![Malawi 2015-16 Demographic And Health Survey - Key Findings [SR237]](/img/37/sr237.jpg)
Transcription
Malawi2015-16 Demographic and Health SurveyKey Findings
The 2015-16 Malawi Demographic and Health Survey (2015-16 MDHS) was implemented by the NationalStatistical Office from 19 October 2015 to 18 February 2016. The funding for the 2015-16 MDHS was providedby the government of Malawi, the United States Agency for International Development (USAID), the UnitedNations Children’s Fund (UNICEF), the Malawi National AIDS Commission (NAC), the United NationsPopulation Fund (UNFPA), UN WOMEN, Irish Aid, and the World Bank. ICF provided technical assistancethrough The DHS Program, a USAID-funded project providing support and technical assistance in theimplementation of population and health surveys in countries worldwide.Additional information about the 2015-16 MDHS may be obtained from the Demography and Social StatisticsDivision, National Statistical Office, Chimbiya Road, P.O. Box 333, Zomba, Malawi (telephone: 265-1-524377; e-mail: enquiries@statistics.gov.mw; Internet: www.nsomalawi.mw).Additional information about The DHS Program may be obtained from ICF, 530 Gaither Road, Suite 500,Rockville, MD 20850, USA (telephone: 1-301-407-6500; fax: 301-407-6501; e-mail: info@DHSprogram.com;Internet: www.DHSprogram.com).Recommended citation:National Statistical Office (NSO) [Malawi] and ICF. 2017. 2015-16 Malawi Demographic and Health Survey KeyFindings. Zomba, Malawi, and Rockville, Maryland, USA. NSO and ICF.Cover art: ‘“Lake Scenery” 2016 Steve Bakali. Used with permission.Cover photograph: 2017 Lusungu Chisesa of NSO Malawi. Used with permission.
About the 2015-16 MDHSThe 2015-16 Malawi Demographic and Health Survey (MDHS) is designed to provide data for monitoring thepopulation and health situation in Malawi. The 2015-16 MDHS is the fifth Demographic and Health Surveyconducted in Malawi since 1992. The objective of the survey is to provide reliable estimates of fertility levels,marriage, sexual activity, fertility preferences, family planning methods, breastfeeding practices, nutrition,childhood and maternal mortality, maternal and child health, HIV/AIDS and other sexually transmittedinfections (STIs), women’s empowerment, and domestic violence that can be used by programme managersand policymakers to evaluate and improve existing programmes.Who participated in the survey?A nationally representative sample of 24,562 women age 15-49 in 26,361 selected households and 7,478 menage 15-54 in one-third of the selected households were interviewed. This represents a response rate of 98% ofwomen and 95% of men. The 2015-16 MDHS provides reliable estimates at the national and regional levels,for urban and rural areas, and for each of the 28 districts.2015-16 Malawi Demographic and Health SurveyPage 1
Characteristics of Households and RespondentsHousehold CompositionThe average household size in Malawi is 4.5members. Three in ten households are headedby women. Nearly half (48%) of the Malawianpopulation is under age 15.Water, Sanitation, and ElectricityNearly 9 in 10 households have access to animproved source of drinking water. Almost allhouseholds in urban areas have access to animproved source of drinking water, comparedto 85% of rural households. Over half (52%) ofhouseholds in Malawi use improved sanitation. Ruralhouseholds are more likely than urban householdsto use improved sanitation (53% versus 45%).Forty-eight percent of households use unimprovedsanitation—31% use a shared facility, 11% use anunimproved facility, and 6% have no facility. Only11% of Malawian households have electricity. Half ofurban households have electricity, compared to 4% ofrural households.Water, Sanitation, and Electricity by ResidencePercent of households with:Total Urban Rural878545534911ImprovedImprovedsource ofsanitation facilitydrinking waterOwnership of GoodsMore than half of Malawian households have amobile telephone, 41% have a radio, and 12% havea television. Urban households are more likely thanrural households to own a mobile telephone, radio,or television. In contrast, rural households are morelikely to own agricultural land or farm animals thanurban households.Education9852 2010 Sally Zweimueller, Courtesy of Photoshare4ElectricityTwelve percent of women and 5% of men age 15-49have no education. Nearly 6 in 10 women and menhave attended primary school, while 23% of womenand 32% of men have attended secondary education.Only 3% of women and 5% of men have more thansecondary education. About three-quarters of womenand 83% of men are literate.EducationPercent distribution of women and men age 15-49by highest level of education attended323532More thansecondarySecondary6212WomenPage 2585MenPrimaryNo education2015-16 Malawi Demographic and Health Survey
Fertility and Its DeterminantsTotal Fertility RateTrends in FertilityBirths per woman for the three-yearperiod before the surveyCurrently, women in Malawi have an average of4.4 children. Since 1992, fertility has decreased from6.7 children per woman to the current level. Thisdemonstrates a dramatic decline of 2.3 children.Fertility varies by residence and district. Women inrural areas have an average of 4.7 children, comparedto 3.0 children among women in urban areas. Fertilityis lowest in Blantyre (3.4 children per woman) andhighest in Machinga (6.6 children per woman).Fertility also varies with education and economicstatus. Women with no education have 3.2 morechildren than women with more than secondaryeducation (5.5 versus 2.3). Fertility decreases as thewealth of the respondent’s household* increases.Women living in the poorest households have anaverage of 5.7 children, compared to 2.9 childrenamong women living in the wealthiest ths per woman for the three-yearperiod before the surveyBirths per woman for the three-yearperiod before the survey4.12.9Lowest Second Middle Fourth 5.1 Lilongwe 5.63.8 Dedza4.4 Mangochi tMalawi4.4Rumphi4.6Mzimba3.9Nkhata Bay4.5Likoma3.6Total Fertility Rate by Household Wealth5.22010 2015-16MDHS MDHSTotal Fertility Rate by DistrictChitipa4.5 Karonga4.35.75.7Kasungu4.5* Wealth of families is calculated through household assets collected from DHS surveys—i.e., type of flooring; source of water;availability of electricity; possession of durable consumer goods. These are combined into a single wealth index. They are then dividedinto five groups of equal size, or quintiles, based on their relative standing on the household wealth index.2015-16 Malawi Demographic and Health SurveyPage 3
Age at First Sex, Marriage, and BirthPolygynyMalawian women begin sexual activity 1.7 yearsbefore Malawian men. The median age at firstsexual intercourse for women age 25-49 is 16.8years, compared to 18.5 years among men age 25-49.Women with more than secondary education initiatesex 3.7 years later than women with no education(19.7 years versus 16.0 years). Nearly two-thirds ofwomen begin sexual activity before age 18, while 1 in5 has sex before age 15.Thirteen percent of Malawian women age 15-49 arein a polygynous union. Polygyny is most commonamong women with no education (21%). Sevenpercent of men age 15-49 are in a polygynous union.Women get married 1.4 years after sexual initiationat age 18.2. Malawian men marry much later thanwomen at a median age of 23.0 years. Women withno education marry 7.2 years earlier than womenwith more than secondary education (17.6 yearsversus 24.8 years). Nearly half (47%) of Malawianwomen are married by age 18.Within one year of marriage women are having theirfirst birth. The median age at first birth for womenis 19.0 years. Women with more than secondaryeducation have their first birth 6.3 years later thanwomen with primary or no education (24.9 yearsversus 18.6 years).Median Age at First Sex, Marriage, and BirthAmong women and men age 25-49Women MenTeenage ChildbearingIn Malawi, 29% of adolescent women age 15-19are already mothers or pregnant with their firstchild. Teenage fertility is higher in rural areas (31%)than urban areas (21%). Adolescent women in thepoorest households are nearly three times as likelyas those in the wealthiest households to have begunchildbearing (15% versus 44%).Teenage Childbearing by Household WealthPercent of women age 15-19 whohave begun childbearing4435312515Lowest Second Middle Fourth HighestPoorestWealthiest23.016.818.5Medianage atfirst sexPage 418.2Medianage at firstmarriage19.0naMedianage atfirst birth2015-16 Malawi Demographic and Health Survey
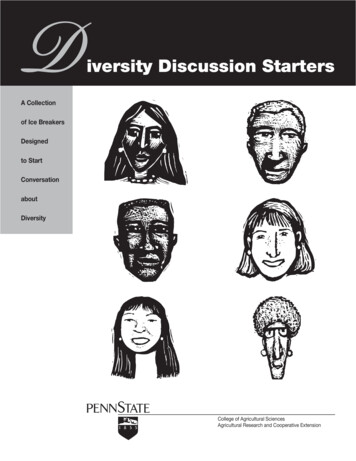
Family PlanningCurrent Use of Family PlanningFamily PlanningAbout 6 in 10 married women age 15-49 use amethod of family planning—58% use a modernmethod and 1% use a traditional method. Injectablesare the most popular modern method (30%),followed by implants (12%), and female sterilisation(11%).Among sexually active, unmarried women age 1549, 43% use a modern method of family planningand 1% use a traditional method. The most popularmethods among sexually active, unmarried womenare injectables (15%), the male condom (14%), andimplants (6%).Use of modern methods of family planning variesby district. Modern method use ranges from a lowof 31% in Mangochi to a high of 68% in Chiradzulu.Modern contraceptive use increases with wealth; 53%of women from the poorest households use a modernmethod of family planning, compared to 61% ofwomen from the wealthiest households.Percent of married women age 15-49using family planningAny method59Any modern method58Implants12Female sterilisation11Any traditional method 1Current Use of Modern Methods by DistrictPercent of married women age 15-49 usinga modern method of family planningChitipa62% Karonga60%Percent of married women age 15-49using family planning100806040Any method20Any modern 015-16 Malawi Demographic and Health SurveyMalawi58%Rumphi63%Mzimba52%Nkhata Bay40%Likoma63%The use of any method of family planning by marriedwomen has dramatically increased from 13% in 1992to 59% in 2015-16. Similarly, modern method use hasincreased eightfold from 7% to 58% during the sametime period.Trends in Family Planning ji62% Lilongwe 53%66% Dedza62% Mangochi ge 5
Demand for Family PlanningMore than one-third of married women want todelay childbearing (delay first birth or space anotherbirth) for at least two years. Additionally, 41% ofmarried women do not want any more children.Women who want to delay or stop childbearing aresaid to have a demand for family planning. The totaldemand for family planning among married womenin Malawi is 78%.The total demand for family planning includes bothmet and unmet need. Met need is the contraceptiveprevalence rate. In Malawi, 59% of married womenuse any family planning method—58% use amodern method and 1% use a traditional method.Unmet need for family planning is defined as theproportion of married women who want to delay orstop childbearing but are not using family planning.Nearly 1 in 5 married women in Malawi have anunmet need for family planning: 11% want to delaychildbearing, while 8% want to stop childbearing.Demand for Family Planning Satisfied byModern MethodsDemand satisfied by modern methods measuresthe extent to which women who want to delay orstop childbearing are actually using modern familyplanning methods. Three-quarters of the demandfor family planning in Malawi is satisfied by modernmethods.Both total demand for family planning and demandsatisfied by modern methods have increased since1992. This indicates that even as more women havea demand for family planning, the gap between totaldemand and demand satisfied is getting narrower—more women need family planning and are usingmodern methods.Page 6Trends in Demand for Family PlanningAmong married women age 15-49, percent withdemand for family planning and demand satisfiedby modern methods10080Total demand6040201992MDHS2000MDHSDemand satisfied bymodern methods20042010 2015-16MDHS MDHS MDHSExposure to Family Planning MessagesThe most common media source of family planningmessages is the radio. Four in ten women and 64% ofmen heard a family planning message on the radio inthe few months before the survey. Women and menwere much less likely to have seen a family planningmessage on television or in a newspaper/magazine.Overall, 42% of women and 17% of men were notexposed to family planning messages via any mediasource.Informed ChoiceFamily planning clients should be informed aboutthe side effects of the method used, what to do if theyexperience side effects, and told about other availablefamily planning methods. More than three-quartersof women were informed of possible side effects orproblems of their method, 73% were informed aboutwhat to do if they experience side effects, and 86%were informed of other available family planningmethods.2015-16 Malawi Demographic and Health Survey
Childhood MortalityRates and TrendsInfant and under-5 mortality rates for the five-yearperiod before the survey are 42 and 63 deaths per1,000 live births, respectively. At these mortalitylevels, 1 in every 16 Malawian children does notsurvive to their fifth birthday.Childhood mortality rates have declined since 1992.Infant mortality has decreased from 135 deaths per1,000 live births in 1992 to 42 in 2015-16. During thesame time period, under-5 mortality has markedlydeclined fourfold from 234 to 63 deaths per 1,000 livebirths.Trends in Childhood MortalityDeaths per 1,000 live births for thefive-year period before the survey250200Under-5 mortality150100Infant MDHSMortality Rates by BackgroundCharacteristicsThe under-5 mortality rate differs by residence,district, and household wealth for the ten-year periodbefore the survey. Children in rural areas are morelikely to die young (77 deaths per 1,000 live births)than children in urban areas (60 deaths per 1,000live births). Under-5 mortality also varies by district,from 51 deaths per 1,000 live births in Mwanza to123 deaths per 1,000 live births in Mchinji. Under-5mortality is higher among children in the pooresthouseholds (83 deaths per 1,000 live births) thanamong children in the wealthiest households (60deaths per 1,000 live births).2015-16 Malawi Demographic and Health Survey 2008 Fletcher Gong’a, Courtesy of PhotoshareBirth IntervalsSpacing children at least 36 months apart reducesthe risk of infant death. The median birth intervalin Malawi is 41.0 months. Infants born less thantwo years after a previous birth have high under-5mortality rates. Under-5 mortality is dramaticallyhigher among children born less than two years aftera previous birth (123 deaths per 1,000 live births)than among children born three or more years aftera previous birth (54 deaths per 1,000 live births).Overall, 12% of children are born less than two yearsafter their siblings.Under-5 Mortality by Previous Birth IntervalDeaths per 1,000 live births for theten-year period before the survey12373 2 years2 years54563 years4 yearsPage 7
Maternal HealthAntenatal CareNearly all (95%) of women age 15-49 receiveantenatal care (ANC) from a skilled provider(doctor, clinical officer, medical assistant, nurse, andmidwife). The timing and quality of ANC are alsoimportant. One-quarter of women had their firstANC visit in the first trimester, as recommended.Half of women made four or more ANC visits.Nine in ten women took iron tablets duringpregnancy. Ninety percent of women’s most recentbirths were protected against neonatal tetanus.Among women who received ANC for their mostrecent birth, 96% had foetal heartbeat checked, 93%had a blood sample taken, 83% had their bloodpressure measured, and 32% had a urine sampletaken.Trends in Maternal Health CarePercent of live births in the five years before the survey100Health facility delivery8060Delivery assistance404 ANC HS*% of women for most recent live birthDelivery and Postnatal CareMore than 9 in 10 births occur in a health facility,primarily in public sector facilities. However, 7%of births occur at home. Women with no educationand those in the poorest households are more likelyto deliver at home. Only 55% of births in 1992 aredelivered in a health facility, compared to 91% in2015-16.Overall, 90% of births are assisted by a skilledprovider, the majority by nurses/midwives. Womenin urban areas, those with secondary or highereducation, those with a first birth, and those living inthe wealthiest households are most likely to receivedelivery assistance from a skilled provider. Skilledassistance during delivery has dramatically increasedfrom 55% in 1992 to 90% in 2015-16.Postnatal care helps prevent complications afterchildbirth. Forty-two percent of women age 15-49receive a postnatal check within two days of delivery,while half did not have a postnatal check within41 days of delivery. Six in ten newborns receive apostnatal check within two days of birth.Page 8 2015 Jodi-Ann Burey VillageReach, Courtesy of PhotoshareMaternal MortalityThe 2015-16 MDHS asked women about deaths oftheir sisters to determine maternal mortality—deathsassociated with pregnancy and childbearing. Thematernal mortality ratio (MMR) for Malawi is 439deaths per 100,000 live births for the seven-yearperiod before the survey. The confidence interval forthe 2015-16 MMR ranges from 348 to 531 deaths per100,000 live births. Between 4 and 5 women age 15-49died during pregnancy, childbirth, or within 42 daysafter childbirth.2015-16 Malawi Demographic and Health Survey
Child HealthVaccination CoverageThree-quarters of children age 12-23 months havereceived all eight basic vaccinations—one dose eachof BCG and measles and three doses each of DPTHepB-Hib and polio vaccine. Rural children are morelikely to have received all eight basic vaccinationsthan urban children (77% versus 70%). Basicvaccination coverage is lowest in Blantyre (63%) andhighest in Mwanza (91%). Basic vaccination coveragehas slightly declined since 2010 when 81% of childrenhad received all basic vaccinations.According to the 2015-16 MDHS, half of childrenage 12-23 months have received all age appropriatevaccinations—one dose each of BCG and measles,two doses of rotavirus, three doses each of DPTHepB-Hib and pneumococcal, and four doses ofpolio. Age appropriate vaccination coverage is 58%in urban areas and 50% in rural areas. By district, ageappropriate vaccination coverage ranges from 32%in Mangochi to 81% in Mwanza. Children from thewealthiest households and whose mothers have morethan secondary education are most likely to havereceived all age appropriate vaccinations.Children age 24-35 months should also receive allage appropriate vaccinations mentioned above plusone more measles vaccination. Only 1 in 10 childrenage 24-35 months have received all age appropriatevaccinations. Age appropriate vaccination coveragefor children age 24-35 months ranges from 1% inKaronga to 32% in Mwanza.Age Appropriate Vaccination Coverageby DistrictPercent of children age 12-23 months whoreceived all age appropriate vaccinesChitipa49% Karonga54%Malawi51%Rumphi60%Mzimba69%Nkhata i65% Lilongwe 49%50% Dedza49% Mangochi ildhood IllnessesIn the two weeks before the survey, 5% of childrenunder five were ill with cough and rapid breathing,symptoms of acute respiratory infection (ARI). Ofthese children, 78% sought treatment or advice.More than 1 in 5 children under five had diarrhoea inthe two weeks before the survey. Diarrhoea was mostcommon among children age 6-11 months (41%).Two-thirds of children under five with diarrhoeasought treatment or advice. Children with diarrhoeashould drink more fluids, particularly through oralrehydration therapy (ORT). While 78% of childrenunder five with diarrhoea received ORT, 13%received no treatment. 2012 Victoria A Smith, Courtesy of Photoshare2015-16 Malawi Demographic and Health SurveyPage 9
Feeding Practices and SupplementationBreastfeeding and the Introduction ofComplementary FoodsVitamin A and Iron SupplementationBreastfeeding is very common in Malawi with 98%of children ever breastfed. Three-quarters of childrenare breastfed within the first hour of life. Only 3%of children who were ever breastfed received aprelacteal feed, though this is not recommended.WHO recommends that children receive nothing butbreastmilk (exclusive breastfeeding) for the first sixmonths of life. Six in ten children under six monthsare exclusively breastfed. Children age 0-35 monthsbreastfeed until a median of 23.0 months and areexclusively breastfed for 3.2 months.Complementary foods should be introduced whena child is six months old to reduce the risk ofmalnutrition. In Malawi, 79% of children age 6-8months are breastfed and receive complementaryfoods.Micronutrients are essential vitamins and mineralsrequired for good health. Vitamin A, which preventsblindness and infection, is particularly important forchildren. In the 24 hours before the survey, 79% ofchildren age 6-23 months ate foods rich in vitaminA. Nearly two-thirds of children age 6-59 monthsreceived a vitamin A supplement in the six monthsprior to the survey.Iron is essential for cognitive development inchildren and low iron intake can contribute toanemia. Two in five children ate iron-rich foods theday before the survey, while 12% received an ironsupplement in the week before the survey. Pregnantwomen should take iron tablets for at least 90 daysduring pregnancy to prevent anemia and othercomplications. One-third of women took iron tabletsfor at least 90 days during their last pregnancy.Use of Iodised SaltIodine is an important micronutrient for physical andmental development. Fortification of salt with iodineis the most common method of preventing iodinedeficiency. Nine in ten households in Malawi haveiodised salt. 2014 Donna Murray, Courtesy of PhotosharePage 102015-16 Malawi Demographic and Health Survey
Nutritional StatusChildren’s Nutritional StatusWomen’s Nutritional StatusThe 2015-16 MDHS measures children’snutritional status by comparing height and weightmeasurements against an international referencestandard. Nearly 4 in 10 (37%) of children underfive in Malawi are stunted, or too short for their age.Stunting is an indication of chronic undernutrition.Stunting is more common in Neno and Mangochi(45%) and less common in Likoma (25%). Childrenfrom the poorest households and whose mothershave no education are more likely to be stunted.The 2015-16 MDHS also took weight and heightmeasurements of women age 15–49. Only 7% ofwomen are thin (BMI 18.5). Comparatively, 21% ofwomen are overweight or obese (BMI 25.0). Womenin urban households are more than twice as likelyto be overweight or obese than rural women (36%vs. 17%). Overweight and obesity is higher amongwomen with more than secondary education (41%)and those in the wealthiest households (36%). Since1992, overweight or obesity has increased from 9% to21% in 2015-16.Wasting (too thin for height), which is a sign of acutemalnutrition, is far less common (3%). In addition,12% of children are underweight, or too thin for theirage. The nutritional status of Malawian childrenhas improved since 1992. In 1992, more than half ofchildren under five were stunted compared to 37% in2015-16.Stunting by DistrictPercent of children under five who are stuntedChitipa33% Karonga28%Malawi37%Rumphi32%Mzimba39%Nkhata 9%40%SalimaMchinji44% Lilongwe 35%37% DedzaBalaka43% 3%Thyolo36%ChiradzuluNsanje33%32%2015-16 Malawi Demographic and Health SurveyAnaemiaThe 2015-16 MDHS tested children age 6-59 monthsand women age 15-49 for anaemia. Overall, 63%of children age 6-59 months are anaemic. Anaemiais more common in children from the pooresthouseholds and those whose mothers have noeducation (both 68%). Anaemia in children hasdecreased since 2004, when 73% of children wereanaemic.One-third of women age 15-49 in Malawi areanaemic. Nearly half of pregnant women areanaemic, while 29% of breastfeeding women and33% of women who are neither pregnant norbreastfeeding are anaemic. Since 2004, anaemiaamong women has decreased from 44% to 33% in2015-16.Trends in Anaemia among Children and WomenPercent of children age 6-59 months andwomen age 15-49 with anaemia2004 MDHS 2010 MDHS 2015-16 MDHS7363634429Children33WomenPage 11
MalariaMosquito NetsAmong all households in Malawi, 57% own at leastone insecticide-treated net (ITN). However, only 24%have enough ITNs to cover each household member,assuming one ITN is used by two people. Amongthe household population, 39% have access to anITN and 34% slept under an ITN the night before thesurvey.Children and pregnant women are most vulnerableto malaria. More than 40% of children under five andpregnant women slept under an ITN the night beforethe survey. Use of ITNs has increased since 2010.ITN use among children under five has increasedfrom 39% in 2010 to 43% in 2015-16, while use amongpregnant women has increased from 35% to 44% inthe same time period.Ownership of, Access to, and Use of ITNsHouseholdsPercent of:Household Population57393424With atWith enoughleast 1 ITN ITNs to coverhouseholdpopulation*With accessto an ITNwithin theirhousehold*Who sleptunder anITN*Assuming one ITN covers 2 people 2008 Paul Jeffrey, Courtesy of PhotoshareIndoor Residual Spraying (IRS)Only 5% of households received indoor residualspraying (IRS) in the year before the survey. IRScoverage is highest in Karonga (34%), Mchinji (28%),and Salima (20%).Intermittent Preventive Treatment ofPregnant Women (IPTp)Malaria during pregnancy contributes to low birthweight, infant mortality, and other complications.To prevent malaria, pregnant women should receiveIPTp (SP/Fansidar during ANC visits). Nearly twothirds of pregnant women took 2 doses of IPTp,while only 30% of pregnant women took 3 doses.Women receiving IPTp has increased since 2004.Management of Malaria in ChildrenIn the two weeks before the survey, 29% of childrenunder five had fever, the primary symptom ofmalaria. Two-thirds of children with fever soughtadvice or treatment, while half had blood taken froma finger or heel stick for testing.Artemisinin combination therapy (ACT) is therecommended drug for treating malaria in childrenin Malawi. Among children under five with feverin the two weeks before the survey who receivedan antimalarial, 92% received Larium (LA), therecommended ACT in Malawi.Page 122015-16 Malawi Demographic and Health Survey
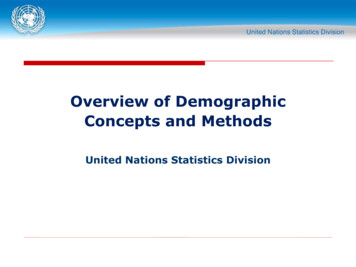
HIV Knowledge, Attitudes, and BehaviourKnowledge of HIV Prevention MethodsMultiple Sexual PartnersSeven in ten women and men know that the riskof getting HIV can be reduced by using condomsand limiting sex to one monogamous, uninfectedpartner. Knowledge of HIV prevention methods ishighest among women and men from the wealthiesthouseholds and those with more than secondaryeducation.Having multiple sexual partners increases the riskof contracting HIV and other sexually transmittedinfections (STIs). A small percentage of women (1%)and 13% of men had two or more sexual partners inthe past 12 months. Among women and men whohad two or more partners in the past year, 27% ofwomen and 30% of men reported using a condomat last sexual intercourse. Men in Malawi have twomore sexual partners in their lifetime than women(4.5 versus 2.1).Knowledge of Prevention of Mother-to-ChildTransmission (PMTCT)Women are slightly more likely than men to haveknowledge of PMTCT. Seven in ten women and 6in 10 men know that HIV can be transmitted duringpregnancy, delivery, and by breastfeeding. About 8in 10 women and men know that HIV transmissioncan be reduced by the mother taking specialmedication.Male CircumcisionTwenty-eight percent of men in Malawi arecircumcised. Male circumcision ranges from 2% inNtchisi to 91% in Machinga. Men from urban areasare more likely to be circumcised than rural men(36% versus 26%).HIV TestingKnowledge of HIV Prevention MethodsPercent of women and men age 15-49 who know thatthe risk of HIV transmission can be reduced by:WomenMen75Using condoms7586Limiting sex to oneuninfected partnerBoth897070Trends in HIV TestingKnowledge of PMTCTPercent of women and men age 15-49 who know that:WomenMenHIV can be transmittedduring pregnancy, delivery,and by breastfeedingTransmission can bereduced by mother takingspecial drugsNearly all women and men know where to get anHIV test. More than 80% of women and 68% of menhave ever been tested for HIV and received theresults. However, 17% of women and 31% of menhave never been tested for HIV. Within the past 12months, 44% of women and 42% of men have beentested and received the results. HIV testing hasincreased since 2004 when only 13% of women and15% of men were ever tested for HIV and receivedthe results. Eight in ten pregnant women with a livebirth in the last two years received HIV testing andcounselling and received the results.Percent of women and men age 15-49 who were evertested for HIV and received their results2004 MDHS 2010 MDHS 2015-16 MDHS697261826851827813Women2015-16 Malawi Demographic and Health Survey15MenPage 13
HIV PrevalenceHIV PrevalenceHIV Testing among HIV Positive AdultsHIV prevalence data were obtained from bloodsamples voluntarily provided by women and meninterviewed in the 2015-16 MDHS. Of the 8,497women and 7,542 men age 15-49 eligible for testing,93%
The use of any method of family planning by married women has dramatically increased from 13% in 1992 to 59% in 2015-16. Similarly, modern method use has increased eightfold from 7% to 58% during the same time period. Family Planning Percent of married women age 15-49 using family planning Any method Any modern method Injectables Implants