Transcription
Suggested Fee Guidefor Dental HygienistsJanuary 1, 2020 2020 Ontario Dental Hygienists’ AssociationAll rights reserved
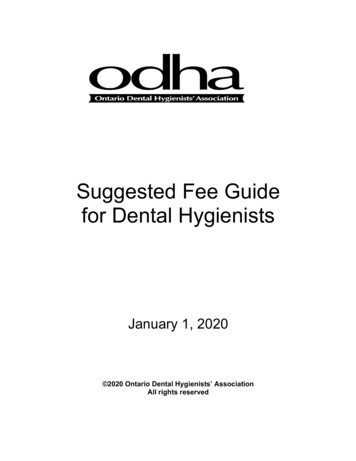
USER GUIDE FOR DENTAL HYGIENISTSThe content, organization and management of dental hygiene care is guided by the principle of accessibility for all Canadians tocomprehensive oral health care and the promotion of oral health as an integral component of general health.The purpose of this Fee Guide is to provide guidance to dental hygienists practising independently in Ontario in setting the feesthey charge for their professional services. It is a guide only; adherence to the guide is not obligatory. Each dental hygienist willset his or her fees to reflect practice realities and local circumstances and requirements. Dental hygienists are expected tofollow their code of ethics and standards of practice when determining the value of a dental hygiene service.This Fee Guide uses the CDHA National List of Service Codes that has been produced by the Canadian Dental HygienistsAssociation (CDHA). The CDHA National List of Service Codes provides a description of the expectations of service for thecodes used in this Fee Guide. The ODHA Fee Guide is not intended for use by dental hygienists employed within traditionaldental offices.Dental Hygiene Claim FormTo protect themselves from copyright infringements, it is important that all Ontario dental hygienists who are submittinginsurance claims use either the standard dental hygiene claim form attached to this Fee Guide and available on the ODHAwebsite or if they are members of CDHA, the CDHA Dental Hygiene Claim Form.ReviewODHA will periodically review the suggested fees and will submit any suggestions for the coding system to the CDHA so it cantake these under advisement in its own review. Members are encouraged to submit their evidence-based feedback to theODHA in writing.Members and third parties are reminded the suggested fees contained in the Fee Guide were prepared by the Ontario DentalHygienists’ Association to provide a guideline of fees considered to be fair and reasonable. The suggested fees are a guidelineonly. The suggested fees are not binding on any dental hygienist or third party billing or paying for dental hygiene services, andthere is no obligation to follow the suggested fees in the Fee Guide. 2020 Ontario Dental Hygienists’ AssociationAll rights reserved. No part of this work covered by the publisher’s copyright may be reproduced or copied in any form or by any means(graphic, electronic or mechanical, including photocopying, recording, recording taping, or information and retrieval systems) without thewritten permission of the publishers. 2020 Ontario Dental Hygienists’ AssociationAll rights reservedPage 2 of 8
In this fee guide:‘ lab’§ means that an additional laboratory expense may be assessed with the procedure code§ the code for laboratory expense is 00991‘ exp’§ means that additional expenses such as courier costs may be assessed with the procedure code§ the code for an additional expense is 00992‘c.s.’§ means that the fee is client specific and determined by the individual time and circumstances of the service provided‘tooth number’§ when a service code requires a “tooth number”, the 2-digit International System of tooth numbering is to be usedCode / ServiceODHA 2020 suggested fee00100 Dental hygiene examination/assessment and diagnosisPrimary, complete00111 45.00Mixed, complete00112 70.00Permanent, complete00113 100.34Edentulous, complete00114 42.00Periodontal, complete00115 70.00Case presentation/treatment planning – unusually complicated case – (each unit of time is 15 minutes)1 unit of time00116 39.922 units of time00117 79.833 units of time00118 119.75each additional unit of time 300119 39.9200120 Limited dental hygiene examination/assessment and diagnosisRoutine reassessment/recall (previous client)00121 29.28Emergency00123 32.28 to 65.86Periodontal, limited, previous client00124 32.28 to 65.86 32.28 to 65.86Specific (new or existing client)00125 32.28 to 65.86Limited, new client0012600130 First dental hygiene visit/orientation00131 25.00Radiographs and photographs (including interpretation for purposes00200 of dental hygiene diagnosis)00210 Intraoral bitewing1 image00211 20.072 images00212 23.203 images00213 26.344 images00214 29.485 images00215 32.616 images00216 35.7500220 Intraoral periapical1 image00221 20.072 images00222 23.203 images00223 26.344 images00224 29.485 images00225 32.616 images00226 35.757 images00227 38.888 images00228 42.02each additional image 800229 3.1400230 Intraoral, full mouth seriesminimum 14 images00231 83.17 2020 Ontario Dental Hygienists’ AssociationAll rights reservedPage 3 of 8
ODHA 2020 suggested feeCode / Service00240 Panoramic1 image00241 59.580025100259 55.26 18.8100250 Cephalometric1 imageeach additional image 100260 Duplication of radiographs1 image2 images3 images4 images5 images6 images7 images8 imageseach additional image 8002701 photo2 photos3 photoseach additional photograph 30030000310bacteriological test00320microbiological test00330oral cavity cytological smearoral mucosal tissue vital stainingoral mucosal tissue direct fluorescence003401 unit of time2 units of time½ unit of timeeach additional unit of time 200400impression(s) – maxilla and/or mandiblefabrication/pouring/preparing casts00500005101 unit of time2 units of time3 units of time4 units of time5 units of time6 units of time½ unit of timeeach additional unit of time 6005201 unit of time2 units of time3 units of time4 units of time 2020 Ontario Dental Hygienists’ AssociationAll rights reserved00261 12.5400262 13.5400263 14.5400264 15.5600265 16.5600266 17.5600267 18.5600268 19.5700269 1.00Photographs for purposes of dental hygiene diagnosis00271 18.8100272 22.5800273 26.3400279 3.76Tests/Analysis and laboratory procedures/interpretationCaries susceptibility test00311 25.00 to 41.65 labPeriodontal disease activity test00321 25.00 to 41.65 labOral cancer testing (technical procedure only)00331 40.00 lab exp00332 40.0000333 40.00Non-ionizing scanning procedure (each unit of time is 15 minutes)00341 43.9000342 87.7900347 21.9500349 43.90Study models (for diagnostic purposes)00401 35.7500402 17.87 labPeriodontal treatment (each unit of time is 15 minutes)Debridement00511 55.6100512 111.2200513 166.8300514 222.4400515 278.0500516 333.6600517 28.3100519 55.61Root planing00521 55.6100522 111.2200523 166.8300524 222.44Page 4 of 8
ODHA 2020 suggested feeCode / Service5 units of time6 units of time½ unit of timeeach additional unit of time 600525005260052700529 278.05 333.66 28.31 55.6100531005320053700539 31.71 63.41 15.85 31.7100530 Stain removal1 unit of time2 units of time½ unit of timeeach additional unit of time 200540 Subgingival periodontal irrigation1 unit of time½ unit of timeeach additional unit of time005501 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 4005601 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 4005701 sextant2 sextants3 sextants4 sextants5 sextants6 sextants005801 unit of time½ unit of timeeach additional unit of time00600006011st tooth in quadranteach additional tooth in quadrant006051 unit of time½ unit of timeeach additional unit of time00610Topical varnish in-officeAll other in-office fluoride products use code 00616Supervised, self-administered in-officeHome - custom maxillary archHome - custom mandibular arch 2020 Ontario Dental Hygienists’ AssociationAll rights reserved00541 50.3700547 25.1800549 50.37Management of oral mucosal disorders00551 39.9200552 79.8300553 119.7500554 159.6700557 19.9600559 39.92Management of oral manifestation of systemic disease00561 39.9200562 79.8300563 119.7500564 159.6700567 19.9600569 39.92Gingival curettage00571 55.6100572 111.2200573 166.8300574 222.4400575 278.0500576 333.66Chemotherapeutic / Photodisinfection therapy00581 53.57 exp00582 26.79 exp00583 53.57 expOther oral services (each unit of time is 15 minutes)Sealants – must include tooth number(s)00602 24.5900603 13.97Application of anticariogenic/antimicrobial agents to hard tissues00606 43.90 exp00607 21.95 exp00609 43.90 expFluoride applications00611006120061300614 25.00 18.06 52.69 lab exp 52.69 lab expPage 5 of 8
ODHA 2020 suggested feeCode / ServiceHome - custom combinedTopical fluoride in-office, all products except varnish006201 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 400630preformed – maxillary archpreformed – mandibular archpreformed – maxillary & mandibular archescustom – maxillary archcustom – mandibular archcustom – maxillary & mandibular arches00638labeling removable prosthesis006401 unit of time2 units of time½ unit of timeeach additional unit of time 2006501 unit of time2 units of time3 units of time½ unit of timeeach additional unit of time 300660maxillary archmandibular archmaxillary and mandibular arches00665Interim Stabilization Therapy (IST)– 1st tooth in quadranteach additional tooth same quadrant - all procedures1st tooth – all other temporary restorations00675one surfaceeach surface 1006801 unit of time2 units of time3 units of timeeach additional unit of time 3006901 unit of time½ unit of timeeach additional unit of time 2020 Ontario Dental Hygienists’ AssociationAll rights reserved0061500616 75.25 lab exp 24.10006210062200623006240062700629 33.87 67.73 101.60 135.46 16.93 33.87006310063200633006340063500636 25.09 exp 25.09 exp 37.63 exp 94.06 lab exp 94.06 lab exp 112.89 lab exp00638 43.90 exp00641006420064700649 43.90 87.79 21.95 43.900065100652006530065700659 50.30 exp 100.59 exp 150.88 exp 25.16 exp 50.30 expFinishing restorationMouth protectorsLabeling removable prosthesisDesensitizationWhitening vital teeth in officeWhitening vital teeth at home00661 150.52 lab exp00662 150.52 lab exp00663 219.50 lab expPlacement temporary restorations – must include tooth number(s)006660066700669 63.47 32.44 63.470067600677c.s.(client specific)c.s.Resin infiltrationPulp vitality testing00681 41.3900682 82.7800683 124.1700689 41.39Denture/removable prosthesis prophylaxis and stain removal00691 50.1700697 25.0900699 50.17Page 6 of 8
Code / Service1 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 4regional blocktrigeminal division blocksupraperiosteal infiltration1 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 41 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 41 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 41 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 41 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 4 2020 Ontario Dental Hygienists’ AssociationAll rights reservedODHA 2020 suggested fee00700 Pain management (each unit of time is 15 minutes)00710 Electronic dental anaesthesia00711 41.3900712 45.5300713 49.6700714 53.8100717 34.7000719 4.1400720 Local anaesthesia00721 15.0500722 15.0500723 15.0500730 Acupuncture00731 41.3900732 45.5300733 49.6700734 53.8100737 34.7000739 4.1400740 Nitrous oxide, conscious sedation00741 62.7200742 125.4300743 188.1500744 250.8600747 31.3600749 62.7200800 Education and habit modification (each unit of time is 15 minutes)00810 Counseling for diet related to oral health00811 43.9000812 87.7900813 131.7000814 175.6000817 21.9500819 43.9000820 Counseling for tobacco use cessation00821 43.90 exp00822 87.79 exp00823 131.70 exp00824 175.60 exp00827 21.95 exp00829 43.90 exp00830 Counseling for oral self-exam00831 43.9000832 87.7900833 131.7000834 175.6000837 21.9500839 43.90Page 7 of 8
Code / ServiceODHA 2020 suggested fee00840 Instruction in oral self care1 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 408501 unit of time2 units of time3 units of time4 units of time½ unit of timeeach additional unit of time 4008601 unit of time2 units of timeeach additional unit of time 200900009101 unit of time2 units of time½ unit of timeeach additional unit of time 2009201 unit of time2 units of time½ unit of timeeach additional unit of time 200950Home visitInstitutional visitEmergency home visitEmergency institutional visit009601 unit of time2 units of time3 units of time4 units of timeeach additional unit of time 4009701 unit of time2 units of timeeach additional unit of time 200990 lab exp 2020 Ontario Dental Hygienists’ AssociationAll rights reserved00841 43.9000842 87.7900843 131.7000844 175.6000847 21.9500849 43.90Group presentations (including preparation)00851 43.9000852 87.7900853 131.7000854 175.6000857 21.9500859 43.90Orofacial myofunctional therapy00861 60.3200862 120.6300869 60.32Outcome evaluation (each unit of time is 15 minutes)Evaluation of dental hygiene care00911 43.9000912 87.7900917 21.9500919 43.90Professional communications / Case presentations00921 43.9000922 87.7900927 21.9500929 43.90Mobile services00951 36.58 to 73.1900952 36.58 to 73.1900953 55.19 to 103.5000954 55.19 to 103.50Exceptional client management (complex or time-intensive) (eachunit of time is 15 minutes)00961 64.0200962 128.0100963 192.0200964 256.0300969 64.02Consultation with client00971 43.9000972 87.7900979 43.90Laboratory and expense services0099100992Page 8 of 8
Top section of form is completed by dental hygienist :DENTAL HYGIENE PRACTICELast name:CLIENTFirst name:Address:Unit/Apt#:City:Prov:Postal Code:For additional notes, assessment, special considerations:Standard Dental Hygiene Claim FormCDHO Registration #I hereby assign my benefits payable from thisclaim to the dental hygienist identified hereand authorize payment directly to him/her.Name:Address:Suite#:City:Prov:Postal Code:Telephone:Fax:(signature of subscriber)I understand that the fees listed in this claim may not be covered by my plan or may exceed the benefits of myplan. I acknowledge that I am responsible for the total fee shown below to the dental hygienist identified aboveand further acknowledge that the said fee is accurate. I agree to the release by the dental hygienist of any information necessary with respect to this claim to my insurance company or plan administrator.(signature of client/parent/guardian)Service provided:Date of servicedaymoyrDescription of service providedIntl.ToothcodeProcedure codeDental hygienist’sfeeThis is an accurate statement of services performed and the total fee dues and payable:Laboratory orExpense chargeTotalTotal fee for ��—————————————— CDHO reg’n# —————————(dental hygienist signature)Employee/Plan member/Subscriber Information:Group policy/plan#EmployerDivision/section#Employee/plan member/subscriber name (please mployee/member/subscriber date of birthdaymoyearClient Information:Relationship to employee/plan member/subscriberClient date of birth dayAre any of the services provided under any other Group Insurance, Dental, WSIB or Government Plan?Is any of the required treatment as the result of an accident?moyear(if not self) yesIf yes, plan name and # no yesIf yes, provide details separately noIf child: studentName of school disabledI hereby authorize the release of any information or records requested in respect of this claim to the insurer/plan administrator and certify that the information given is true,accurate and complete to the best of my knowledge.signature of employee/plan member/subscriberdate
00130 First dental hygiene visit/orientation 00131 25.00 00200 Radiographs and photographs (including interpretation for purposes of dental hygiene diagnosis) 00210 Intraoral bitewing 1 image 00211 20.07 2 images 00212 23.20 3 images 00213 26.34 4 images 00214 29.48 5 images 00215 32.61 6 images 00216 35.75