Transcription
NYC Hospital Guidance for Respondingto a Contaminating Radiation IncidentApril 2009Created byNYC Hospital Radiation Response Working GroupNYC Department of Health and Mental HygieneHealthcare Emergency Preparedness Program
This publication was supported by Grant Number U3RHS05957-01-00 from theHealth Resources and Services Administration. Its contents are solely theresponsibility of the authors and do not necessarily represent the official views ofHRSA.All inquiries about the “Hospital Guidance for Responding to a ContaminatingRadiation Incident”may be addressed to:Healthcare Emergency Preparedness Programc/o NYC Department of Health and Mental Hygiene125 Worth Street, RM 222, Box 22ANew York, NY 10013Phone: 212-788-4277or by e-mail athepp@health.nyc.gov
List of ContributorsNYC Hospital Radiation Response Working GroupChairpersonCurt Dill, MDDirectorEmergency MedicineVA New York Harbor Hospital SystemProject Manager/EditorKatherine Uraneck, MDSenior Medical CoordinatorHealthcare Emergency Preparedness ProgramNYC Department of Health & Mental HygieneManfred Blum, MDProfessor of Medicine & RadiologyNYU School of MedicineLewis R. Goldfrank, MDProfessor and Chair, Emergency MedicineNew York University School of MedicineDirector, Emergency MedicineBellevue Hospital/NYU Hospitals/VAMedical CenterMedical DirectorNew York City Poison CenterBruce Ellerin, MDRadiation OncologyNYU School of MedicineChristopher Marshall, Ph.DProfessor Emeritus of RadiologyNYU School of MedicineKent Friedman, MDAssistant Professor of RadiologyDivision of Nuclear MediciNYU School of MedicineRajesh Mittal, MDEmergency MedicineSUNY Downstate/Kings County HospitalCenterChristopher Freyberg, MDDirector, Emergency DepartmentSouthern Arizona VA Health Care SystemGabriella Wernicke, MDAssociate Professor Radiation OncologyRadiation OncologyNYU Clinical Cancer CenterJoseph Albanese, Ph.DRadiation BiodosimetristYale New Haven Center for EmergencyPreparedness and Disaster ResponseNaomi H. Harley, PhDResearch ProfessorDepartment of Environmental MedicineNYU School of MedicineEllen WebbCoordinatorNew York Center for TerrorismPreparednessBellevue Hospital Center
Forward1. What is this guidance document?The aim of this publication, NYC Hospital Guidance to Responding to a ContaminatingRadiation Incident, is to serve as a practical resource for New York City Hospitals inplanning a response to an emergency involving radioactive contamination.This guide was developed by The New York City Hospital Radiation Working Group, amulti-hospital working group convened by the NYC Department of Health and MentalHygiene (DOHMH) that included nuclear medicine, radiation oncology, emergencymedicine, health physics, emergency management, mental health, environmentalmedicine, and radiation-related treatment and monitoring professionals. Every efforthas been made to ensure the information in this manual is accurate and consistentwith sound radiation protection and assessment methods, policies, and practices.2. Are the recommendations in this guideline mandatory?The NYC Department of Health and Mental Hygiene (DOHMH) do not require thathospitals incorporate all the following recommendations verbatim. Rather hospitalsshould develop a radiological emergency plan consistent with their local perceivedradiological threat, while considering their staffing capabilities, equipment resources,and other unique characteristics and condition.3. Why does my hospital need this guideline?The manual assumes that, if a radiological incident occurs, hospitals will activatetheir Hospital Incident Command System (HICS) and the hospital specific emergencyresponse plan. Each plan should include a radiation-specific annex. If a hospital doesnot have a radiation annex, this guideline will assist hospital planners and medicalstaffs create one.Hospitals and their personnel must be able to immediately receive, evaluate andtreat victims. Some victims will be ill and injured; some will be exposed and/orcontaminated while others who have not been exposed will be concerned about theirpotential exposure. With little or no warning and information and limited access toradiation specialists, front line staff will be called upon to make complex decisions inan austere environment. To effectively meet this challenge, adequate planning andpreparation are necessary.While participation by radiation specialists during planning is critical, the assumptionis that adequate numbers of radiation specialists will not be available immediately toperform all essential functions in the event of a radiation emergency. Many tasksmust be delegated to the initially available staff. Hence, the Job Action Sheets andappendices were developed to enable non-radiation specialists to perform theseessential functions.4. My hospital plan is to not permit any radiationcontamination inside, why do I still need a radiation responseannex to my plan?NYC Hospital Guidance for Responding to a Contaminating Radiation Incidenti
Controlling and limiting contamination is vital, but planners and administrators mustunderstand that some radioactive material will inevitably enter the hospitals if alarge scale radiation contaminating incident occurs. The physical properties ofradioactive materials, technical limitations of equipment, demand for immediateclinical care, and relative scarcity of radiation specialists make complete exclusion ofradioactivity impossible. However, following the radiation control recommendationsin this manual the magnitude of contamination should significantly limited, therebypermitting ongoing clinical responsibilities. The manual addresses how to controlsuch contamination, while continuing critical hospital functions and keeping hospitalpersonnel and patients safe.5.Who should read this guideline?The primary audiences for most of the chapters include emergency planners,administrators, security, radiation safety personnel, and emergency departmentpersonnel. The recommendations focus on practical response procedures rather thanon treatment protocols with the exception of Section 7: Radiation Medicine.One of the main goals of this document is to adapt the best available knowledge,which is based on the experience gained from treating small numbers of patients, toa potentially overwhelming number in the midst of the chaos of a mass casualtysituation.Katherine Uraneck, MDProject Manager and EditorSenior Medical CoordinatorHealthcare Emergency Preparedness ProgramNew York City Department of Health and Mental HygieneNYC Hospital Guidance for Responding to a Contaminating Radiation Incidentii
Table of ContentsRadiation Abbreviations & AcronymsviPART ISection 1: Introduction to Planning for a Radiation Incident1 Key Planning Considerations for Radiation Incidents2 Essential Radiation Concepts and Definition3 NYC Radiological Dispersal Device Assumptions8Section 2: Staff Safety during a Radiation Incident9 Occupational Health10 Protective Clothing and Respiratory Protection11 Radiation Protection Practices13 Radiation Dose Limits for Hospital Personnel14 Recommended Occupational Exposure Limits in an Emergency16 Radiation Safety Information Sheet for Staff17 PROCEDURE: PPE Donning and Doffing19 FORM: Employee Exposure Assessment Worksheet21Section 3: Radiation Control-Keeping Facilities Safe during a Radiation Incident 22 Radiation Control General Recommendations23 Radiation Control and Safety Team (RCST)23 RCST Personnel24 Priorities for RCST Members24 oGeneral Priorities for all Members24oPre-Decontamination Area Priorities25oPost-Decontamination Area Priorities25oRadiation Control Treatment Area Priorities26General Radiation Contamination Control Practices26oRED Control Treatment Area Special Considerations28oYELLOW Control Treatment Area Special Considerations29oGREEN Control Treatment Area Special Considerations30 Radiation Safety Officer Responsibilities31 Radiological Surveyors Job Action Sheets (JAS)32oGeneral Radiological Surveyors JASNYC Hospital Guidance for Responding to a Contaminating Radiation Incidentiii32
Table of ContentsoPre-Triage Radiological Surveyors JAS33oPost-Decontamination Radiological Surveyors JAS34oRed Treatment Area Radiological Surveyors JAS35oYellow Treatment Area Radiological Surveyors JAS36oGreen Treatment Area Radiological Surveyors JAS37 Emergency Dept. Schematic for Placement of Radiation Surveyors & Meters38 Establishing Radiation Zones during Radiation Incidents39Section 4: Triage and Patient Flow during a Radiation Incident41 Introduction to Triage42 Medical Triage42 Radiological Triage43 Prioritizing Radiological Screening of Victims44 Hospital Triage Process for Arriving Victims45 Summary Flow Chart of Triage Process47 Treatment Areas Activities Flow ChartsoRed Control Treatment Area Activities48oYellow Control Treatment Area Activities49oGreen Control Treatment Area Activities50 PROCEDURE: Conducting a Rapid Radiological Survey of Crowds51 PROCEDURE: Conducting a Rapid Radiological Screening Survey52 PROCEDURE: Conducting a Full-Body Radiological Survey of an AmbulatoryPerson53 FORM: Post Decontamination Survey Sheet55Section 5: Decontamination of Patients during a Radiation Incident56 Patient Decontamination Procedure Recommendations57 Decontamination Recommendations for Severely Ill or Injured57 Decontamination Recommendations for Stable Patients58 PROCEDURES: Special Decontamination Procedures59 oDecontamination of Localized Skin Contamination59oDecontamination of Eyes59oDecontamination of Burns60oDecontamination of Wounds60oDecontamination of Hairy Areas61oEmbedded Radioactive Particles61PROCEDURE: Decontamination of Non-ambulatory Patients without LifeThreatening ConditionsNYC Hospital Guidance for Responding to a Contaminating Radiation Incidentiv62
Table of Contents PROCEDURE: Decontamination of Expired Victims63 Table of Recommended Patient Decontamination Decisions64Section 6: Equipment for Radiation Incidents65 Descriptions of Survey Meters and Personal Dosimeters66 Table of Suggested E.D. Radiation Equipment and Materials69 Special Considerations for Planning for Equipment and Supplies70Section 7: Training Resources and Competencies for a Radiation Incident71 Introduction72 Essential Training Competencies for First-Receivers72 Training Resources75Part I References80Glossary of Radiological Terms86AppendicesConversions of Conventional and International System of UnitsA-1Appendix 1: Forms, Worksheets, and Handouts 1.a. Radiation Safety Information Sheet for Staff MembersA-2 1.b. Post-Decontamination Survey WorksheetA-4 1.c. Wound Survey WorksheetA-5 1.d. Patient Biodosimetry WorksheetA-6 1.e. Employee Radiation Exposure WorksheetA-8 1.f. Instructions to the Public Waiting for DecontaminationA-9 1.g. Instructions to Perform Decontamination at HomeA-1Appendix 2: Procedures and Protocols 2.a. Portable Radiographic Examination of the Contaminated PatientA-11 2.b. CT or Radiology Suite Radiation SafetyA-12 2.c. Operating Room Radiation SafetyA-13 2.d. Conducting an Area Rapid Radiological SurveyA-14 2.e. Conducting a Rapid Radiological Screening SurveyA-15 2.f. Conducting a Full-Body Radiological Survey on an Ambulatory PatientA-16 2.g. PPE Donning and Doffing ProcedureA-18 2.h. How to Distinguish Between Alpha, Beta, and Gamma Radiation Using aPancake GM Survey MeterA-20Appendix 3: On-line ResourcesNYC Hospital Guidance for Responding to a Contaminating Radiation IncidentvA-21
RADIATION ABBREVIATIONS & IAEAICRPICRUIOMINDJJCAHOAmerican Association of Physicists in MedicineAmerican College of Radiologyas low as reasonably achievableAmerican Medical AssociationAmerican Nuclear SocietyAmerican National Standards InstituteAgency for Toxic Substances and Disease Registrybiological effects of ionizing radiationbequerelCenters for Disease Control and Preventioncommitted effective dose equivalentCode of Federal RegulationscurieConference of Radiation Control Program Directors, Inc.dose and dose-rate effectiveness factor,US Department of Health and Human ServiceUS Department of Homeland Securitydeoxyribonucleic acidUS Department of EnergyNYC Department of Health and Mental Hygienedose-rate effectiveness factorDefense Threat Reduction Agencyelectroencephalogramextremely low frequencyEmergency Management Agreement Compactemergency medical servicesUS Environmental Protection AgencyEmergency Response PlanUS Food and Drug AdministrationFederal Emergency Management AgencyGlobal Information SystemgastrointestinalGrayhigh dose rateHospital Emergency Incident Command SystemHealthcare Emergency Preparedness ProgramHealth Physics SocietyHealth Resources and Services AdministrationInternational Atomic Energy AgencyInternational Commission on Radiological ProtectionInternational Commission on Radiation Units and MeasurementsInstitute of Medicineimprovised nuclear deviceJoint Commission on Accreditation of Healthcare OrganizationsNYC Hospital Guidance for Responding to a Contaminating Radiation Incidentvi
SvTTEDETLDUUAUNSCEARUVVVAWWBCWHOXYZZlow dose ratelinear-energy transferlower limit of detectionmilliremmilliSievertNational Academy of SciencesNational Council on Radiation Protection and MeasurementsNational Incident Management SystemNational Institute of Occupational Safety and HealthNational Institute of Standards and TechnologyUS Nuclear Regulatory AgencyOffice of the Assistant Secretary for Preparedness and ResponseOffice of Radiological HealthOccupational Safety and Health Administrationprotective action guidelinespersonal communication systemUS Public Health Servicepersonal protective equipmentpulsed wavered blood cellsrelative biological effectiveness of a particular treatment to some other treatmentradiological dispersal deviceradiological dispersal eventradiation exposure deviceRadiation Effectiveradiological protective guidelineradiation safety officerInternational System of UnitsSieverttotal effective dose equivalentthermoluminescent dosimeterurine analysisUnited Nations Scientific Committee on the Effects of Atomic RadiationultravioletDepartment of Veterans Affairswhite blood cellsWorld Health Organizationatomic numberNYC Hospital Guidance for Responding to a Contaminating Radiation Incidentvii
NYC Hospital Guidance for Respondingto a Contaminating Radiation IncidentApril 2009PART INYC Hospital Guidance for Responding to a Contaminating Radiation Incidentviii
Section 1: Introduction to Planning for aRadiation IncidentSection Contents: Key Planning Considerations for Radiation Incidents Essential Radiation Concepts and Definitions NYC Radiological Dispersal Devices AssumptionsNYC Hospital Guidance for Responding to a Contaminating Radiation Incident1
Section 1. Introduction to Planning for a Radiation IncidentKey Planning Considerations for Radiation Incidents1. Treatment of life-threatening illness and injury takes precedence overradiological assessment and decontamination. (Burnham and Franco, 2003).2. Detect High Radiation Sources and control contamination. All hospitalemergency departments must have radiation detection equipment and stafftrained to use this equipment immediately available 24 hours a day/ 7 days aweek.3. Universal precautions in the emergency room are usually sufficient fortreatment of victims of radiological incidents. (NCRP, 2006).4. Expect early patients to arrive unannounced. Hospitals must be prepared toreceive contaminated patients with little to no warning.5. Clothing removal eliminates up to 80-90% of contamination. (Levitin et al.,2003).6. Individuals may be advised by public health authorities to self-decontaminateat home if resources do not permit decontamination of large numbers ofpeople. (CRCPD, 2003).7. In a mass casualty event, it is impractical to assume that all radioactivematerial will be kept out of the facility. Plans should be developed for criticalmedical facilities and critical care equipment to continue functioning in lowradiation areas. (CEMSA, 2005).8. Fear of radiation is substantial by both the public and responders. Prioritizingpersonnel safety concerns prior to and during an event will help to put riskhazard into a proper perspective.9. Identify radiation experts during planning phase. The emergency responseplan should identify radiation expertise available to the hospital to facilitateplanning, response, and recovery phases during a radiation incident.NYC Hospital Guidance for Responding to a Contaminating Radiation Incident2
Section 1. Introduction to Planning for a Radiation IncidentEssential Radiation Concepts and DefinitionsRadiation Exposure versus Radiation Contamination of people Radiation Exposure (irradiation): A general term used to express what aperson receives as a result of being exposed to ionizing radiation.The unit ofexposure most often used is the roentgen (R). People who have been exposedto radiation only, are not radioactive AND ARE NOT A RISK TO OTHERS DUE TOSECONDARY CONTAMINATION. Radioactive Contamination: the deposition of unwanted radioactive materialon the surfaces of structures, areas, objects, or people. It can be airborne,external, or internal.Useful analogy of exposure vs. contamination: Let’sallow a camp fire to represent a radioactive source.If you put a Marshmallow near the fire (exposure),the heat (energy) from the fire will begin to brown(damage to the marshmallow). Take themarshmallow away and the browning stops,marshmallow is safe to eat. But drop themarshmallow in the embers and it gets covered withsoot and dirt (contamination), now it is not safe toeat.External Contamination vs. Internal Contamination External Contamination: Radioactive material (liquid, powder, metalfragments, dust) contamination on the body surface or clothing. Externalcontamination may be removed by washing with water or simply taking off theouter layers of clothing. Once external contamination is removed and away fromthe body, it no longer has an effect on the body. Following an RDD event thequantity of radioactive material deposited on an individual is not expected to behigh enough to be immediately life threatening. Internal Contamination: Radioactive material (liquid, powder, metalfragments, or dust) contamination inside the body. Pathways include ingestion,inhalation, injection, or absorption. Internal contamination may be a continuoussource of radiation exposure if radioactive material is incorporated into the bodyand not removed. Certain treatments exist for specific isotopes to lessen theamount of material in the body by either blocking the absorption of the isotope orchelating the material. Everyone has small amounts of radioactive material intheir body either from natural sources (such as potassium or radon) or throughthe uptake of minute amounts of fallout from atomic weapons tests or throughsmoking (polonium). This level of contamination is not treated. Larger amountsof internal contamination are a concern when the amounts might cause acutesymptoms or significantly increase the risk of cancer or other long term effects.NYC Hospital Guidance for Responding to a Contaminating Radiation Incident3
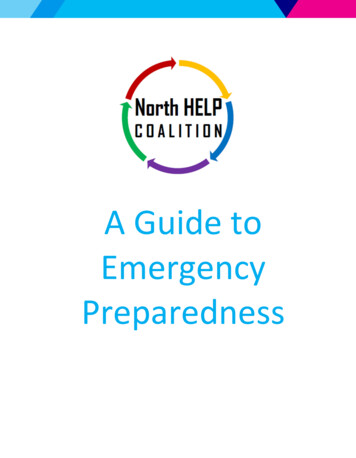
Section 1. Introduction to Planning for a Radiation IncidentTypes of ionizing radiationGamma rays High-energyelectromagnetic radiation emitted bycertain radionuclides when their nucleitransition from a higher to a lower energystate. Gamma rays penetrate tissuefarther than do beta or alpha particles,but are less damaging locally.Beta particles Electrons ejected from thenucleus during radioactive decay. Theyare less penetrating than gamma rays andcan be shielded by a thin sheet of metal.Their chief hazard is ingestion and skincontamination. Beta particles canpenetrate the dead layer of skin andcause severe burns.Alpha particles Equivalent to a heliumnucleus (2 protons and 2 neutrons). Alphaparticles generally carry more energy thangamma rays and beta particles. They areeasily shielded by a sheet of paper orclothing and present no external hazard.Alpha particles are quite damaging ifinternalized because they deposit all oftheir energy in a very small volume oftissue.Hot particles are radioactive fragments that may get embedded in the body. Theexposure from such fragments can cause severe local injury and possiblyconsequential whole body exposure unless they are removed. Removal of clothingand showering should remove any not embedded in the body, but the remaindermay require surgical removal.NYC Hospital Guidance for Responding to a Contaminating Radiation Incident4
Section 1. Introduction to Planning for a Radiation IncidentSelected Radiation Measurement UnitsFor more information, see Primer on Radiation Measurement in Appendix Rad: (Radiation Absorbed Dose) The rad is a special unit of absorbed radiationdose. It is a measure of the amount of energy absorbed per unit mass(energy/gram) body. The rad is the traditional unit of absorbed dose but is beingreplaced by the Standard International (SI) unit, the Gray (Gy). One Gray isequal to 100 rad. See Glossary Gray: The Gray is the SI unit of dose absorbed energy per unit mass(Joules/Kg). 100 rad 1 Gray (Gy). See Glossary Rem: The rem is a unit of absorbed dose that attempts to normalize the dosefrom different types of radiation exposure. See Glossary Sievert: The Sievert is the SI unit used to normalize the dose from alpha, betaand gamma radiation exposures. See GlossaryRadiation Dose: a generic term to describe the amount of radiation absorbed by aperson’s body. Dose is measured in units of thousands of a roentgen equivalent man(rem) Dose is a general term used to assist in the management of individualexposure to radiation. The international scientific community has adopted the use ofa different term for millirem called a milliSievert (mSv). One mSv is the same as 100mrem.Radiation Health EffectsDeterministic Effects (Acute) vs. Stochastic Effects (Delayed) Deterministic effects: effects that can be related directly to the radiation dosereceived. The severity increases as the dose increases. A deterministic effecttypically has a threshold below which the effect will not occur. Examples of adeterministic effect are acute radiation syndrome or hair loss. Almost allimmediate safety measures are aimed at preventing acute or deterministiceffects. Stochastic effect: effect that occurs on a probabilistic basis directly related tothe size of dose. The effect typically has no threshold and is based onprobabilities, with the chances of seeing the effect increasing as the dose ofradiation increases. If it occurs, the severity of a stochastic effect is independentof the dose received. Stochastic effects appear years after the exposure. Canceris a stochastic effect.High Dose vs. Low Dose High doses can generally be considered any dose of radiation that can causeacute deterministic effects. Typically, 10 rem – 15 rem causes fetalabnormalities and decrease in sperm count. For Acute Radiation Syndrome thedose is approximately 100 rem 1 Sv. Low doses are doses that do not produce acute deterministic effects. Below 5 rem(the yearly occupational maximum dose for radiation workers) would beconsidered a low dose. Low dose radiation can still result in long term effects.NYC Hospital Guidance for Responding to a Contaminating Radiation Incident5
Section 1. Introduction to Planning for a Radiation IncidentRULE OF THUMB:Deterministic effects start at HIGH DOSES (see above). After a personhas reached the threshold for a given effect, the more radiation, theworse the effect. Acute Radiation Syndrome is an example of an AcuteEffect. All the Protective Action Guidelines for Responders are aimed atpreventing Acute Effects. Acute usually means the effects occur withinin minutes to months of the exposure.Stochastic effects are health effects that occur over the long term, yearsand generations later. These are the effects that may or may not be seenwith and doses including LOW DOSES (see above). These effects onlyincrease in probability as the dose goes up, not severity. For example, astochastic effect would be the risk of getting leukemia after a total bodyexposure, and the leukemia would not be worse if the dose is higher,just a greater probability of getting it.Pregnancy, Children and Radiation Rapidly dividing cells are more sensitive to the effects of radiation. Thereforefetuses, newborns, and children are more susceptible earlier in development themore susceptible to radiation therefore children and Fetuses are most sensitive toradiation during 8-15 weeks following conception. Children and fetuses are moresensitive to radiation because their cells divide at a more rapid rate and there is agreater opportunity for radiation to disrupt this process.Clinical Status Medical emergency: a condition in which the absence of immediate medicalattention could reasonably result in serious dysfunction, impairment of bodilyfunction, or loss of life. Medical urgency: A condition that requires attention, but delay in care will notresult in serious dysfunction, impairment of bodily functions or loss of life.Treatment Areas Pre-decontamination Area: An area designated outside of thedecontamination zone where patients may or may not be contaminated. Post-decontamination Area: Area located immediately after decontaminationshowers where a repeat radiation screening is completed prior to sending patienton to treatment areas or back through decontamination showers. Red (Radiation Controlled) Treatment Area: The designated treatmentarea(s) for critically ill and injured patients who may have received minimal or nodecontamination and screening prior to entry. Radiation Control and screeningprocedures will be required for this area and should receive the highest priorityfor assigning radiation detection equipment. Yellow (Radiation Controlled) Treatment Area: The designated treatmentarea for Non-critically ill or injured patients requiring some medical interventionNYC Hospital Guidance for Responding to a Contaminating Radiation Incident6
Section 1. Introduction to Planning for a Radiation Incidentor hospitalization. Patients should have undergone maximum decontaminationprior to entry. However, some radioactive contamination may enter this area.This area should have little to no contamination, but it is still possible thatradiation contamination may be inadvertently tracked in and, therefore, radiationcontrol practices should be in place. Additionally, special radiation procedures willbe required for this area, for example, treatment of contaminated wounds. Green (Radiation Controlled) Treatment Area: The designated treatmentarea(s) for Patients with minimal or no physical illness or injury. Patients shouldbe maximally decontaminated prior to entry to this area, but inadvertent trackingof radiation contamination is possible. Radiation Control Zones: These zones are not predefined areas, but locationswhere the ambient radiation dose rates exceed prescribed levels. For example, aheavily contaminated individual may result in a hot zone surrounding his/herstretcher, but the areas farther away may be within normal limits for the public.These designations will be dynamic and need to be determined in real time by thedesignated radiation control team. Designation of radiation control Zones definesthe activities, personnel, and access within that zone. See Section for 3 for Tableof Radiation Zones, Stay Times, and Activities. For more information aboutRadiation Control Zones go to Section 3. Radiation Control—Keeping FacilitiesSafe during a Radiation Incident. Extreme Radiation Zone: 10,000 mrem/hrHigh Radiation Zone: 1000 - 10,000 mrem/hrMedium Radiation Zone: 100 - 1000mrem/hrLow Radiation Zone: 2 -100mrem/hrNot controlled 2mrem/hr (approximately 1,000 cpm)Background Radiation: the amount of ionizing radiation from natural sources, suchas terrestrial radiation due to radionuclides in the soil, stone, or cosmic radiationoriginating from space. Radon is the greatest contributor to background radiation.NYC Hospital Guidance for Responding to a Contaminating Radiation Incident7
Section 1. Introduction to Planning for a Radiation IncidentRadiological Dispersal Devices (RDD) AssumptionsThese assumptions were utilized for the basis of all of the recommendations in thisguidance document.1. The inhalation hazard is greatest for those close to the site of an explosion.After the explosion, airborne radioactive material should dissipate within 1015 minutes. (Mussolino and Harper, 2006).2. The principal hazard to patients and responders in the immediate area of theexplosion will be from radioactive material on the ground and buildings andespecially from highly radioactive fragments (hot particles) if they arepresent.(Mussolino and Harper, 2006).3. For the most plausible scenarios, the high-risk area is approximately 500meters (about 7 small city blocks) from the blast point. This is expected to bemade smaller as first responders and environmental tests refine and surveythe area. (Mussolino and Harper, 2006).4. Safe and controlled evacuation of potentially contaminated areas is a higherpriority than decontamination during the immediate phase of anincident.(Mussolino and Harper, 2006).5. The affected population within the immediate vicinity of an RDD will bedirected away from the blast using all available routes, as long as the routesdo not traverse the blast area.6. Isotopic identification will be conducted by city agencies with subsequentcommunication to the hospitals through the City Incident ManagementSystem.7. Evacuation Areas will most likely change over the course of days to severalweeks after an incident based on the Environmental Protection Agency (EPA)Intermediate and Late Phase Protective Action Guidelines (PAG).8. Hospita
NYC Hospital Guidance for Responding to a Contaminating Radiation Incident i Forward 1. What is this guidance document? The aim of this publication, NYC Hospital Guidance to Responding to a Contaminating Radiation Incident, is to serve as a practical resource for New York City Hospitals in planning a response to an emergency involving radioactive contamination.