Transcription
Injuries of the shoulder girdleby Ntambue Kauta & Stephen RocheLearning objectives1.Red flags in the outpatient setting: infection, malignancy and spinal disorders.2.Red flags in the Orthopaedics ward: fat embolism, compartment syndrome.Paediatrics: Non-accidental injury.IntroductionThe shoulder girdle consists of threeanatomical joints, the sternoclavicular,acromioclavicular and glenohumeraljoints. Acute injuries to the shoulder girdlemay result in a traumatic dislocation ofone of the joints or a fracture. Theseinjuries are usually due to either highenergy impact (fall, road traffic accidents,sports injuries and so on) or low energyfall in patients with weak bones.Sternoclavicular dislocationsPosterior dislocations pose a risk of injuryto vital structures behind the sternum andunder the clavicle. Therefore, all patientswith posterior sternoclavicular jointdislocation must be admitted to the traumaward and prepared for surgery. A closedreduction manoeuvre must be attemptedby a team of cardiothoracic andorthopaedic surgeons. If the closedreduction method reduction fails, the teamwill proceed to an open reduction andsurgical stabilisation of the joint.This is a rare injury and can be dividedinto anterior or posterior dislocations.Acromioclavicular dislocationsCompared to an anterior dislocation, aadults, often resulting from falls fromposterior dislocation has a higher risk ofheights or contact sports injuries.damage to retrosternal structures such asA threatened skin overlying the clavicle andThis is a common injury affecting youngthe subclavian vessels. The patient mayneurovascular compromise is a red flag forpresent with a hoarse voice, stridor, orurgent referral. After the initial assessment,compromised neurovascular status of thethe treatment will depend mainly on theupper limb due to pressure on vitalseverity of the displacement of the clavicle.structures by the retrosternally positionedPatients with a prominent step deformityclavicle. Dedicated sternoclavicular jointwithradiographic views of both joints must beradiographs should be immobilised in aobtained and will show the dislocation.sling and referred for orthopaedic review.upto100%displacementonPatients with 100% displacement usuallyManagementIn the acute setting, anterior dislocationsare treated with a simple arm sling or acollar and cuff for two weeks and earlyreturn to function.warrant surgical management.
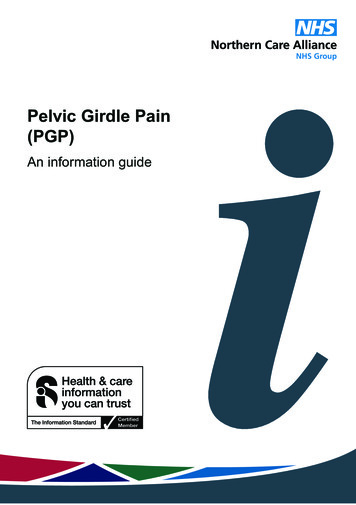
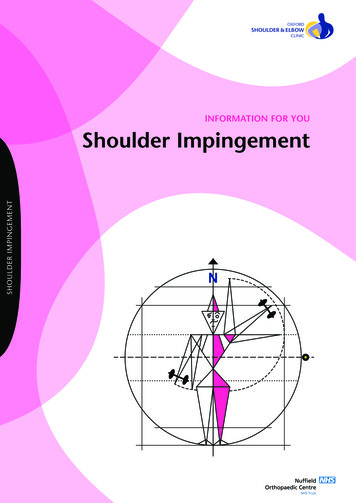
At two weeks, patients should be reassessedfor residual instability or, most importantly, atraumatic cuff tear (ideally with ultrasoundor MRI) which should be urgently addressedsurgically.Other rare forms of shoulder dislocationsinvolve acute traumatic inferior dislocationX-ray shows an acromioclavicular dislocationwith more than 100% displacement.and multidirectional instability, often becauseof generalised ligamentous laxity.Shoulder dislocationsThe glenohumeral shoulder dislocation is themost common in the human body. Patientsyounger than 30y may develop recurrentinstability, and those older than 40 are likely topresent with an acute cuff tear or avulsionfracture of the greater tuberosity.AssessmentA clinical examination must exclude brachialplexus, axillary nerve and vascular injury. OnX-rays of anterior dislocations, the humeralhead displaces medially and inferiorly.Posterior dislocations can be easily missedbecause only physicians aware of the ‘lightbulb’ sign can make the correct diagnosis onAP radiographs. Besides AP and Y-view(lateral X-ray of the shoulder), a modifiedaxillary view is essential to assess this injury.ManagementInline traction (Hippocratic method) underconscious sedation should be used to relocatethe shoulder. The neurovascular assessmentmust be repeated and documented after therelocation.Fracture-dislocations should haveorthopaedic input before attempted reduction.AP X-ray of acute shoulder dislocation with anassociated fracture of the greater trochanter.All acute dislocations are treated initially withan emergency room or sports field relocationfollowed by a course of physical therapy.Patients presenting with recurrent dislocationsor patients younger than 20 years of age andinvolved in contact sports, should be referredto an orthopaedic surgeon for reassessmentand further treatment.
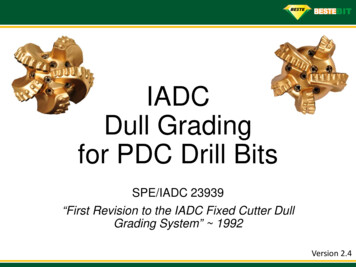
Clavicle fracturesMost clavicle fractures will respond wellvalgus or varus deformity of more than 30degrees).to immobilisation in an arm sling for 4to 6 weeks and an early gradual returnto function. Full healing is to beexpected in 8–12 weeks.Absolute indications for surgery areopen fracture, skin tenting, neurovascularinjury requiring repair and symptomaticnon-unions after conservative treatment.Relative indications for surgery aremultiple fractures, and patients’ workor leisure requirements.ReferencesApley and Solomon’s System ofOrthopaedics and Trauma 10thEd. A Blom et al, (Eds) CRCPress, 2017.Bhandari, Mohit, ed. Evidence-basedorthopedics. Vol. 77. John Wiley &Sons, 2011.Rockwood and Green’s: Fractures inAdults, 7th ed. J H Beaty et al, (Eds)Philadelphia: Lippincott Williams. X-Ray showing a midshaft claviclefracture with 100% displacement andshortening.Proximal humerus fracturesThese are fractures proximal to the surgicalneckline. The majority of these injuries canbe treated conservatively in an arm slingor collar and cuff. Surgical indicationsinclude open fractures, fracture-dislocation,displaced articular segment split fractures,pathological fractures and fractures whichhave failed conservative treatment (100%displacement, less than 50% apposition),
Rockwood and Green's: Fractures in Adults, 7th ed. J H Beaty et al, (Eds) Philadelphia: Lippincott Williams. X-Ray showing a midshaft clavicle fracture with 100% displacement and shortening. Proximal humerus fractures . These are fractures proximal to the surgical neckline. The majority of these injuries can be treated conservatively in an .