Transcription
Lecture Notes: Orthopaedics and Fractures
Lecture NotesOrthopaedics andFracturesT DuckworthBSc (Hons), MBChB (Hons), FRCS (Eng)Emeritus Professor of OrthopaedicsUniversity of SheffieldC M BlundellMB, ChB, BMedSci (Hons), FRCS (Eng), MD, FRCS (Tr&Orth)Northern General HospitalSheffield, UKFourth editionA John Wiley & Sons, Ltd., Publication
This edition first published 2010, 2010 by T Duckworth and CM BlundellPrevious editions: 1980, 1984, 1995Blackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishing program has beenmerged with Wiley’s global Scientific, Technical and Medical business to form Wiley-Blackwell.Registered office: John Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UKEditorial offices: 9600 Garsington Road, Oxford, OX4 2DQ, UKThe Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, UK111 River Street, Hoboken, NJ 07030-5774, USAFor details of our global editorial offices, for customer services and for information about how to apply for permissionto reuse the copyright material in this book please see our website at www.wiley.com/wiley-blackwellThe right of the authors to be identified as the authors of this work has been asserted in accordance with theCopyright, Designs and Patents Act 1988.All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in anyform or by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UKCopyright, Designs and Patents Act 1988, without the prior permission of the publisher.Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not beavailable in electronic books.Designations used by companies to distinguish their products are often claimed as trademarks. All brand names andproduct names used in this book are trade names, service marks, trademarks or registered trademarks of their respectiveowners. The publisher is not associated with any product or vendor mentioned in this book. This publication isdesigned to provide accurate and authoritative information in regard to the subject matter covered. It is sold on theunderstanding that the publisher is not engaged in rendering professional services. If professional advice or otherexpert assistance is required, the services of a competent professional should be sought.Library of Congress Cataloging-in-Publication DataDuckworth, T.Lecture notes. Orthopaedics and fractures / T. Duckworth, C.M. Blundell. – 4th ed.p. ; cm.Rev. ed. of: Lecture notes on orthopaedics and fractures / T. Duckworth. 3rd ed. c1995.Includes index.ISBN 978-1-4051-3329-61. Orthopedics–Handbooks, manuals, etc. 2. Fractures–Handbooks, manuals, etc. I. Blundell, C. M. (Chris M.)II. Duckworth, T. Lecture notes on orthopaedics and fractures. III. Title. IV. Title: Orthopaedics and fractures.[DNLM: 1. Orthopedic Procedures–Handbooks. 2. Fractures, Bone–Handbooks. WE 39 D836L 2010]RD732.5.D83 2010616.7–dc222009046372ISBN: 9781405133296A catalogue record for this book is available from the British Library.Set in 8 on 12 pt Stone Serif by Toppan Best-set Premedia LimitedPrinted and bound in Singapore12010
ContentsContributors viPreface to fourth edition viiPreface to first edition viii131415Infections 100Metabolic diseases of bone 109Examination of the musculoskeletalsystem 116Part 1: General Principles123456789101112Musculoskeletal structures and function 3Soft-tissue injuries and healing 12Nerve injuries and repair 20Fractures and healing 25Fractures—principles of management 32Complications of fractures 44Major trauma 49Congenital and developmental conditions 52Generalized orthopaedic conditions 66Inflammatory conditions 74Degenerative conditions 87Neoplastic conditions of bone and softtissue 92Part 2: Regional Orthopaedics161718192021222324The forearm, wrist and hand 123The elbow 139The shoulder and upper arm 148The spine 157The pelvis 172The hip and thigh 176The knee and lower leg 188The foot and ankle 201Orthopaedic techniques 218Appendix 233Index 237v
ContributorsStephen BostockConsultant Orthopaedic Hand SurgeonSheffield Orthopaedics LtdSheffield, UKAshley ColeConsultant Orthopaedic Spinal SurgeonSheffield Orthopaedics LtdSheffield, UKRichard GibsonConsultant Orthopaedic SurgeonSheffield Teaching Hospital NHS TrustSheffield, UKBob GrimerThe Royal Orthopaedic HospitalBirmingham, UKAndrew HamerConsultant Orthopaedic SurgeonSheffield Orthopaedics LtdSheffield, UKviPaul HaslamConsultant Orthopaedic SurgeonDoncaster and Bassetlaw Hospitals NHS TrustDoncaster, UKStan JonesConsultant Orthopaedic SurgeonSheffield Orthopaedics LtdSheffield, UKDavid StanleyConsultant Orthopaedic SurgeonSheffield Teaching Hospitals NHS TrustSheffield, UKSimon TillConsultant RheumatologistSheffield Teaching Hospitals NHS TrustSheffield, UKRob TownsendConsultant MicrobiologistDepartment of MicrobiologyNorthern General HospitalSheffield, UK
Preface to fourth editionMedical training is constantly changing. Surgicaltraining is becoming shorter and the decisionabout which branch to follow is being asked at anevermore junior level. It is only possible to makean informed career choice by having a sufficientgrasp of the relevant speciality and, wherever possible, having some exposure to it.Orthopaedics is a changing speciality. Subspecialization has become commonplace and the‘general’ orthopaedic surgeon is now rare. Thisbook attempts to introduce most aspects of orthopaedics at a level which will satisfy medical students, students of professions allied to medicineand general practitioners alike.This fourth edition has been rewritten to make iteasier to study the basis of orthopaedics (Part 1)and then to refer to each region in turn (Part 2).With the advent of sub-specialization, this is howthe subject is often now encountered. The regionalsection is further sub-divided into four areas:examination, adult pathology, paediatric pathology and trauma.We hope we have achieved our goal in creating abook which is broad enough in scope to cover mostpathologies whilst covering the more commonconditions in sufficient depth to allow a comprehensive understanding.T DuckworthC M Blundellvii
Preface to first editionAt first sight there would appear to be little difficulty in compiling a short textbook of orthopaedics and fractures to meet the needs of medicalstudents, general practitioners and others with anon-specialist interest in the subject. They are alllikely to require a quick and reliable source of reference and some practical advice on management.But how much material, how much detail and howmuch practical advice?Many medical schools have reduced the timeavailable for the study of disorders of the musculoskeletal system. The medical student is now luckyif he/she can gain experience in the techniques ofclinical examination, let alone become familiarwith those common orthopaedic conditions whichoccupy so much of the average general practitioner’s time and encroach on every branch ofmedicine.It would be a short textbook indeed whichcovered only the contents of this type of course.Students often complain that they are given noguidance as to how far their reading shouldtake them beyond the confines of their limitedclinical experience. They often ask in desperationfor a syllabus or a list of reading material: howmuch do we need to know? Unfortunately,although examiners may be prepared to confinethemselves within pre-determined limits, patientsrarely do so. They present with obscure problems,or, worse still, common problems in familiarguises. No matter how well he/she has beentaught and has understood the principles ofdiagnosis and management, no textbook canprovide the new doctor with what will becomehis/her most valuable asset—experience. It canhowever provide him/her with other people’sexperience and also with something almost equallyvaluable—an awareness of what are the possibilities. Without this awareness, a diagnosis can rarelybe made.viiiIn the absence of clear guidance from the medicalfaculties about what their end-product, the newlyqualified doctor, is supposed to be, it seemed reasonable to try to produce a book which wouldattempt to provide answers, albeit often brief andincomplete ones, to most of the questions theinterested and intelligent student and postgraduate would be likely to ask about the subject.In doing so, emphasis has been placed on theprinciples of diagnosis and management and onclassification. It is hoped that the latter will be anaid to understanding relationships and alsoperhaps to memory. Common conditions havebeen allocated relatively more space, and somedetails of the management of such conditions,which might be of value to junior staff, areincluded, with short sections on orthopaedic andoperative procedures. Rarities are either excludedor simply receive a brief mention to make thestudent aware of their existence. Inevitably, somesections will appear too condensed and others toodetailed. The section on ankle fractures, forexample, is perhaps more appropriate for a traineeorthopaedic surgeon than a student, but here, as inother places, it was felt that the subject couldbecome almost meaningless if less detail wasincluded.The layout of the book may be found convenientby some readers, irrational and perhaps irritatingby others. This particular arrangement has beenchosen so that answers will be easy to find, embedded in related information which will make thesubject more of a whole. The regional chaptersprovide an alternative approach to the same information, and cross-references have been providedto avoid repetition.The content is, of course, the author’s choice,based on experience of what has been found usefuland of interest to students. Orthopaedics is astrongly clinical subject with a high visual content.
Preface to first editionThis is reflected in the relatively large number ofillustrations. X-rays are so much a part of the worldof orthopaedics that it is difficult to imagine thespecialty without them, and wherever possiblethese have been used to illustrate the various conditions. Nevertheless, some experience is requiredin their interpretation, and where this could be aproblem diagrams have been substituted for theirextra clarity.Finally, and in response to suggestions fromstudents, an appendix has been added, givinguseful pathological and clinical data for rapidreference.If this volume proves useful on the wards and inthe clinics, and stimulates an interest in a fascinating subject, it may justify adding to the rising tideof published material which threatens to overwhelm students and practising doctors alike.ix
Part 1General Principles
Chapter 1Musculoskeletal structuresand functionThe skeletal structuresModern orthopaedics is concerned with thediagnosis and management of disorders of themusculoskeletal system, that is the skeleton andthe soft tissues associated with it. Worldwide,orthopaedic surgeons deal with both injuriesof the musculoskeletal system, particularly fractures, as well as non-traumatic conditions. Subspecialization within orthopaedics is increasinglycommon and can be organized by patient age(e.g. paediatric orthopaedics), by region (e.g. hipsurgery) or by condition (e.g. rheumatoid surgery).Alternatively, orthopaedics can be considered interms of the structures with which it is primarilyconcerned. A knowledge of the anatomy, physiology and pathology of these structures and tissuesforms a logical starting point for studying the clinical aspects of the subject.The connective tissuesThe connective tissues of the body are composed ofcells embodied in a matrix which varies in its quantity and composition. The cells can be categorizedby the nature of the intercellular material, of whichthere are three types:Bony—osteoid (produced by droblasts) Fibrous—collagenoustissue (producedfibroblasts). bybyStructureIn each case the matrix is mainly composed of acomplex mixture of proteoglycans and glycoproteins, forming a ground substance in which isembedded a meshwork of fibrils, mostly of collagen, a protein. At least four genetically differenttypes of collagen are now recognized—bone contains Type I and hyaline cartilage Type II. Skin contains Types I and III and, being a convenient tissuefor biopsy, is used for the study of certain collagenrelated bone diseases. Elastin, a different protein, isfound within skin and to a lesser extent in tendon.Matrix disorders cause a wide variety of clinicalmanifestations. For example, in the so-called‘mucopolysaccharoidoses’ (see p. 68), an enzymedeficiency interferes with the breakdown of largemucopolysaccharide molecules, which accumulatein the tissues causing widespread abnormalities.Connective tissues grow by cell proliferation anddeposition of intercellular material.PhysiologyLecture Notes: Orthopaedics and Fractures, 4e.By T Duckworth and CM Blundell. Published 2010 byBlackwell Publishing.The connective tissues are by no means inertand they play an important role in biochemicalprocesses in the body.3
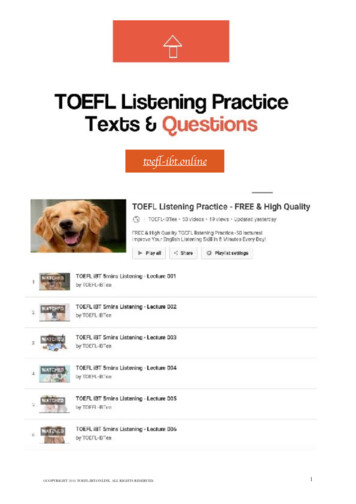
Chapter 1 Musculoskeletal structures and functionGround substance is an important water-binding agent and acts as an ion-exchange resin in controlling the passage of electrolytes. Its deposition isinfluenced by many factors, such as hormones andvitamins, and its composition reflects abnormalities in the supply of these factors.Cartilage ‘turnover’ is the subject of muchresearch. It is controlled by a complex interactionof different enzymes, some of which promote andothers suppress chondrocyte function. Thus, balanced synthesis and degradation of the ground substance has been shown to continue throughout life.Bone is known to play a vital role in metabolism,mainly because of its calcium and phosphatecontent. These minerals enter into the formationof crystals of hydroxyapatite and their depositionis sensitive to many influences. Diseases such asrickets, osteomalacia and hyperparathyroidismare associated with dramatic changes in bonedevelopment.Demineralization of bone results in loss of bonestrength and may be caused by diminished matrixformation, inadequate calcification or bone resorption. The latter occurs as a result of the activity ofspecial cells—osteoclasts—which remove both theorganic and inorganic components. The radiographic appearances of loss of density are similarwhatever the cause of the demineralization, andthese appearances give rise to the term ‘osteoporosis’, although specific scans (dual energy X-rayabsorption [DEXA] scan) are required to make adefinitive diagnosis of osteoporosis.BoneMacroscopic structureA long bone is characteristically tubular withexpanded ends and is remarkably strong for itsweight. The shaft is called the diaphysis and thezone adjacent to the epiphyseal line is the metaphysis (Fig. 1.1). This is the part of the developing bonethat is most likely to be the seat of disease, probably because it is the most metabolically active areaand has the greatest blood supply. Damage to, orabnormal development of, the epiphyseal plateitself is likely to result in growth disturbance.4The short bones consist of a cancellous coresurrounded by a layer of cortical bone, partlycovered by articular cartilage. They contain redmarrow in their trabecular spaces and the vertebralbodies are important sites of blood formationthroughout life.A normal bone can resist large compressiveforces and considerable bending stresses, and onlybreaks when subjected to considerable violence. Itmay, however, be weakened by disease and canthen fracture as a result of minimal trauma. Suchpathological fractures are often orientated transversely across the bone.The bones form fixed points for muscle attachments and their periosteal sheaths blend with thecollagen of the tendons and ligaments.Microscopic structureBone consists of osteoid, which is resilient and isheavily infiltrated with calcium salts, giving ithardness and strength. The mechanism of mineralization is not well understood. The mineral ismainly deposited in crystalline form as hydroxyapatite, but there is also an amorphous phase whichis found particularly in newly formed bone. It isworth noting that various ions, such as strontium,fluoride and lead, can enter the crystal lattice ofbone mineral.A normal bone is composed of concentric cylinders of matrix with cells lying in lacunae betweenthe layers, the whole forming a ‘Haversian system’.In the hard cortex, the Haversian systems arepacked tightly together; in the spongy or cancellous bone, they are more loosely arranged (Fig.1.2). The bony trabeculae are structured and orientated to withstand the stresses of weight-bearingand muscle activity, obeying Wolff’s Law. Theinterstices of the cancellous bone and the hollowcentres of the shafts of long bones are filled withmarrow. Haemopoiesis occurs in the marrowthroughout the bones in the child, but in theadult is confined to the short bones, particularlythe vertebral bodies, and to the ends of the longbones.Each bone is ensheathed by fibrous periosteumwith an underlying layer of osteoblasts, and is
Musculoskeletal structures and function Chapter 1Articular cartilageProximal epiphysisEpiphyseal lineProximal metaphysisSpongy boneMedullary canalNutrient foramenCortexEndosteumDiaphysisPeriosteumDistal metaphysisDistal epiphysisArticular cartilageFigure 1.1 Macroscopic structure ofbone.vascularized from the periosteum and by one ormore nutrient arteries penetrating the cortex.Bone formationThe bones develop initially in early intrauterinelife as condensations of mesenchymal tissue in theaxis of the limb (Fig. 1.3a), and by the sixth weekthe connective tissue cells have started to lay downcartilage to form the shape of the future bone (Fig.1.3b). At the centre of the cartilage mass, the cellshypertrophy and apparently die, and with theingrowth of vascular connective tissue, the matrixcalcifies and eventually ossifies (Fig. 1.3c). Thisprocess spreads along the bone (Fig. 1.3d), so thatit eventually consists of a bony shaft with cartilaginous ends (Fig. 1.3e) which become the sites ofsecondary ossification centres (Fig. 1.3f). The intervening or epiphyseal cartilage remains until maturity as the growth point for bone length, theproliferating cartilage cells on the diaphyseal sideforming into columns and undergoing a series of5
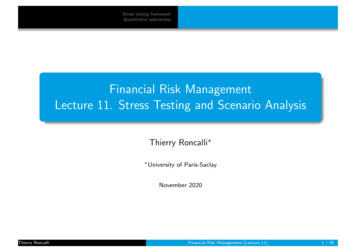
Chapter 1 Musculoskeletal structures and functionHaversian MedullaFigure 1.2 Microscopic bone structure.changes, eventually ‘ballooning’ as the zone of vascularization reaches them and ossification of thematrix begins. This results in gradual growth of theepiphysis away from the centre of the shaft.Growth in width occurs by deposition of noncartilaginous subperiosteal bone and the wholebone is constantly remodelled as the child grows.The earliest bone to be laid down is often called‘woven bone’ because its histological structureshows the fibrils to be randomly distributed, unlikethe regular lamellar structure of mature bone.Some bones develop entirely by intramembranousossification, with no intermediate cartilage stage,the clavicle and the skull being examples.Growth does not occur equally at the two ends ofa long bone. It is more active, for example, at theends farthest from the elbow and nearest to theknee (growth is often described by ‘to the elbow Igrow, from the knee I flee’). Diseases such as osteo6myelitis and tumours are noticeably more commonat these sites. The spongy ends of the bone have acomplex architecture and it is here that the trabeculae can be seen to follow the lines of greatest stress(Fig. 1.4).Remodelling of bone continues throughout life,but particularly during growth and after fracturehealing. In children, even severe residual deformities can be corrected fully, with the possible exception of rotational deformities; this capacity forremodelling is less in the adult and, although thebone smoothes itself out, it is usually possible tospot the site of a fracture many years later (Fig. 1.5).CartilageThis varies in appearance and physical characteristics, depending on the predominant type of fibriland the density of the matrix. Two types of fibril,
Musculoskeletal structures and function Chapter llsEpiphyseal lineCell columnsCalcificationOssification(f)Figure 1.3 Bone growth and development.collagen and elastin, are found in varying proportions. Three types of cartilage are normallyrecognized.1 Hyaline cartilage The pre-ossified epiphysesand the articular surfaces both consist of hyalinecartilage, which is indistinguishable in the two byordinary histological techniques, but has differentproperties and, of course, different functions in thetwo tissues.2 White fibro-cartilage is found mainly inmidline structures such as intervertebral discs andsymphyses. The collagen content is much greaterthan in hyaline cartilage and the fibres are muchmore obvious. This type of cartilage has the abilityto withstand strong tension and bear heavy compressive loads.3 Yellow or elastic fibro-cartilage is found in thenasal and aural cartilages, and contains the highestproportion of elastin.Cartilage grows by direct proliferation of the cellswith pericellular deposition of matrix, but evenduring rapid active growth relatively few cells canbe seen to be dividing. The capacity of hyalinecartilage to regenerate and repair itself is strictlylimited, which means that damage to an articularsurface can have long-lasting consequences. There7
Chapter 1 Musculoskeletal structures and functionis some evidence that intrinsic mechanisms ofrepair can be supplemented by ingrowth and metaplasia of periarticular collagenous tissue, but repairof any but the smallest defect is seldom complete.Figure 1.4 Upper end of femur to show trabeculae.Figure 1.5 Remodelling after a fracture.8Fibrous tissueFibrous tissue is widespread throughout the bodyand consists mainly of collagen fibres with relatively little matrix.Disorders of collagen metabolism are beingextensively studied because of their dramaticeffects on body structure and development. Theseconditions are sometimes called ‘true collagendiseases’, as opposed to the non-developmentaldiseases of collagen, such as rheumatoid arthritis.Osteogenesis imperfecta (see p. 66), is an exampleof an inherited disorder of collagen metabolism,mainly affecting the structure and strength ofbone.Collagen growth is an important aspect ofgeneral body development and fibroblasts are frequently to be seen proliferating and laying downcollagen fibres. This is particularly the case in anysituation where repair of tissues is required. Theusual end-result of repair, the scar, consists almostentirely of collagenous material. In situationswhere there is continuing damage to the tissues,with concomitant repair, the scar tissue formedcan be extremely dense. As it matures, collagenousscar tissue tends to contract, sometimes producingdistortion and obstruction of internal structures orcontractures of skin and joints. Occasionally, thehealing of a skin wound may be complicated
Musculoskeletal structures and function Chapter 1by the formation of over-exuberant scar tissue,producing a wide and thickened scar knownas ‘keloid’. This is more common in races withblack skin.LigamentsThese may be either discrete structures or thickenings of the joint capsule. Being necessary for jointstability, they are strong and are orientated to resistspecific stresses. They are, however, occasionallyruptured, either completely or partially, and aredifficult to restore when damaged. A partial ruptureis known as a sprain or strain, and usually healscompletely.JointsThe function of a limb is heavily dependent on thesmooth working of the joints, and joint diseasesare common and troublesome.Three types of joint are usually recognized.1 Fibrous joints or syndesmoses. As the namesuggests, in this type of joint the bones are connected by a continuous band of fibrous tissue, as isthe case with the sutures of the skull. These jointsare strong and not readily disrupted, but they allowlittle movement.2 Cartilaginous joints or synchondroses. Theseconsist of a cartilaginous band joining the bones.This may be hyaline, as between some of the skullbones, in which case ossification usually occurs atmaturity. Secondary cartilaginous joints consist ofa mass of fibro-cartilage lying between two thinplates of hyaline cartilage.3 Synovial joints. This type of joint allows thegreatest mobility. The joint surfaces are coveredwith hyaline cartilage and the joint is enclosed bya fibrous capsule which is usually attached close tothe edge of the articular surface. It is lined by a vascular synovial membrane which secretes synovialfluid. This fluid is a remarkable substance whichperforms a nutritive function and has importantlubricating properties. Articular cartilage, apartfrom its deepest layer, derives most of its nutritionfrom the synovial fluid which must, therefore,have access to the whole articular surface. There issome evidence that degenerative joint disease maybe, at least partly, due to an interruption in the freeflow of this fluid.Some joints contain fibro-cartilaginous discspartly separating the joint surfaces. The menisci ofthe knee are examples of this and they have beenshown to have an important stress-distributingfunction.Articular cartilage, normally smooth and elastic,may be pitted or eroded by disease or completelyworn away to reveal the underlying bony cortex.The earliest stages of this process are known as‘fibrillation’. The articular cartilage becomes irregular and tends to fray and split. To some extent,this phenomenon is age-related, but it does notoccur uniformly throughout the joints and variesin its extent from individual to individual. It isessentially a focal change, and there are certainsites where it is common, particularly thoseareas which rarely contact the opposing articularsurface and/or where loads are high, such as thepatella. In certain circumstances, this conditionprogresses to fully developed osteoarthritis (seeChapter 11).Blood supply and innervation of jointsAll joints have a free blood supply with manyanastomozing arteries. An operation on a majorjoint without a tourniquet provides a gooddemonstration of joint vascularity. There is afine plexus of lymphatics within the synovialmembranes.The nerve supply of a joint is the same as that ofthe overlying muscles moving the joint and theskin over their insertions (Hilton’s Law). Most ofthe nerve end-organs lie in the joint capsule, butmuscle and tendon end-organs are equally important for proprioception. Autonomic nerves alsoreach the joint, mainly with the blood vessels, andcontrol the blood supply and perhaps the formation of synovial fluid.The protective and proprioceptive functions ofnerves supplying joints are vital to the normalfunctioning of a joint, which rapidly disintegratesif this protection is lost (Charcot’s joint).9
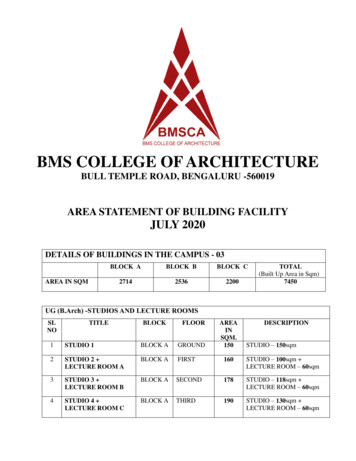
Chapter 1 Musculoskeletal structures and functionMusclesThe functions of joints and muscles are closelyinterrelated. Not only are muscles important formoving the joints, but their co-ordinated action isessential for joint stability. This is very evident inparalytic conditions where the lack of stability mayhave to be compensated by the use of externalsplints.Skeletal muscle is composed of fibres whoselength varies from a few millimetres to about30 cm. Each fibre contains many nuclei embeddedin its syncytium and the fibre itself is built up ofmany myofibrils, each of which consists of units ofthe proteins actin and myosin. These are arrangedin interlocking bands. They give the fibre its characteristic cross-sections, and are the contractileelements of the muscle.The form of a muscle determines its power andcontractility. If the fibres are arranged parallel tothe line of pull, the contractility is greatest: wherethere are many fibres arranged obliquely to the lineof pull, the power is greater but the ability toshorten is less.Nerve supply to musclesThe nerve enters the muscle at the motor point,which is usually constant and is the point at whichelectrical stimulation is most effective. The smallerbranches of each nerve fibre supply a variablenumber of muscle fibres, each junction beingcalled a motor end-plate. Where fine control isneeded, as with the small muscles of the hand, the(a) Tendon sheathnumber of muscle fibres supplied by each nervefibre is small, whereas more coarsely innervatedmuscles may have one nerve fibre dividing tosupply over a hundred motor end-plates. Afferentfibres derive from muscle spindles and are essential for the feedback mechanisms controllingcontraction.Muscles have many actions, sometimes functioning as prime movers, at other times asco-ordinating antagonists, synergists and cooperating muscles. Many of their so-called ‘voluntary’ activities are concerned with posture and areessentially unconscious.Tendons and bursaeMost muscles are attached to the bone ends by atendon, which may be a few millimetres or manycentimetres long. Many of the larger tendons movewithin a fibrous sheath, which has a synoviallining (Fig. 1.6a).Tendons do not resist pressure very well and arefrequently separated or protected from their underlying bones by thin-walled cavities containingsynovial fluid. Some of the larger tendons containa bone within their substance at the place wherethey cross a joint and have to bear considerablestresses. These are known as sesamoid bones.Examples are the patella and the sesamoids underthe first metatarsal head. They have articular cartilage on their deep surfaces (Fig. 1.6b).Small sacs or bursae are often found overlyingbony prominences. They may be fairly constantanatomical structures, like those overlying the(b) Sesamoid(c) BursaFigure 1.6 Tendons and bursae. The darker blue areas indicate: (a) synovial sheath, (b) hy
book attempts to introduce most aspects of ortho-paedics at a level which will satisfy medical stu-dents, students of professions allied to medicine and general practitioners alike. This fourth edition has been rewritten to make it easier to study the basis of orthopaedics (Part 1) and then to refer to each region in turn (Part 2).