data is also used to assess theneed for space, used for patient care, capital equipment and the need for services with a geographic area. National cooperative studies with the American Cancer Society and the American College of Surgeons have used our data as well.Carle is a small part of the total picture, which is reflected by the State of Illinois Department of Public Health CancerRegistry website.The Carle Cancer Center engages multidisciplinary cancer clinics, patient navigators, support groups, and clinical trialopportunities to deliver integrated cancer care.Our accreditations through Commission on Cancer (CoC), National Accreditation Program for Breast Centers (NAPBC),Quality Oncology Practice Initiative (QOPI) and American College of Radiology (ACR) continue to validate ourcommitment to the highest quality of care.Sincerely,James R. Egner, MDChairman, Carle Cancer Committee4 Carle Cancer Center Public Reporting of Outcomes
Carle Research and Cancer ConferencesAll conferences serve as a multidisplinary consulting board for presenting cancer cases andmaking recommendations for the patient’s course of diagnosis, treatment and survivorship.up for the future and the clinical trials that have opened,closed and would be best for Carle. On occasion, outsidespeakers present studies and interesting research topics.The conferences are attended by physicians from allcancer specialties, staff, interns, medical students,residents, nurses, social workers, dietians, geneticcounselors, researchers, cancer registry staff andapproved guests. All the conferences are held withthe utmost of confidentiality and the underlying goalis to ensure high quality of seamless care provided toall patients and their families.Carle Foundation is accredited by the Illinois StateMedical Society to provide continuing medical educationfor physicians and staff. The Care Foundation designateseach educational activity for a maximum of 1 AMA PRACategory of 1 Credit.The Houseworth Conference Room is designed with hightech equipment and capabilities of skyping out to theoutside facilities, physicians and staff who cannot attendthe conference in person. The Carle satellite in Danville,IL. are invited to join in on the conferences. Outsidephysicians can participate, observe and present cases, inwhich the multidisplinary team at Carle can provide theiropinions on the outside casesTHE FOLLOWING IS A LIST OF OUR CONFERENCES:Research conferenceFrequency: Every week on Fridays in the HouseworthConference RoomChair: Dr. Kendrith RowlandUniversity of Illinois teaching researchers and Carleclinical researchers inform the physicians and staff ofthe different protocols and clinical trials.In the research conferences, the researchers andphysicians present and discuss new clinical trials coming5 Carle Cancer Center Public Reporting of OutcomesGeneral cancer conferenceFrequency: Every week on Friday in the HouseworthConference RoomChair: Dr. James EgnerGI cancer conferenceFrequency: Every week on Fridays in Digestive Health.Chair: Dr. Robert DodsonThis conference used to be held in conjunction withGeneral Cancer Conference. With the opening of theGI Multidisciplinary Clinic in July, this conference is nowheld weekly before the start of the clinic day. This willensure that those enduring GI cancer will have accessto a multidisplinary approach with less barriers.Breast cancer conferenceFrequency: Every Wednesday in the HouseworthConference RoomChair: Dr. Maria Grosse- PerdekampHead and neck conferenceFrequency: First and third Monday of every monthin the Houseworth Conference RoomChair: Dr. Kelly CunninghamGenitourinary (GU) and Gynecology (GYN)cancer conferenceFrequency: Second and fourth Tuesdays of every monthin the Houseworth Conference Room.Chair: GU- Dr. Glen Yang GYN- Dr. Ronald KimballThe GYN Cancer Conference has applied to becomea CME Credited Conference.Thoracic surgery/pulmonary case conferenceFrequency: second and fourth Thursday of every monthin the Houseworth Conference RoomChair: Dr. Yujie Zhao
2017 Cancer Committee Members and their AlternatesAcademic Comprehensive Cancer Program (Approved 2/6/2017)Cancer Program Standard 1.32017 Cancer Committee MembersRoleMemberAlternateCancer Committee ChairCancer Liaison PhysicianDiagnostic RadiologistPathologistSurgeonMedical OncologistRadiation OncologistGI Center for ExcellenceSpecialistPalliative CareDr. James Egner/Dr. Suparna ManthaDr. Anna Higham/ Dr. Pratima ChalasaniDr. Martin KuntzDr. Frank BellafioreDr. Anna HighamDr. James Egner/Dr. Suparna ManthaDr. Kalika SarmaDr. Robert DodsonDr. Kendrith RowlandDr. Michael ArefDr. Maria Grosse-PerdekampDr. Vamsi VasireddyDr. James HlubockyDr. Ike UzoaruDr. Marta SpainDr. Maria Grosse-PerdekampDr. Sinisa StanicDr. Michelle OlsonRoleCancer Program Adm.Registered DieticianOncology NurseSocial WorkerCert. Tumor RegistrarCancer Conference CoordinatorQuality Improvement CoordinatorCa. Registry Quality CoordinatorComm. Outreach CoordinatorClinical Research CoordinatorPharmacistRehabilitationRadiation OncologyPastoral CareGenetics CounselorAmerican Cancer SocietyMemberCaleb Miller/ Matthew KolbTammie HeiserCourtney Cox, RNKimberly Harden, LCSWSharon Jacobson, CTRSharon Jacobson, CTRSarah Glenn, RNSharon Jacobson, CTRMary VanCleave, RNBetsy Barnick, BSTodd Thompson, RPHRenee DanielsDavid Pool, BSJeffrey McPikeJacquelyn Johnson, MSLinda SchulzAlternatePamela Bigler, RN/ Jason HirschiDr. Anna ArthurChristine Plotner, RNKelly Harris, LCSWHeather Benson, CTRHeather Benson, CTRSherry Rose, RNHeather Benson, CTRGloria Davis, RNJoshua Ward, BSLauren Trisler, PharmDElizabeth CampAmy Gerdes, RTTThe Cancer Committee selected the following membersto represent each of the following cancer committeecoordinator specialties: KimberlyHarden, MSW, LCSW – Psychosocial ServicesQuality Coordinator Betsy Barnick, BS, CCRP – Clinical Research Coordinator Mary VanCleave, BSN, RN, OCN – CommunityOutreach Coordinator Sarah Glenn, MSN, RN, OCN – Quality ImprovementCoordinator Sharon Jacobson, CTR – Cancer RegistryQuality Coordinator Sharon Jacobson, CTR – CancerConference Coordinator6 Carle Cancer Center Public Reporting of OutcomesDr. April YasunagaCarle’s cancer committee has four required quarterlybusiness meetings. They consist by discussing theCommission on Cancer Program Standards, EligibilityRequirements, registry activities, and new business. Theadministrative cancer committee determines the goals,quality studies, improvements, community outreachactivities, screening and prevention programs and whatwill benefit our patients and community.The Administrative Cancer Committee Meetings wereheld on second floor in the Houseworth Conference Roomon February 6th, May 8th, August 7th and November 6thin 2017.
Clinical Trial AccrualsFor nearly 35 years, the Carle Cancer Center has offeredpatients access to cutting edge clinical research. As oneof the first cancer facilities in the United States to bedesignated a Community Clinical Oncology Program(CCOP), now renamed National Community OncologyResearch Program (NCORP), Carle is one of only 34 healthcare groups in the nation to have this designation by theNational Cancer Institute (NCI). These research initiativesoffer new insight into how to prevent cancer, demonstratenew ways to treat cancer and its side effects, and explorenovel screening and imaging modalities. In addition, thesetrials focus on supportive care, symptom management,surveillance, quality of life and genetics.7 Carle Cancer Center Public Reporting of OutcomesMore recent to the cancer research program are increasedcollaborations with the University of Illinois. Throughinitiatives like C*STAR, also known as the Cancer Scholarsfor Translational and Applied Research, several trials areunderway examining topics like individualized treatmentregimens, cognitive health, nutrition and survivorship, andtumor imaging. This jointly funded graduate program,initiated in the fall of 2015, matches students with an Illinoisfaculty mentor and a Carle physician mentor. The programfosters translational research and was developed toencourage near-term benefits to patients served by Carleand the greater Champaign-Urbana community. C*STARprojects complement other U of I projects that are ongoingin the areas of activity and cognition, imagingand nutrition.
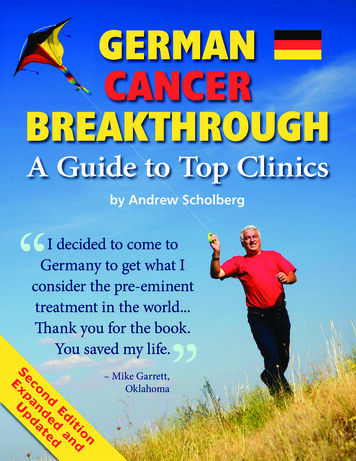
Lung Cancer in Our CommunityA Report by Dr. Suparna ManthaThe Cancer Committee identified lung cancer as an areaof focus for 2017. The incidence of lung cancer is higherin Vermilion and Coles counties, both are major serviceareas for the cancer center.Lung cancer is the second most common cancer inboth men and women. It is the leading cause of deathfrom cancer. According to the NCI SEER database, theestimated new cases of lung cancer in 2017 is 222,500accounting for 13.2% of new cancer cases. Estimateddeaths from lung cancer in 2017 is 155,870, which is 25.9%of all cancer deaths.The most common risk factors for lung cancer includesmoking, exposure to second hand smoke, radiationexposure – from radiation therapy, imaging tests, Radonexposure, exposure to air pollution etc. The median age atdiagnosis is 70 years.There are two main types of lung cancer – Non-small celllung cancer and small cell lung cancer. Non-small cell lungcancer is more common of the two types.A review of NCDB report for Carle Foundation HospitalCancer Center was performed for the years 2011 to2015 and compared to data from other ComprehensiveCommunity Cancer Programs. Consistent with the SEERdata, the most common age group at diagnosis for Nonsmall cell lung cancer was 70-79 years. As lung cancer isusually diagnosed at advanced stage, the most commonCarle has offered low dose CT screening for lung cancersince 2013, to people who are at high risk to develop lungcancer. This year, Carle conducted four education eventsin the month of October, focusing on education regardingRadon exposure and risk of cancer, symptoms and signs oflung cancer and information regarding Radondetection kits.The most common mode of treatment for early stageNon-small cell lung cancer is surgery. The more advancedstages are treated with a combination of surgery,chemotherapy and/or radiation. The rate of surgery andradiation therapy to treat lung cancer at Carle are similarto other comprehensive community cancer programs.To ensure timely, expedited care and access to variousspecialists involved in care of lung cancer patients, Carleis now planning Lung multidisciplinary clinic. Such aclinic will add to our goal to attack lung cancer right fromprevention, education, screening andmultidisciplinary care.200150120CASES (N)NON-SMALL CELLLUNG CANCERBENCHMARKSThe number ofcases of non - smallcell lung cancerdiagnosed at Carlefrom 2011 to 2015 isa follows:stage at diagnosis was Stage IV. With improved screening,the second most common stage was Stage I. Thedistribution of new cancers diagnosed across differentstages was similar to the data from other comprehensivecommunity cancer center IS YEAR8 Carle Cancer Center Public Reporting of Outcomes20142015
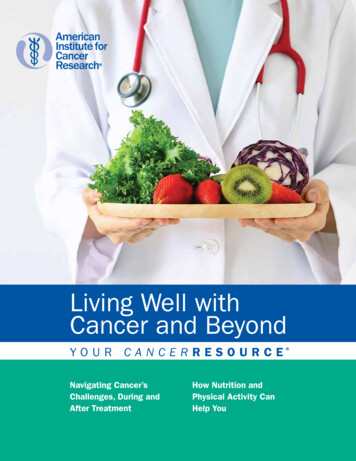
38%38%THE DISTRIBUTIONOF NEW NON SMALL CELL LUNGCANCER BY STAGE:PERCENTAGE (%)29%27%19%17%11%10%0%7%0%0IIIIIIIVUNKSTAGETHE FIRST COURSE OF TREATMENT FOR NON-SMALL CELL LUNG CANCER AT CARLE COMPARED TO OTHERCOMPREHENSIVE COMMUNITY CANCER PROGRAMS:PERCENT (%)23%23%19%17%21% 21%17%20%14%12%12%14%16%5%6%0%SurgeryOnlyRadiation &No 1stChemotherapy RadiationOnlyChemotherapy Course RXOnly5%Surgery &ChemotherapyFIRST COURSE TREATMENTMy FacilityOtherMetricCarle Performance RateRequired Performance RateSystemic chemotherapy is administered within 4 m onths to daypreoperatively or day of surgery to 6 months postoperatively, or it isrecommended for surgically resected cases with pathologic lymph nodepositive (pN1) and (pN2) NSCLC (Quality Improvement)100%85%Surgery is not the first course of treatment for cN2, MO lung cases (QualityImprovement)100%85%At least 10 regional lymph nodes are removed and pathologically examinedfor AJCC stage IA, IB, IIA and IIB resected NSCLC (Surveillance)41.7%N/A(NCDB CP3R Measures 2015)9 Carle Cancer Center Public Reporting of Outcomes
Outreach ActivitiesRadon and Lung Cancer: An Education event aimed at the prevention of Radon relatedLung Cancer.Carle Cancer Center held four (4) education andprevention sessions at different locations in our servicearea on the following dates: 10/1/2017 10/7/2017 10/20/2017 10/29/2017Radon education materials were given out along with astock card with lung cancer signs and symptoms. This wasin accordance with the Community Needs Assessmentand the Illinois Emergency Management Agency (IEMA).Information is in accordance with the NCCN guidelineLCS-1, and is obtained from the Environmental ProtectionAgency (EPA). Also given was information regardingseveral different types of Radon detection kits availableand the cost associated with each kit, obtained fromthe IEMA.10 Carle Cancer Center Public Reporting of OutcomesA small survey was given to each participant to determineif the participant felt the information was helpful and if theywould utilize the information given.A total of 69 people accepted the information: 59 participants (85%) felt the information was of use tothem and would follow up with Radon detection. 10 people felt it was not helpful:–– 4 were already scheduled for service to remit the gasin their homes.–– 2 were undergoing testing–– 2 were in the business of Radon mitigation–– 2 would not respond
Cancer RegistryMission: Carle Cancer Registry is dedicated to accurately abstracting cancer information frommedical records and maintaining a Certified Cancer Registry. Patients diagnosed and/or treatedwith cancer are followed annually with the utmost compliance of confidentiality for their lifetime.Cancer Registry abstracts, collects and maintains all cancer patient information at Carle. The Cancer Registry staff followsthe cancer patient for their life- time if they are diagnosed and/or treated at Carle. The abstracted information providesthe registry with measurement of outcomes and cancer patient survival. Our annual analytic caseload is over 1500 cases.Table 1: Follow up Rates as required by Commission on Cancer/American College of Surgeons:RequirementActual RateReference Year (2000)80%87.86%5 year90%94.47%2017 CANCER REGISTRY STAFFSharon Jacobson, CTR, Cancer Program CoordinatorSarah Glenn, MSN, RN, OCN, Quality CoordinatorJulie McClain, Cancer Registry InternStephanie Grote, Cancer Registry Specialist11 Carle Cancer Center Public Reporting of OutcomesOUTSOURCED REGISTRY STAFFDawn Grabowski, CTRHeather Benson, CTRBrandy Lewis, CTRTalisha Ballard, CTRTiffany Ervin, CTR
Quality StudiesThe Commission on Cancer “is dedicated to improvingsurvival and quality of life for cancer patients throughstandard-setting, prevention, research, education and themonitoring of comprehensive quality of care.”of women with endometrial cancer treated surgically whoundergo minimally invasive surgery with laparoscopic DaVinci robot (total hysterectomy and bilateral salpingooophorectomy with or without pelvic sentinel lymphnode mapping). The target goal is 65%. The study datacontinues to be evaluated but we are meeting our targetgoal. Timely changes will be considered based on datareceived. Over a six month time frame, we had 23 patientswho had surgery for their endometrial cancer. Of those 23patients, 19 had surgery with robotic assistance. Those thatdidn’t, had conditions that did not lend themselves for alaparoscopic surgery.The Carle Cancer Center 2017 study of quality is lookingat the quality of care for endometrial cancer. At thepresent time measures are being monitored and evaluatedendometrial surgery. The study was chosen by the cancerteam to ensure that those patients having surgery forendometrial cancer are getting the least invasive surgeryaccording to the guidelines of the Society of GynecologicOncology. Specifically we are assessing the percentage% Robotically assisted surgery for endometrical cancer2 3 %CASES (N)100%50%0%JanFebMarAprMayJun% Robotically assisted surgery for endometrical cancerQUALITY IMPROVEMENTS100%The Carle Cancer Center Cancer Committee decided on a quality improvement to ensure that 100% of all eligiblewomen diagnosed with epithelial ovarian cancer are being offered genetic testing.Any cause for a patient not offered80%100%genetic testing will be investigated, documented and tracked. The practice statement by the Society of Gynecologic60% cancers should receive geneticOncology states that women diagnosed with epithelialovarian, tubal, and peritoneal80%counseling and be offered genetic testing, even in the absence of a family history. Nine months of data show that 100%40%of eligible patients are being offered an appointmentwith our genetics counselor.Evaluation and feedback from the60%Cancer Committee has been performed on a quarterly basis and will continue to complete the ffered genetics40%20%0%JanFebMarAprMayOffered genetics12 Carle Cancer Center Public Reporting of OutcomesJunJulTargetAugSepMarAprMayOffered geneticsJunJulAugTargetJuSep
Who We Serve* Metriq (Elekta) through Carle80-8912%90 2%0-292% 30-393%40-498%70-7924%50-5920%60-6929%* Metriq (Elekta) through Carle13 Carle Cancer Center Public Reporting of Outcomes
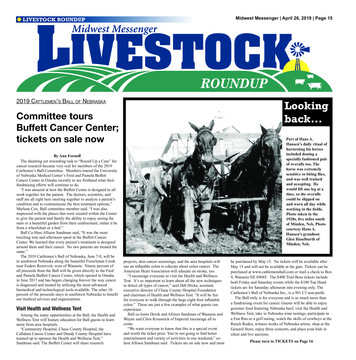
* Metriq (Elekta) through CarleSummary of Body System and Sex Report, 11/14/17MalesOral Cavity & Pharnyx - 40 (6%)Lung & Bronchis - 97 (15%)Pancreas - 30 (5%)Kidney & Renal Pelvis - 36 (6%)Urinary Bladder - 38 (6%)Colon % Rectum - 65 (10%)Prostate - 129 (20%)Non-Hodgkin Lymphoma - 29 (4%)Melanoma of the Skim - 55 (8%)Leukemia - 19 (3%)All other sites - 119 (18%)FemalesThyroid - 46 (6%)Lung & Bronchis - 75 (10%)Breast - 226 (30%)Kidney & Renal Pelvis - 13 (2%)Ovary - 23 (3%)Uterine Corpus - 69 (9%)Colon % Rectum - 62 (8%)Non-Hodgkin Lymphoma - 22 (3%)Melanoma of the Skim - 49 (7%)Leukemia - 10 (1%)All other sites - 154 (21%)Images reprinted by the permission of the American Cancer Society, Inc. from www.cancer.org. All rights reserved* Metriq (Elekta) through Carle14 Carle Cancer Center Public Reporting of Outcomes
HCRG111717A
NON-SMALL CELL LUNG CANCER BENCHMARKS The number of cases of non - small cell lung cancer diagnosed at Carle from 2011 to 2015 is a follows: The Cancer Committee identified lung cancer as an area of focus for 2017. The incidence of lung cancer is higher in Vermilion and Coles counties, both are major service areas for the cancer center.